
Abstract
Background:
To maintain and enhance the wound healing effects of mesenchymal stem cells (MSCs), a scaffold for hosting MSCs is needed, which ought to be completely biocompatible, durable, producible, and of human source.
Objective:
To build a cell-extracellular matrix (ECM) complex assembled by human umbilical cord mesenchymal stem cells (HuMSCs) and to investigate its clinical potentials in promoting wound healing.
Method:
HuMSCs were isolated and expanded. When the cells of third passage reached confluency, ascorbic acid was added to stimulate the cells to deposit ECM where the cells grew in. Four weeks later, a cells-loaded ECM sheet was formed. The cell-ECM complex was observed under the scanning electron microscopy (SEM) and subjected to histological studies. The supernatants were collected and the cell-ECM complex was harvested at different time points and processed for enzyme-linked immune sorbent assay (ELISA) and mRNA analysis. The in vivo experiments were performed by means of implanting the cell-ECM complex on the mice back for up to 6 months and the specimens were collected for histological studies.
Results:
After 4 weeks of cultivation with ascorbic stimulation, a sheet was formed which is mainly composed with HuMSCs, collagen and hyaluronic acid. The cell-ECM complex can sustain to certain tensile force. The mRNA and protein levels of vascular endothelial growth factor-α (VEGF-α), hepatocyte growth factor (HGF), keratinocyte growth factor (KGF), and transforming growth factor-β1 (TGF-β1) were remarkably increased compared to monolayer-cultured cells. The implanted cell-ECM complex on mice was still noticeable with host cells infiltration and vascularization on 6 months.
Conclusion:
Our studies suggested that HuMSCs can be multi-cultivated through adding ascorbic stimulation and ECM containing collagen and hyaluronic acid were enriched around the cells which self-assembly formed a cell-ECM complex. Cell-ECM complex can improve growth factors secretion remarkably which means it may promote wound healing by paracrine.
Introduction
Intractable chronic wounds, characterized by dysfunctional features, such as excessive quantities of pro-inflammatory cytokines, proteases, reactive oxygen species (ROS), and senescent cells, as well as the persistent infection, 1 are usually resistant to conventional therapy regimes. A number of preclinical and clinical investigations have shown that MSC therapy can help cure non-healing wound. Its benefits include isolation from adult or fetal tissue sources (e.g. bone marrow, adipose tissue, and umbilical cord), a large in vitro expansion capacity, immunosuppressive activity and differentiation multipotency.2–5 MSCs are assumed to be promising measures in dealing with the problems by its potentials in suppressing inflammatory reactions, improving granulation formation, reepithelialization, and being involved in ECM metabolism.6–8 MSCs can settle on damaged skin and take part in the healing process. Based on the study, BM-MSCs migrated into skin wounds9,10 and released bioactive components that attracted additional repair cells from the host animals.11,12 Wu et al. 13 also have revealed that MSCs could differentiate into keratinocytes at the wound bed. Since bone marrow-derived cells (BM-MSCs) have been the subject of the majority of the research into MSC biology to date, BM-MSCs are usually recognized as the primary cell source for potential clinical applications. 14 But BM-MSCs are difficult to obtain and have a much lower yield than other resources. Furthermore, when Kern et al. 15 evaluated the proliferative capacities of MSCs from other origin, they found that BM-MSCs had the lowest proliferative capacity compared to other resources. Despite some success in endeavor, it is a less desirable source for cell-based therapy due to the high amount of inflammatory cells and the low frequency of stem cells in the bone marrow.
Among the MSCs of different sources, HuMSCs are becoming thought highly for its non-invasive harvest, lack of ethical issuses, low immunogenicity, lack of controversy and good expandability. 16 The HuMSCs keeps young with higher vitality and shorter doubling time, 17 and are from full-term deliveries of donors who are healthy and screened to be free of contagious or genetic diseases, which promised the safety and the quality of the cell source. HuMSCs could enhance the proliferation and migration of fibroblasts through paracrine actions and hence promote wound healing. 18 Moreover, HuMSCs were confirmed to produce more pro-angiogenic and tissue repair-related molecules than the MSCs from bone marrow or adipose tissue.19,20
Persistent inflammation might make chronic wounds trapped in inflammatory state. 21 Inflammatory cells release growth factors that are essential for the development of new tissue, while they also emit a variety of toxic mediators, such as proteases and ROS, which are damaging to the surrounding tissues 22 and make the microenvironment for engrafted cells highly hostile. 23 Due to the cellular damage generated by enzymatic treatment during harvesting 24 and the lack of cell-ECM adhesion, locally injected MSCs are known to be lost significantly soon after transplantation.25,26
It is necessary to increase cells engraftment efficiency. The locally administered cells may need carriers or scaffolds to ensure the viability and sustained functioning of the cells on the wounds. 27 By sustaining cell-cell connections and cell surface proteins, ECM can increase cell density and cell survival at the transplantation site. 28 Numerous biocompatible biomaterials, such as cell sheets, 29 cell-loaded hydrogels, 30 and composite scaffolds, that imitate the properties of ECM are being developed in the disciplines of dermal filling and wound healing care, as well as being used to improve delivery efficiency and therapeutic efficacy.
The ideal cell scaffold should be durable, inexpensive, and readily available, as well as having high biocompatibility and the ability to be loaded by live cells, and it should not injure the targeted tissue.31,32 With the MSCs seeded in, the scaffold should not only fill the defects, but also facilitate the cells to exert repair and regenerating roles and hopefully be completely biocompatible and could be integrated into the host tissues. MSCs not only increased the production of collagen and elastin by fibroblasts,33,34 they themselves possess strong potentials of synthesizing and depositing ECM.35,36 In our earlier research, we found that the HuMSCs seeded in a gelatin sponge kept remodeling the scaffold by depositing collagen and hyaluronic acid while degrading the original gelatin structure. 37 However, HuMSCs still needed scaffolds to be multi-cultured.
In this study, we tried to build a fully self-assembled cell-ECM complex which can get rid of the influence on degrading scaffolds. After observing the ultrastructure of the cell-ECM complex, the histological experiments further confirmed the formation of cell-ECM complex. The mRNA analysis and ELISA assay were performed to examine the secretion of growth factors. In vivo experiments, we expected to explore if the cell-ECM complex was compatible with in vivo environment and finally integrate into the host tissue. Based on the above data, we assumed the cell-ECM complex may be applied in chronic wounds through paracrine.
Materials and methods
Preparations of HuMSCs from human umbilical cords
Before parturition, Informed consent forms and ethical permissions were authorized by the Ethics Committee of Shantou University Medical College (SUMC). The Department of Obstetrics and Gynecology, the Second Affiliated Hospital of SUMC, help us collected umbilical cords from full-term (38–40 weeks) healthy pregnancies (excluding HIV, hepatitis and syphilis) through cesarean section. HuMSCs were extracted from the umbilical cord, cultivated and characterized as described previously. 38 Briefly, Wharton’s jelly was separated after the blood vessels in the umbilical cord were removed and cut into 1–2 mm2 pieces, which were then attached to a culture dish. High glucose Dulbecco’s modified Eagle’s medium (DMEM, Gibco, Thermo Fisher Scientific, Inc., USA) containing 2% fetal bovine serum (Gibco, USA), basic Fibroblast Growth Factor (bFGF, Zhuhai Essex Bio-Pharmaceutical Co., Ltd., China), transferrin(Sigma, Sigma-Aldrich, Co., USA), insulin(Sigma, Sigma-Aldrich, Co., USA), and selenium acid(Aldrich, Sigma-Aldrich, Co., USA) was prepared to add into culture plates. 39 When cells attained confluency, they were divided and passaged. The cells of passage three were used in the experiments. Culture medium was changed every 2 days.
Preparations of self-assembled cell-ECM complex
HuMSCs were seeded in the 10 cm culture dish with cell density of 5x105 cells/dish. As soon as HuMSCs reached confluency, 50 ug/ml ascorbic acid was added to the culture medium to induce the cells to proliferate and deposit ECM. The culture medium was changed every 2 days for 4 weeks. By day 28, the cell-ECM complex was harvested for implantation on mice and the samples were also processed for histological study and SEM. HuMSCs were grown as the control group using same medium exchange period as the experiment groups, but without ascorbic acid stimulation.
Histological examination of Cell-ECM in vitro
After 28 days culture, the cell-ECM complex was formed successfully. The samples were obtained and fixed in 4% paraformaldehyde overnight, dehydrated at different concentrations of ethanol (70%, 80%, 90%, 95%, and 100%), embedded in paraffin, and sectioned at 5 μm. Hematoxylin-eosin (HE, Beyotime, China), Van gieson (VG, Leagene, China) and Alcian blue (AB, Maixin, China) stains were applied to the sections after they were rehydrated and dewaxed. The images were taken using BX51 Olympus microscope (Tokyo, Japan).
Cell-ECM complex for SEM
In order to characterize the ultrastructure of cell-ECM complex, the prepared samples were examined by SEM at 10 kv and 1500-fold magnification. To begin, the materials were fixed for 3 h at 4°C in 2.5% glutaraldehyde, and then rinsed three times with PBS, each for 15 min. After dehydrating the samples in increasing percentages of ethanol (30%, 50%, 70%, 90%, and 100%) for 10 min, the specimens were air-dried overnight at room temperature. Finally, the objects were sputter-coated with gold and analyzed by the Gemini 300 field emission scanning electron microscope (ZEISS, Germany).
Real-Time polymerase chain reaction (RT-PCR) analysis
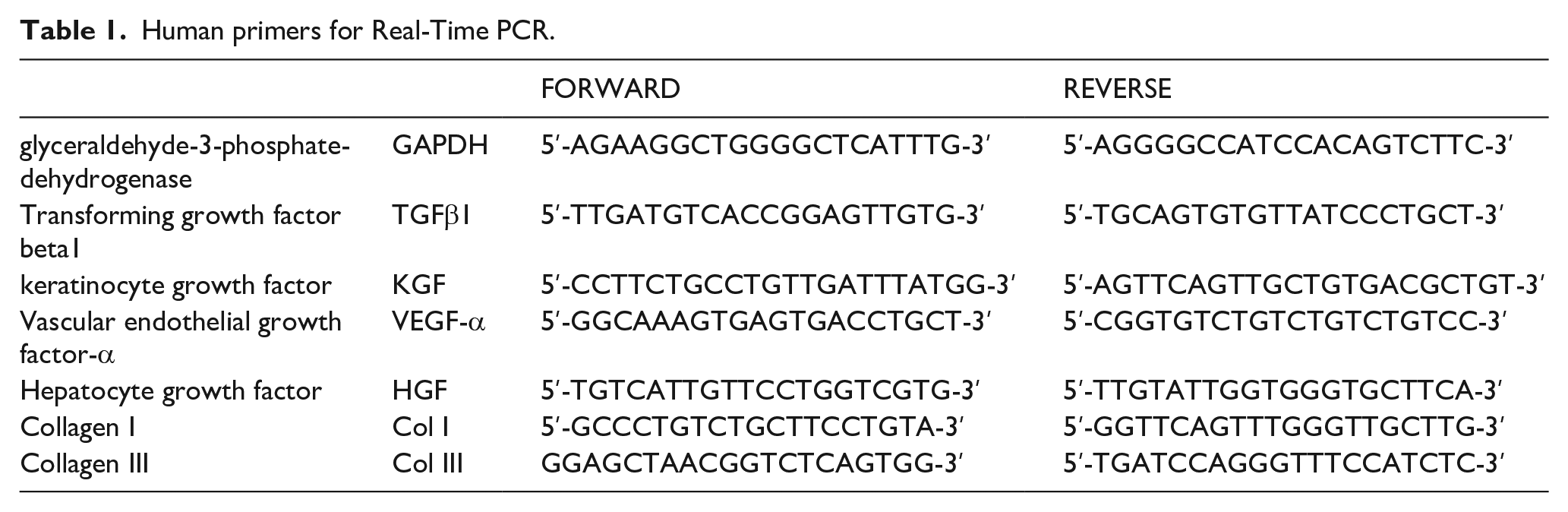
For RNA analysis, HuMSCs were separated into control group and experiment groups. When cells reached confluency, they were collected and used as the control group. When the cells were treated with ascorbic acid for 3, 7, 14, and 28 days, the cells were harvested and employed as the experiment groups. Total RNA extraction was performed using TRIzol reagent (Invitrogen, Carlsbad, CA, USA), and the DNase I (Sigma-Aldrich, USA) according to the manufacturer’s instructions. The concentration of the total RNA was determined with a NanoDrop-2000C spectrophotometer (Thermo Scientific, Waltham, MA, USA). cDNA was synthesized in a C1000 Touch™ Thermal Cycler (BIO-RAD, USA). PrimeScript™ RT Master Mix (TaKaRa) was used for reverse transcription. RT-PCR was performed using SYBR® Premix Ex Taq™ mix in a BioRad CFX96™ Q-PCR Detection System. Glyceraldehyde-3-phosphate-dehydrogenase (GAPDH) levels were measured in parallel with target genes as an internal control. The primers used for RT-PCR are shown in Table 1. The ΔΔCt method was used to measure the relative gene expression and fold changes. The results were obtained from three separate assays, with each carried out in duplicate.
Human primers for Real-Time PCR.
ELISA analysis of growth factors levels
The supernatants were divided into two groups. Supernatants from control group were collected when cells came to confluency. Supernatants from experiment groups were harvested after giving cells ascorbic acid for 3, 7, 14, and 28 days. Supernatants from control group and experiment groups were centrifuged at 1500 rpm for 15 min to remove floating cells and cell debris and allotted and stored at −80°C for Elisa analysis. The secreted cytokines including VEGF-α, KGF, HGF and TGF-β1 in the supernatants were identified in duplicates using the ELISA assay according to the manufacturer’s protocols. Growth factor levels were estimated using three independent experiments and four parameter logistic curves.
The subcutaneous implantation of cell-MSC complex
The in vivo study was approved by the Animal Care and Use Committee at SUMC. The prepared cell-ECM complexes were harvested and washed with saline for three times to remove the components in culture medium. The cell-ECM complex was cut into 2.5 mL of small fragments in a tube and then was implanted subcutaneously on the backs of KM male mice (6 weeks) purchased from the Laboratory Animal Center of SUMC. The injection was accomplished with 1 ml syringes (Henan piaoan group CO., LTD, China) coupled with 21 G needles. The mice were sacrificed at 2 and 6 months respectively after operation, and the samples were harvested, photographed and processed for histological studies.
Histological study of the cell-MSC complex in vivo
According to histological studies in vitro as mentioned above, cell-MSC complex implants acquired from mice were fixed by 4% paraformaldehyde overnight, and then dehydrated and embedded in paraffin. 5 μm thick tissue was sectioned and stained with HE, AB, and VG stains. The Images were observed and recorded by microscope.
Statistical analysis
The data were provided as the mean ± standard deviation, with one-way analysis of variance (ANOVA) used to compare between groups. The control group was compared to other experiment groups in terms of the mRNA and protein levels of growth factors. P < 0.05 was considered statistically significant.
Results
Preparation of cell-ECM complex
When HuMSCs reached confluency, the spindle shaped cells arranged in fascicular and whorled (Figure 1(a)). After adding ascorbic acid for 3 days, the cells were much more tightly packed and overlapped, with elongated cell branches (Figure 1(c)). Under an inverted contrast microscope, the cells were further overlapping and starting to form a three-dimensional structure after being consistently ascorbic stimulated for 7 days (Figure 1(e)). By day 28, a cell-ECM complex that was semitransparent and capable of withstanding pull and stretch to a certain extent without rupturing had developed (Figure 1(f)). HuMSCs multiplied quickly in the three-dimensional structure, gradually obscuring the cell’s shape and morphology. Compared to the control group which wasn’t treated with ascorbic acid, different changes were observed, such as the lengthened cell distance, branched cells, polygonal cells, and apoptotic cells (Figure 1(b) and (d)).

The observation of morphology of HuMSCs self-assembled complex. The microscopic view of HuMSCs when cells reached confluency (Figure 1(a)). Morphological changes of HuMSCs after adding ascorbic acid for 3 days (Figure 1(c)) and 7 days (Figure 1(e)) were captured under the microscope. HuMSCs without treated with ascorbic acid were observed at day 3 (Figure 1(b)) and day 7 (Figure 1(d)). By day 28, a semitransparent and elastic cell-ECM complex was formed (Figure 1(f)). Scale bar, 200 μm.
Histological study and the ultrastructure of the cell-ECM complex
The cell-ECM complex was stained with HE, demonstrating that the cells were embedded in the matrix (Figure 2(a)). Collagen that stained pink and hyaluronic acid that stained blue were identified using VG and AB stains (Figure 2(b) and (c)). SEM imaging showed various fiber bundles with bead-like particles attached, which may have been HuMSCs connected to collagen fibers (Figure 2(d)).

Histological assessments and ultrastructure observation of the cell-ECM complex (28 days). HuMSCs distribution (black arrows) were presented in the cell-ECM complex by HE stain (Figure 2(a)). Plenty of collagen (green arrows) were stained pink in the cell-ECM complex by VG stain (Figure 2(b)). A lot of hyaluronic acid (yellow arrows) were also detected by AB stain (Figure 2(c)). SEM image showed the HuMSCs (white arrows) attached around the collagen fiber bundles (Figure 2(d)). Microscope scale bar, 100 μm, SEM scale bar, 10 μm.
Investigation of wound healing-related growth factors at mRNA and protein levels
To examine the changes of growth factors in cell-ECM complex, cells and supernatants were collected for RT-PCR and ELISA analyses. When compared to the control group, HGF, VEGF-α, KGF and TGF-β1 levels in terms of mRNA and excreted protein levels almost increased starting on day 3, virtually reached high levels by day 7, and maintained at a high level until day 28 (Figures 3(a)–(d) and 4(a)–(d)). Otherwise, collagen I mRNA expression peaked on day 3 while collagen III expressed its highest level on day 7 (Figure 3(e) and (f)). The results demonstrated that ascorbic acid can stimulate the upregulation of mRNA expression and increased levels of HGF, TGF-β1, VEGF-α, and KGF secretion. They also suggested that HuMSCs in cell-ECM complex continuously deposited ECM might assist in maintaining the production of growth factors at a high level.

mRNA expression of cell-ECM complex secreted growth factors. Six growth factors were measured with RT-PCR after adding ascorbic acid, including HGF (a), VEGF-α (b), KGF (c), TGF-β1 (d), collagen type I (e), and type II (f). The control group wasn’t treated with ascorbic acid while the experiment groups were treated with ascorbic acid. The cells of control group and experiment groups which were harvested at day 3, day 7, day 14, and day 28 were used for RNA analysis, respectively.

The protein levels of cell-ECM complex secreted growth factors. The control group wasn’t treated with ascorbic acid and the experiment groups were treated with ascorbic acid. With collecting the supernatant of control group, the supernatants of cell-ECM complex were also collected at day 3, day 7, day 14, and day 28 after adding ascorbic acid.
Gross view and histological study of the implanted cell-ECMs
The cell-ECM complex was cut into 2.5 mL of small pieces (Figure 5(a)) and implanted subcutaneously on the back of mice. The mice were sacrificed and the cell-ECM complex were collected after being implanted for 2 and 6 months, respectively. The 2 months implants integrated with the subcutaneous tissue of mice, eventually forming a yellowish bulge (Figure 5(b)). The histological views showed masses of the implants were enclosed with dense connective tissue (Figure 5(d)–(f)). Six months later, the cell-ECM complex shrank and turned pink (Figure 5(c)), and the histological findings revealed loose connective tissue were infiltrated with blood vessels (Figure 5(g)–(i)). Compared to the implants from 2 months, the ones from 6 months were denser and the fibers appeared thicker.

Gross view and histology of cell-ECM complex implants. The cell-ECM complex prepared for implantation was cut into pieces, about 0.3 ml in a tube (Figure 5(a)). The gross views of cell-ECM complex implants for 2 months (Figure 5(b)) and 6 months (Figure 5(c)) were presented respectively. The samples were stained with HE, VG and AB stains. The cell-ECM complex implanted for 2 months were shown in (Figure 5(d)–(f) while cell-ECM complex implanted for 6 months were shown in (Figure 5(g)–(i). The cell-ECM complex was invaded by the host cells (red arrows). The blood vessels (black arrows) infiltrated in the implanted cell-ECM complex. Scale bar, 100 μm.
Discussions
MSCs are widely adopted to treat intractable chronic wounds, but locally injected MSCs suspensions rapidly degrade after transplantation. Instead of cell suspensions, MSCs are supposed to be packaged into carriers or scaffolds, which can increase the engraftment rate and cell viability, to better withstand the hostile microenvironment inundated with inflammatory molecules and enzymes.40,41 The scaffolds, synthetic materials or of natural origin, should be biocompatible, accommodative for the cells to adhere and proliferate, so the composition of ECM is preferable option. 42 Besides, scaffolds are expected to support MSCs for a long term to exert repairing or regenerative roles or even to be integrated into the host tissues. Some natural materials like collagen or hyaluronic acid, as well as human sourced materials, including plasma gel or fibrin, have been applied for carriers.38,43 However, these scaffolds might quickly disintegrate as a result of fibrolysis soon after implantation. HuMSCs implanted gelatin sponge also slowly disintegrated in 2 months in our experiments 37 and HuMSCs seeded plasma gel gradually degraded by 2 weeks. 38
Abercrombie et al. 44 revealed that fibroblasts avoid touching each other’s surfaces, which is referred as “contact-inhibition.” This “contact-inhibition” of movement can explained the tendency of cells to form a single layer at the interface, a type of behavior called “monolayering.” Ascorbic acid is added during the cell culture to encourage MSCs produce their own ECM which cells can escape from contact inhibition. 45 This technique is called self-organization or self-assembly, and is used to reconstruct vascular or dermal constructs. 46 In this study, after 4-week cultivation, a thick cell-ECM complex was formed with the MSCs embedded in collagen and hyaluronic acid. The longitudinal alignment of the collagen bundles within the cell-ECM complex gave the cell matrix a significant resistance to pull and shear force.
It is widely accepted that the therapeutic effects primarily depend on their paracrine actions, through which MSCs secrete a variety of soluble factors like growth factors, immune factors, chemokines, and exosomes, to promote the survival, recruitment, and function of wound repair cells.47,48 Along with the stimulation of ascorbic acid and subsequent deposition of ECM in which the MSCs were embedded, the mRNA and protein levels of wound healing-related growth factors and collagen continuously increased rapidly and maintained at a high level at least 1 month. Growth factors secretions in cell-ECM complex are far more than supernatants the monolayer HuMSCs released (Figures 3 and 4), which suggested cell-ECM complex has an advantage in clinical application. When treating chronic wounds, the persistent release of cytokines that promote wound healing is significantly favored over the injection of growth factors or MSC supernatants in a single dose.
Antiangiogenic circumstances compete with the angiogenic growth factors in chronic wounds (e.g. increased levels of matrix metalloproteinases). 49 HuMSCs in cell-ECM complex can assist in the development of new blood vessels by encouraging the recruitment and proliferation of host endothelial cells. The new vascular endothelial cells might invade and create a blood supply for the implanted tissue.
Without ingesting any natural or synthetic materials, the self-assembled cell-ECM complex which may match human tissue in components, proportions and structure offers the highest level of biocompatibility. In this study, the cell-ECM complex can extend HuMSCs survival period in vivo, and vice versa with the prolonged time of biomaterials when HuMSCs are embedded in them. The complex is compactly organized, and it accommodates the cells to survive in vitro or in vivo and permit host cells to migrate in to form blood vessels or reconstruct the scaffold structure after being implanted (Figure 5). Therefore, the self-assembled matrix not only played as a carrier for the cells to exert roles in promoting repair or regeneration, but it may also be adopted to fill soft tissue defects with very good biocompatibility.
The study should have been traced the fate of the cells embedded in the implanted cell-ECM complex. However, HuMSCs failed to proliferate and deposit ECMs to form a well-developed cell-matrix as we labeled the MSCs with Dil. In the continued study, more efficient cell-marking measures may be applied to elucidate how the cells evolve in the cell-ECM complex in vitro or in vivo.
Conclusions
In conclusion, the self-assembled cell-ECM complex provides a safe, producible and bioactive biomaterial with good biocompatibility in promoting wound healing. Without chemical damage some artificial materials may bring in, the cell-ECM complex can survive longer in vivo. With continuously secreting numerous growth factors, cell-ECM complex may exert an effort on wound healing through paracrine.
Footnotes
Acknowledgements
We thank Miss Bingna Zhang and Dangui Zhang (the Research Center for Translational Medicine, SUMC) for technical support. We also thank the Department of Obstetrics and Gynecology, the Second Affiliated Hospital of SUMC for their assistance in obtaining umbilical cords.
Author contributions
LY and SJ conceived of the project, designed the study and revised the manuscript. DY performed most of the research, data analysis and manuscript writing. YS participated in the vivo experiments and collected the data. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Grant for Key Disciplinary Project of Clinical Medicine under the Guangdong High-level University Development Program and Shantou Medical Science and Technology Planning Project: 2022-81-5.
Guarantor
LY