
Abstract
Objective:
The aim of this study was to investigate the effects of fiber-reinforced composite base material on fracture resistance and fracture pattern of endodontically treated maxillary premolars restored with endocrowns using two different resin nanoceramic computer-aided design and computer-aided manufacturing (CAD/CAM) restorative material.
Methods:
Forty extracted sound maxillary premolars with an occlusal reduction of 2 mm above the cementoenamel junction (CEJ) was performed following root canal treatment. Mesial interproximal box was prepared for each tooth at the margin of the CEJ and randomly distributed into four groups (n = 10) as follows: Group A, no resin build-up in the pulp chamber; Group B, 2 mm of fiber-reinforced composite (FRC) build-up (EverX Posterior, GC).; Group C, no resin build-up in pulp chamber; Group D, 2 mm of FRC build-up. Groups A and B were prepared with resin nanoceramic (RNC) consisting ceramic nanofillers (Lava Ultimate 3 M ESPE), while Group C and D were prepared with RNC consisting ceramic nanohybrid fillers (Cerasmart GC Corp). All samples were subjected to 1,200,000 chewing cycles (1.6 Hz, 50 N) and 5000 thermal cycles (5°C–55°C) for artificial aging on a chewing simulator with thermal cycles (CSTC). Samples that survived the CSTC test without being damaged were subjected to a load-to-fracture test.
Results:
The highest mean fracture strength was found in Group D (936.0 ± 354.7) and lowest in Group A (684.2 ± 466.9). Fracture strength was higher in groups where FRC was used as a base material than plain restorations. However, there were no significant differences between the Lava and Cerasmart groups with and without FRC (p > 0.05). Most of the samples were irreparably fractured under CEJ.
Conclusion:
Using short FRCs as a resin base material did not significantly improve fracture resistance. Cerasmart and Lava blocks had similar fracture resistance and fracture pattern.
Introduction
Teeth that require endodontic treatment usually lose a large volume of tissue due to extensive caries, replacement of extensive old restorations and trauma; in addition, during endodontic treatment, dentin loss occurs, particularly in preparing the access cavity by removing the pulp chamber roof. 1 Access cavity preparation may further weaken the previously weakened structure. Therefore, these teeth are prone to fracture under occlusal forces. 2
Many endodontically treated teeth (ETTs) are lost mostly because of coronal restoration failures 3 and cusp fractures. 4 Fuss et al. 5 stated that the three most common reasons for ETT extractions are endodontic failure (21.1%), nonrestorable teeth (43.5%), and vertical root fractures (10.9%). Therefore, the long-term prognosis of ETTs depends not only on the quality of the endodontic treatment but also on the selection of the appropriate restoration type and biomaterial that protects and strengthens the remaining tooth structure against fracture.6–8
Full-crown restorations and post- cores have been used in the traditional method to restore teeth with severe tissue loss.9,10 However, due to the loss of radicular dentin, posts may weaken the residual root structure, and iatrogenic root perforations may also occur. Furthermore, it has been demonstrated that removing healthy tissue during the preparation of traditional crowns impairs the biomechanical properties of the remaining dental tissue.11–13 With the development of adhesive systems and biomaterials, endocrowns have been suggested as a conservative treatment option as opposed to traditional crowns as they have the advantage of preserving the peripheral enamel. 14
To ensure the long-term survival of ETTs, the clinician should select the best design and material that maximizes function and esthetics while minimizing fractures.15,16 With their remarkable optical properties, computer-aided design and computer-aided manufacturing (CAD/CAM) materials with improved mechanical properties may be suitable for restoring ETTs. 17 Ceramic restorations have grown in popularity due to their esthetics, biocompatibility, and durability. However, these restorations have some significant disadvantages, such as the possibility of brittle catastrophic tooth fractures and antagonist wear.18,19 Resin nanoceramic (RNC) CAD/CAM materials were created to combine the benefits of nonbrittle polymers with the outstanding visual appeal of ceramics.20,21 RNC CAD/CAM materials have been recommended for use in the fabrication of endocrowns due to their similar modulus of elasticity to dentin. They act as stress absorbers under pressure, reducing stress peaks within the root dentin and the restoration-tooth interface.22,23
EverX posterior (GC Europe), a short fiber-reinforced composite (FRC) composed of resin, e-glass fibers, and inorganic fillers, 24 was designed to mimic dentin’s stress absorption capacity. It is intended for use in high-stress areas, prevents crack formation and propagation and can limit the risk of fractures. 25
The roof of the pulp chamber is completely removed while performing endodontic access cavity, to localize all root canal orifices and provide direct access to the apical foramen 26 But removing dentin roof could play a role in predisposing to fracture under occlusal forces in premolar and molar teeth. 27 In a morphologic study regarding the anatomy of maxillary second premolars, in 92.8% of premolars, the pulp chamber roof was determined at cementoenamel junction (CEJ). 28 Therefore short FRC may be an appropriate material to compensate the dentin loss in this region. However, the implications of utilizing short FRCs mimicking dentin-roof under CAD/CAM-fabricated maxillary premolar restorations have not yet been investigated. In addition, the use of RNC endocrowns for maxillary premolars is not well documented. 29
Thus, the purpose of this study was to investigate the effect of FRC base material on fracture prevention and the pattern of endocrowns restored by two different types of RNC. This study’s first null hypothesis was that the FRC base material would have no effect on the load-bearing capacity and fracture pattern of teeth restored with RNC endocrowns. The second null hypothesis was that no differences in load-bearing capacity or fracture pattern would be observed between the endocrown materials.
Materials and methods
The study was approved by the Ethics Committee of Istanbul Aydın University (B.30.2.AYD.0.00.00-050.06.04/243). A total of 40 extracted permanent maxillary second premolars were used. This study excluded premolars that had been restored, cracked/chipped, or showed signs of caries. Premolars with a single visible root canal in the preoperative radiograph and similar dimensions in the CEJ were included (mean dimensions; buccolingual: 7 ± 1 mm, mesiodistal: 5 ± 0.5 mm, and root length of 13 ± 1 mm).
Endodontic treatment
Root canal instrumentation was performed by rotary nickel-titanium files (Protaper Universal, Dentsply, Maillefer, Ballaigues, Switzerland), and the F2 size file was selected as the master apical file. The canal was irrigated with 1% NaOCl after each file, followed by the application of paper points to dry out the root canal. The canals were obturated by using a single cone technique.
Cavity preparation and cementation
The ETT was occlusally reduced 2 mm above the CEJ. The same operator used an angled (8°–10°), rounded diamond bur on standardized cavities with a cervical width of 2 mm, and measurements were performed with a graded periodontal probe. Each tooth was prepared with mesial interproximal boxes (Figure 1) (4 mm in length, 1 mm in width) at the CEJ and classified into four groups (n: 10). Following cavity preparation, all preparations were embedded up to 2 mm below the CEJ in an acrylic self-polymerizing resin, and the teeth embedded in the acrylic resin were scanned with an intraoral scanner (Cerec Omnicam, Sirona Dental Systems, Germany). For each crown design, an intact extracted tooth was used as the master model of the biogeneric copy (Cerec 4.0).

Presentation of standardized cavity preparation.
Samples were restored in four different ways (Figure 2 and Table 1).
Group A – No resin build-up in the pulp chamber. The endocrowns were prepared by CAD/CAM with Lava Ultimate RNC (Figure 2(a)).
Group B – Build-up of 2 mm FRC (EverX Posterior). The endocrowns were prepared by CAD/CAM with Lava Ultimate RNC (Figure 2(b)).
Group C – No resin build-up in the pulp chamber. The endocrowns were prepared by CAD/CAM with Cerasmart RNC (Figure 2(c)).
Group D – 2 mm FRC build-up (EverX Posterior). The endocrowns were prepared by CAD/CAM with Cerasmart RNC (Figure 2(d)).
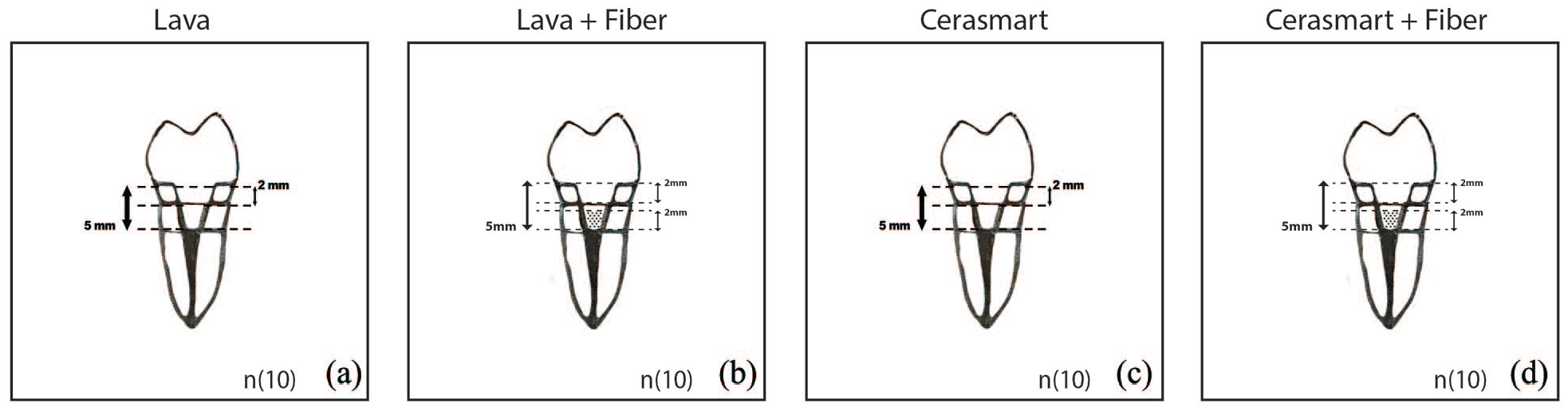
Schematic presentation of tooth restoration in each group: (a) no resin build-up in the pulp chamber and fabricated by Lava Ultimate, (b) 2 mm FRC (EverX Posterior) was placed as a base material and fabricated by Lava Ultimate, (c) no resin build-up in the pulp chamber and fabricated by Cerasmart, (d) 2 mm FRC (EverX Posterior) was placed as a base material and fabricated by Cerasmart.
Materials used in this study.

Groups A and C: The central retention cavity depth was 5 mm from the cervical margin; Groups B and D:2 mm EverX Posterior build-up, and the cavity depth was 3 mm from the cervical margin.
To cement the endocrowns, (Figure 3) each restoration’s intaglio surface was sandblasted with aluminum oxide for 5 s before being immersed in an ethanol bath for 60 s and dried. Intaglio surfaces were coated with a single-bond adhesive (3M ESPE Neuss, Germany) for 20 s and then thinned with air. The prepared teeth were etched with 37% phosphoric acid etching gel for 15 s, rinsed for 20 s using a water syringe and blow-dried for 5 s. After 20 s of application, the single-bond universal adhesive (3M ESPE Neuss, Germany) was fully dried for 5 s, and an LED light was used to polymerize the single-bond universal adhesive based on the manufacturer’s protocol. All endocrowns were cemented with continuous finger pressure using self-adhesive resin cement (RelyX™ Ultimate resin, 3M ESPE Neuss, Germany). Excess material was removed with a microbrush, and the restoration margins were coated with a glycerin gel to avoid oxygen inhibition during the polymerizing step. For 20 s, each surface was irradiated using a bluephase light curing device (Ivoclar Vivadent AG, Schaan, Liechtenstein). All samples were tested for durability using a chewing simulator with thermal cycles CSTC device (Analitik Medikal ve Mühendislik A, Gaziantep, Turkey). All samples were loaded for 1,200,000 cycles using a 50 N compressive with a frequency of 1.6 Hz. Chewing simulation with these parameters could simulate up to 5 years of oral usage. 30 Steel balls with a diameter of 4.5 mm were used as the antagonist. The thermal cycle parameters used in conjunction with the chewing cycles were as follows: samples were immersed in 5°C and 55°C water for 30 s at 10 s intervals.

Photograph of Lava Endocrown restoration.
After CSTS, the fracture resistance of the surviving crowns was determined by mechanically loading the crowns until failure using a universal testing machine (AGS-X series, Shimadzu, Japan). The force was applied on the center of the crowns using 5 mm rounded steel tips.
At the triangular junction containing the buccal and lingual cusps, the load was applied in the direction parallel to the tooth axis with a round metal tip (Figure 4). To determine the fracture mode, fracture loading values were recorded, and tooth fragments were observed. Four fracture patterns were identified:
Type I: The vertical fracture split the tooth and the restoration (Figure 5(a)).
Type II: Fracture of the restoration (Figure 5(b)).
Type III: Fracture of both the tooth and restoration (Figure 5(c)).
Type IV: Complete separation of the crown (Figure 5(d)).

Positioning and axial compressive loading of the sample.
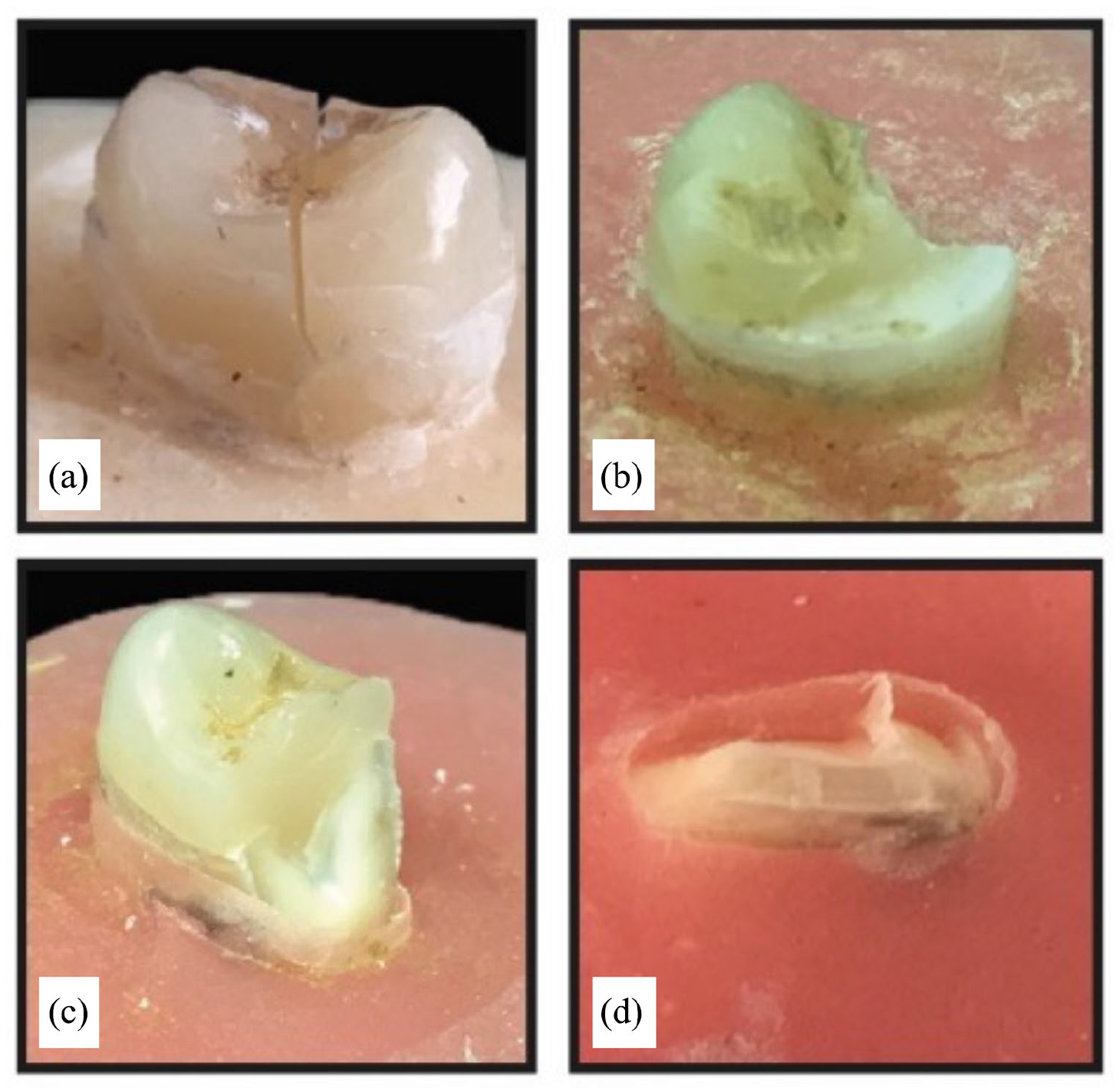
(a) The vertical fracture splits the tooth and the restoration (b) Fracture of the restoration (c) Fracture of both teeth and restoration (d) Complete separation of the crown.
Failures above the CEJ were classified as “repairable,” while those occurring below the CEJ and extending to the root were classified as “irreparable.”
Statistical analysis
The data were analyzed using the IBM SPSS Statistics 22 program. The distribution of the parameters was evaluated with the Shapiro-Wilk test, and it was determined that the parameters were in accordance with a normal distribution. Two-way ANOVA was used to evaluate the effect of material and fiber usage on fracture strength. Significance was evaluated by a threshold of p < 0.05.
Results
Only one sample from Group B (Lava + Fiber) was found to be coronally fractured after the CSTC test. A two-way ANOVA was performed to analyze the effect of material and FRC on the fracture strength (Table 2). The highest mean fracture strength was found in Group D (Cerasmart + Fiber) (936.0 ± 354.7), and the lowest was found in Group A (Lava) (684.2 ± 466.9) (Table 3). Fracture strength was higher in groups where FRC was used as a base material than in plain restorations. However, there were no significant differences between the Lava and Cerasmart groups with and without FRC (p > 0.05).
Evaluation of the effect of material and fiber usage on fracture strength.

Two-way ANOVA.
Mean fracture load values and standard deviations (SD) of groups restored with and without FRC base material.
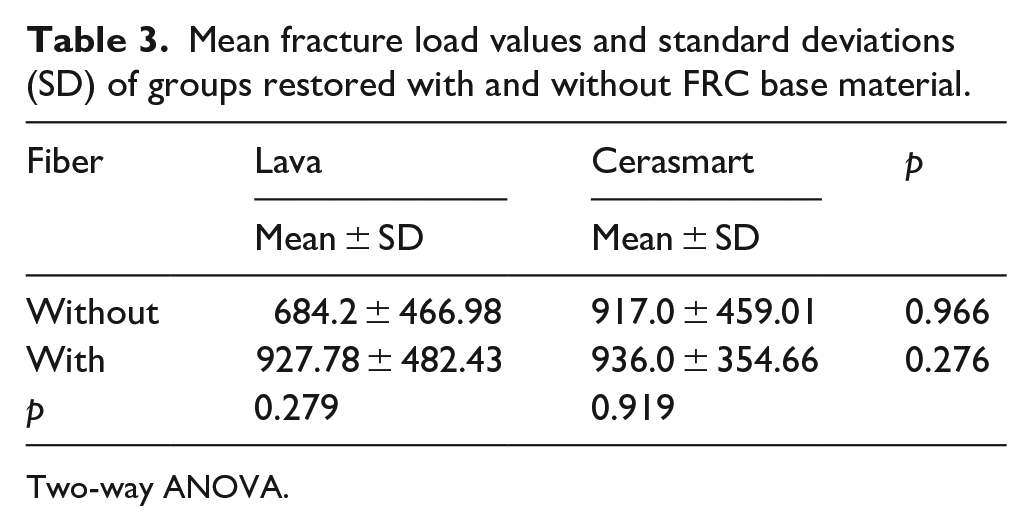
Two-way ANOVA.
Four fracture patterns were identified (Figure 5). Thirty-one of 39 samples (79.48%) were irreparably fractured under the CEJ (Table 4). Type III fractures were observed in the majority of the samples.
Fracture types among groups.

Discussion
The purpose of this study was to investigate the durability of endodontically treated premolars that had been restored with two different resin nanoceramic CAD/CAM blocks with and without an FRC base. The results of this study showed that there were no significant differences in load-bearing capacity or fracture pattern between the groups. Consequently, the null hypothesis was accepted.
Maxillary premolars with significant coronal loss are the teeth that have been primarily affected by biomechanical failure due to poor structural integrity. 31 During chewing, due to the anatomical shape of maxillary premolars, a tendency for separation of cusps can occur, and post placement is not usually indicated because of their tiny and curved roots. 32 Therefore, a scenario mimicking a severely damaged maxillary premolar is planned to evaluate the effectiveness of FRC and endocrowns.
RNC blocks to replace dentin and absorb stresses have been introduced to the dental market. 33 In the majority of studies, resin nanoceramic or lithium disilicate ceramics have been used to construct endocrowns.34–37 Endocrowns constructed of resin to restore premolars showed increased resiliency to fractures and reduced failure rates compared to endocrowns made of lithium disilicate. This outcome could be explained by the resin elasticity, which is comparable to that of dentin. This elasticity would allow force to be better distributed over the bonding surface of premolars, improve the resistance to fracture and reduce catastrophic failure rates. 38 In the current study, CAD/CAM RNC was chosen as the material for endocrown restoration because of its biomechanical advantages and low elastic modulus.
RNC blocks can be constructed from a polymer matrix reinforced by ceramic fillers, such as nanofillers (Lava Ultimate 3M ESPE) or nanohybrid fillers (Cerasmart GC Corp). 39 Goujat et al. 40 evaluated the mechanical characteristics and internal adaptability of polymer-infiltrated ceramics in comparison to two resin nanoceramics (Lava and Cerasmart) and a lithium disilicate ceramic. According to the researchers, Cerasmart exhibited significantly higher flexural strength (216.5 MPa) than Lava Ultimate (172.8 MPa). Compared to Cerasmart (1.2 MPa.m½), Lava Ultimate (1.6 MPa.m½) had substantially higher fracture toughness values. While both are RNCs, their behavior was not similar. Therefore, we decided to compare the effectiveness of two commonly used RNCs based on the load-bearing capacity and fracture pattern.
FRC has been proposed to improve the strength and toughness of composite restorations, support residual tooth tissue, and prevent fractures. 41 FRC contains randomly oriented short E-glass fibers. The presence of fibers in resin decreases polymerization shrinkage, 42 and the random organization of fibers provides a uniform stress distribution, which is essential for maximum reinforcement. 43 Furthermore, FRC can prevent crack propagation and act as a load-bearing barrier under high occlusal forces. 44
Several studies have indicated that teeth restored with SFC as a bulk core under composite restorations had higher load-bearing capacity.45–48 Contrary to these studies, there were no significant differences in load-bearing capacity between the single-structure (without FRC) and bistructured (with FRC) groups in the current study. Such differences could be due to the thickness of the FRC core, cavity design, severity of the aging process and CAD/CAM material.
Although many studies have investigated the load bearing effect of FRCs under composite restorations of ETTs, only a limited number of studies have investigated the effect of FRCs under CAD/CAM materials.48–51 Rocca et al. 51 compared the fracture resistance and fracture pattern of endodontically treated molars restored with resin nanoceramic CAD/CAM material (Lava Ultimate) either with an endocrown without fiber reinforcement or overlays with different types of fiber reinforced cavities. It was found that reinforcement did not improve fracture resistance, and all samples fractured under the CEJ in a nonrepairable manner. Consistent with their study, no statistically significant findings were observed between groups in terms of fracture resistance with and without short fiber reinforcement. Furthermore, 79.48% of samples under the CEJ fractured in a nonrepairable manner.
Huda et al. 50 stated that endocrowns had better fracture resistance than inlay and onlay restorations. The authors compared the fracture resistance of various Cerasmart inlays, onlays, and endocrown restorations in endodontically treated mandibular molars. In their study, inlay and onlay restorations were filled with either FRC or a flowable composite in the pulp chamber (G-aenial Universal Flo). Although the fracture resistance was higher in the flowable light-cured composite than in the FRC, no significant difference was found. Contrary to their study, our results demonstrated that fracture resistance was higher in samples where EverX Posterior (FRC) was used as a base material in the pulp chamber compared to samples without FRC. However, no statistically significant differences were found.
Garoushi et al. 49 investigated the effect of the short fiber composite (SFC) core and the thickness ratio of the SFC on the fracture behavior of different posterior restorations. Five direct overlay restorations were made with varying thicknesses of SFC-core (EverX Flow), and four groups of CAD/CAM restorations were made with a 2-mm layer of SFC-core or without fiber reinforcement. Likewise, in our study, the load-bearing capacity of the restorations with a 2-mm SFC core (bistructured) and those from plain restorative materials showed no statistically significant difference. The researchers demonstrated that using flowable SFC as a reinforcing base can result in more repairable failures in extensive direct and indirect restorations. In the current study, however, most of the samples below the CEJ were fractured irreparably. Such differences in fracture patterns between the studies could be attributed to the exclusion of the aging process in Garoushi’s study and the severe aging protocol applied in our study. Additionally, the morphology of premolars, which are more prone to fracture than molars, may have been influential.
In the present study, to better reflect the clinical scenario, artificial aging was performed, which may affect both the fracture resistance and pattern of samples. Because the coefficient of thermal expansion of the restorative materials and the tooth structure differs during thermocycling, stress is produced at the adhesive interface. 52 The mechanical fatigue simulation in which 1,200,000 load cycles were applied to the samples. They are designed to simulate restoration stress after a maximum of 5 years of intraoral use. 30 Two different and commonly used nanoceramic composite materials (Lava Ultimate CAD/CAM and Cerasmart CAD/CAM) were tested in a chewing simulator. The mean masticatory forces during mastication and swallowing in humans range from 3 to 72 N. 53 Therefore, a loading force of 50 N was used. Since the chewing load was applied to the endocrowns, cusps were not modeled, and only uniform anatomical restorations were made.
The same operator performed all experimental work to ensure uniform sample preparation and testing. To extrapolate therapeutically relevant data, all restorations were prepared using a biogeneric copy. The fracture resistance of samples that survived CSTS testing without being damaged was evaluated as one of the test parameters. Only one fiber-reinforced Lava sample failed to withstand 1,200,000 chewing cycles, simulating 5 years of function. 30 According to our findings, resin nanoceramic restorations could be promising because they can withstand repetitive occlusal stress, such as that found in the mouth.
Post-core systems and full crown restorations are traditionally indicated during the restoration of ETT having excessive loss of dental tissue.8,9 In recent years, fiber-reinforced posts (FRPs) having the modulus of elasticity similar to that of dentin have been frequently used to increase the retention and resistance of the restoration after root canal treatment 54 Gallicchio et al. 55 investigated fracture resistance and fracture patterns of three types of fiber posts used in restoring maxillary premolars subjected to similar fatigue cycling (1,000,000) and static tests of the current study. The mean fracture strength of both Lava and Cerasmart groups with and without Short FRC was lower than both sound teeth (1909) and fiber post-core restorations of Gallicchio’s study. The fracture resistance difference between the studies may depend on the cavity design, restoration type and restoration material. The tissue loss of the samples in the present study was more than in the aforementioned study.
In the present study, although the results were not statistically significant, higher fracture resistance was observed in the fiber-reinforced groups than in the plain groups. In particular, the Lava group without fiber reinforcement showed the least fracture resistance, and the increase in fracture resistance when fiber was added was greater in the Lava group (684–927 N) than in the Cerasmart group (917–936 N). These results could be attributed to the small sample size. Further in vitro studies with large sample sizes are needed, especially to evaluate the effect of FRC bases under Lava material in endocrown restoration of severely damaged premolar teeth. In addition, quite a high standard deviation of fracture load values was detected in the current study. This could be due to the time difference of extracted teeth. Teeth extracted for orthodontic reasons within the last 6 months were used as test samples.
By absorbing occlusal stresses, the periodontal ligament provides critical support for the tooth. 56 The periodontal ligament has a thickness of 0.1–0.3 mm. 57 According to Soares et al., 58 the periodontal ligament may influence the fracture resistance and pattern of fracture of the restoration. Even though previous studies have simulated periodontal ligaments,59,60 the lack of periodontal ligament simulation due to difficulties in standardizing thickness and stability is a limitation of this study. Another limitation of the study was the limited sample size. In the current study, extracted sound teeth were used, but in a clinical situation, mostly an endodontically treated tooth would have been restored before endodontic therapy. Tooth walls could have had irregular shapes and thicknesses. Furthermore, the oral cavity simulation was performed with distilled water rather than artificial saliva.
Conclusion
According to the study’s findings, the Lava and Cerasmart groups with and without FRC withstood severe artificial aging. Cerasmart and Lava restorations had similar fracture resistance and fracture patterns with and without FRC. With an increased sample size, it could be recommended to compare implications of utilizing short FRC under resin and ceramic CAD/CAM-fabricated restorations for further studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.