
Abstract
Objective:
To evaluate the effects of surface treatment and repair material on the repair shear bond strength (SBS) of the bioactive restorative material.
Methods:
A total of 240 Activa BioActive Restorative (Activa) discs were prepared, aged, and polished, and divided randomly into eight groups (n = 30). Groups 1–4 discs were repaired with bulk-fill flowable resin-based composite (Bulk-RBC), and Groups 5–8 discs with Activa. Surface treatment used for each repair material type were air abrasion with silica-coated 30-m Al2O3 particles (air abrasion) (Groups 2 & 6), Air abrasion with universal primer (Groups 3 & 7), and Air abrasion with universal adhesive (Groups 4 & 8). Groups 1 and 5 were controls without surface treatment. SBS test was performed, and the failure mode and surface topography were assessed.
Results:
Surface treatment with air abrasion significantly improved the SBS for repair using both Activa and Bulk-RBC. Repair SBS using Activa was significantly higher compared with Bulk-RBC. Cohesive failure in substrate and mixed failures were most common in the surface-treated groups (2–4, 6–8). Air abrasion produced prominent surface topography changes compared with polishing.
Conclusion:
Air abrasion enhances the repair SBS of aged bioactive restorative material. The use of the same material (Activa) for repair affords a higher bond strength compared with the use bulk-RBC.
Keywords
Introduction
Tooth-colored restorative materials used for direct tooth restorations include resin-based composites (RBCs), 1 conventional glass ionomer cements (GICs), resin-modified glass ionomer cements (RMGICs), enhanced RMGICs, and alkasites. Fluoride-releasing restorative materials such as GICs and RMGICs inhibit secondary caries,2 –6 which is a major cause of direct restoration failure.1,7
Glass ionomer restorations exhibit an acceptable clinical performance for primary dentitions,5,6 and permanent dentition. 8 However, because of the inferior mechanical properties of some RMGICs as compared with RBCs, degradation of the restoration surface may occur when using RMGICs. 4 In addition, RMGIC restorations loose retention and dislodge, especially in cases of shallow non-retentive cavities, 9 when compared with RBC restorations, which exhibit established and robust adhesive bonding with tooth structures. 10
Although dental restorations exhibit clinical durability, degradation with complete or partial failures occur due to the dynamic nature of oral function. Repairs of partly defective restorations are indicated with certain pre-requisites. The repair procedure involves partial removal of the defective part of the restoration, which is then replaced using new material. 11 The repair may help increase the longevity of the restoration, 12 with RBC restoration having a particularly high repair potential.
Knowledge of the composition of the resin composite is crucial for a successful RBC repair. 13 The procedure usually involves surface treatment using processes such as air abrasion, bur roughening, or the application of adhesion promoters such as silane-based primers and other contemporary repair material.11,14,15 Shear bond strength (SBS), and macro-tensile and micro-tensile bond strength (MTBS) tests can be used to evaluate the repair bond strength of RBC materials, with SBS and MTBS being the most commonly used for this purpose.11,15 GIC has a comparatively low repair potential.16 –18 There are also some controversies regarding the choice of surface treatment and repair material for GIC repair.16,18
Activa BioACTIVE Restorative (Activa), developed by Pulpdent (Watertown, MA, USA), is a new bioactive restorative material that combines the advantages of an RMGIC and RBC, representing a new category of restorative materials that are ion releasing. It contains methacrylate-based monomers, a modified polyacrylic acid, modified diurethane dimethacrylate (rubberized resin), and fillers.19,20
Partly failed or defective bioactive restorations are indicated for repair in a clinical situation. Activa can bond adhesively and is indicated for posterior stress-bearing areas because it possesses excellent mechanical and physical properties.19 –21 However, reliability of the adhesive bond between the existing and new bioactive material using different surface conditioning techniques, is unknown. This study investigated the null hypothesis that neither surface treatment nor repair material significantly affects the repair bond of Activa with ageing. The repair bond strength of Activa BioACTIVE using different materials and surface conditioning techniques was examined.
Methods
Sample preparation
The study materials and their compositions are presented in Table 1. A total of 240 Activa discs (Ø 6 mm, depth 3 mm) were prepared using a silicon mold. The Activa material was filled into the mold in a single layer, adapted, covered with a Mylar strip, and light-cured for 20 s using light emitting diode (LED) light curing unit (LCU) (EliparTM S10, 3M ESPE, St. Paul, MN, USA). Radiant existence (intensity) of the LCU was 1100 mW/cm2, as verified by Marc Resin CalipratorTM (Blue Light Analytics Inc., Halifax, Nova Scotia, Canada). Additional light-curing over 20 s was performed after removal of the discs from the mold. The prepared discs were stored in distilled water for 24 h at 37°C, then subjected to 5000 thermocycles using a thermocycling machine (THE-1100, SD Mechatronik GmbH, Feldkirchen-Westerham, Germany). In each cycle, samples were maintained in distilled water baths at 5°C and 55°C for 30 s each. The duration between the baths was 5 s, as adapted and modified from previous studies.15,22
Materials used in the study.
HEMA: 2-hydroxyethyl methacrylate; MDP: methacryloxydecyl phosphate; UA: universal adhesive; UP: universal primer.
The discs were subsequently fixed in a self-cured acrylic resin material. Silicon carbide papers with 600 grit size (CarbiMet®, Buehler, Lake Bluff, IL, USA) attached to an Automata grinding and polishing machine (Jean Wirtz, Dusseldorf, Germany) were used to polish the embedded Activa discs for 30 s, at low speed (300 rpm), under running water. After polishing, specimens were cleaned ultrasonically for 5 min with distilled water in an ultrasonic bath (Bransonic CPXH Ultrasonic Bath, Emerson Electric Co., St. Louis, MO, USA), and subsequently air-dried. According to the repair protocols applied (Table 2), the specimens were distributed randomly into eight groups (n = 30). Groups 1–4 and groups 5–8 were repaired with restorative material (Activa), and the bulk-fill flowable resin-based composite (Bulk-RBC) (Tetric N-Flow Bulk Fill, Ivoclar Vivadent), respectively.
Repair protocols applied and the mean and SD values of the repair SBS (MPa).

Superscript letters a–f indicate significant differences between groups in the same column at p<0.05; * indicated significant differences between storage time for the same group (rows) at p < 0.05.
Bulk-RBC: bulk-fill flowable resin-based composite; SBS: shear bond strength; SD: standard deviation; UA: universal adhesive; UP: universal primer.
Repair was performed without any surface treatment for groups 1 and 5. Specimens in groups 2 and 6 were subjected to air abrasion for 10 s with silica-coated 30-m Al2O3 particles (Cojet Sand, 3M ESPE) using a chair-side air abrasion device (MicroEtcher™ II, Danville, San Ramon, CA, USA), operated from 10 mm distance and with a pressure of 2 bar. Specimens in groups 3 and 7 discs were subjected to the same air abrasion treatment, followed by application and rubbing with universal adhesive (UA) (Scotchbond universal adhesive, 3M ESPE) for 20 s, air-drying until no visible motion of adhesive solution, and light curing for 10 s. For specimens in groups 4 and 8, air abrasion was followed by treatment with universal primer (UP) (Mononbond Plus, Ivoclar Vivadent, Schaan, Principality of Liechtenstein). The UP was applied to Activa surfaces and left to react for 1 min and then air-dried until no solution motion was visible. Glossy surfaces of the groups 3 and 7 and groups 4 and 8 discs were examined visually after the respective applications of the UA and UP.
A silicon mold with dimensions of 3 mm diameter and 2 mm height was secured onto the surface of each treated Activa disc to build the repair material on the disc. The repair material was applied in a single layer, light cured for 20 s using LED LCU (EliparTM S10, 3M ESPE) with radiant existence (intensity) of 1100 mW/cm2, as verified by a digital radiometer. After removal of the mold, the repair material was further light-cured for 20 s. Half of the bonded specimens in each group was evaluated for SBS after 24 h of storage in distilled water at 37°C, whereas the other half were subjected to 5000 thermocycles using the abovementioned thermocycling protocol before testing.
SBS test
A digital caliper was used to measure the cross-sectional area of each bonded Bulk-RBC or Activa material buildup at the interface. The Activa/Bulk-RBC or Activa/Activa interface was subjected to a shear force at a cross speed of 0.5 mm/min using a notched chisel mounted on a universal testing machine with a 5-kN load cell (Instron 5965, Instron Corporation, Norwood, MN, USA) until debonding or failure (Figure 1). The SBS was calculated by dividing the maximum load by the cross-sectional surface area

Schematic diagram of shear bond strength test.
The failure modes of tested specimens were evaluated (at 24 h and after thermocycling) by a scanning electron microscope (SEM) (JSM-6610LV, JEOL Ltd., Tokyo, Japan) with ×15 magnification, at a voltage of 10 kV, at 8 mm working distance. The failure modes were classified as adhesive (failure totally at the interface), mixed mainly adhesive (failure mostly at the interface), mixed mainly cohesive (failure mostly at the substrate), cohesive in the substrate (failure totally in the substrate), and cohesive in the repair material (failure totally in the repair material), as adapted and modified from a previous study. 23
Statistical analysis
Kolmogorov–Smirnov test was utilized to assess the normality of the SBS data obtained. Three-way analysis of variance (ANOVA) was utilized to analyze the data for overall significance, considering the effect of surface treatment, repair material, aging (24 h or thermocycling), and their interactions, on repair SBS. One-way ANOVA followed by Tukey’s post hoc test was used to compare the difference between specific group’s means. Independent t-test was used to detect the differences between the groups of repaired materials at 24 h and after thermocycling (p <0.05). The statistical analyses were performed using Systat Software (SigmaPlot 12.5; Systat Software Inc., San Jose, CA, USA).
Surface topography evaluation
Nine Activa discs were prepared using the abovementioned protocol, and divided randomly into three groups (n = 3). The group 1 discs were not treated, those of group 2 were polished, and those of group 3 were subjected to air abrasion using previously described protocols. The top surfaces of the discs were gold-plated and then examined by SEM with ×1500 magnification.
Results
SBS
The mean and standard deviation (SD) values of the repair SBS for all groups are illustrated in Table 2. As can be observed from the data, surface treatment using air abrasion significantly impacts the repair SBS when both Activa and Bulk-RBC are used. Regardless of the applied surface treatment, repair using Activa produced a significantly higher SBS compared with the use of Bulk-RBC. The application of the UP after air abrasion did not have any significant effect on the repair SBS for either of the repair materials, whereas the application of the UA after air abrasion (groups 4, 8) significantly improved the repair SBS compared with the other surface treatments for repair using Activa (23.71 ± 1.76 MPa) or Bulk-RBC (20.45 ± 1.97 MPa), after thermocycling. Thermocycling significantly affected the repair SBS of all groups. Only interactions between aging and surface treatment had a significant effect on repair SBS.
Failure mode assessment
The frequencies of the observed failure modes in the respective groups are illustrated in Figure 2. Adhesive failures (Figure 3A) were the most frequent in control groups 1 and 5, at 24 h and after thermocycling. At 24 h, no adhesive failures were noted in groups 2–4 and groups 7 and 8. After thermocycling, groups 1–5, and 7, presented increase in adhesive failures compared with those noted at 24 h. Mixed failures (mixed mainly adhesive and mixed mainly cohesive) (Figure 3B,C) modes were most frequent in groups 6 and 7, at 24 h and after thermocycling, and in group 8 after thermocycling. Cohesive failures in the substrate (Figure 3D) was the predominant failure mode in groups 2–4, at 24 h and after thermocycling, and in group 8 at 24 h. Cohesive in repair material was noted only in group 3 at 24 h, and was the least frequent noted failure mode.
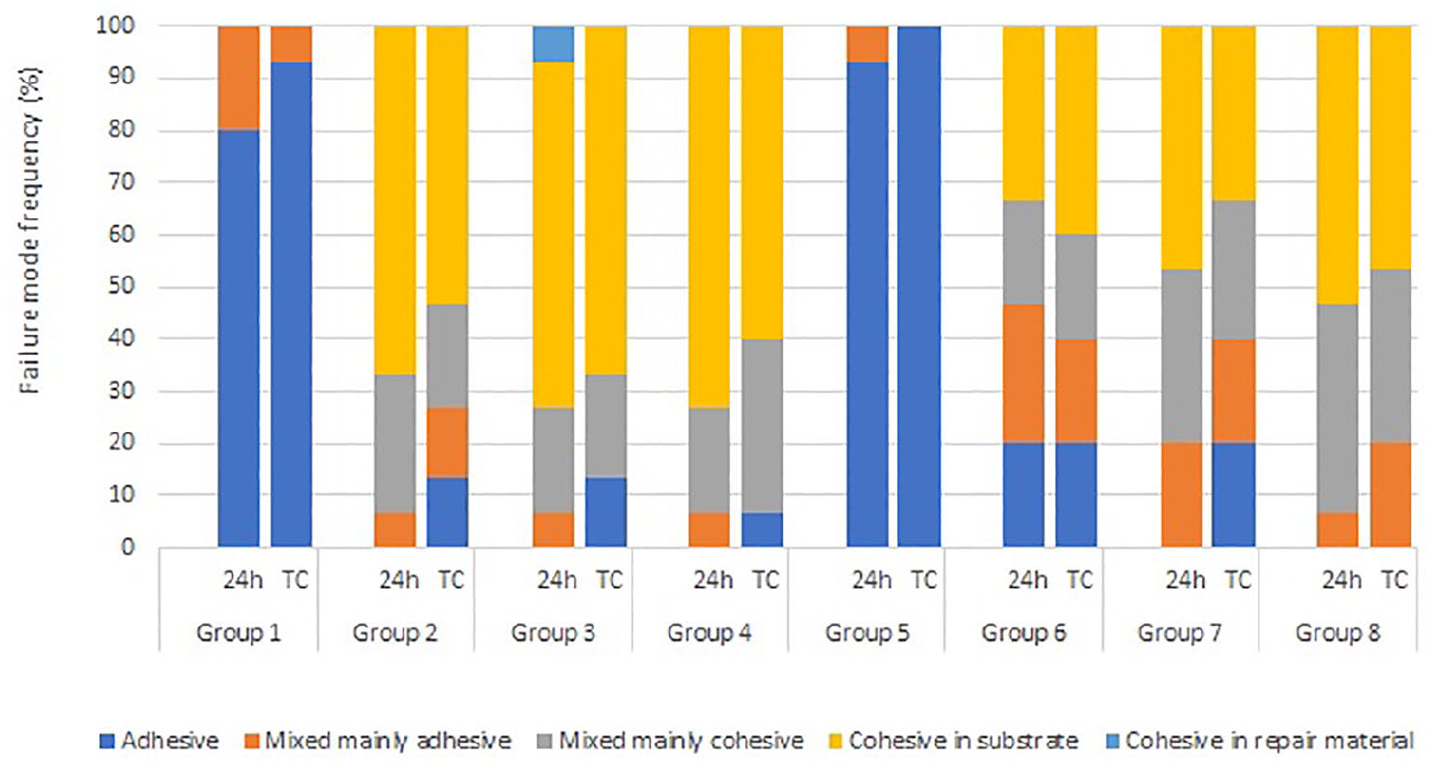
Frequencies of failure modes observed in the different repair protocol groups.

SEM micrograph (×15) showing the adhesive (A), mixed mainly adhesive (B), mixed mainly cohesive (C), and cohesive in substrate (D) failure modes.
Surface topography
The air-abraded Activa samples experienced more significant surface topographic changes (Figure 4C) compared with the polished samples (Figure 4B), whereas the samples light-cured under a plastic strip had smooth surfaces with fewer irregularities (Figure 4A).
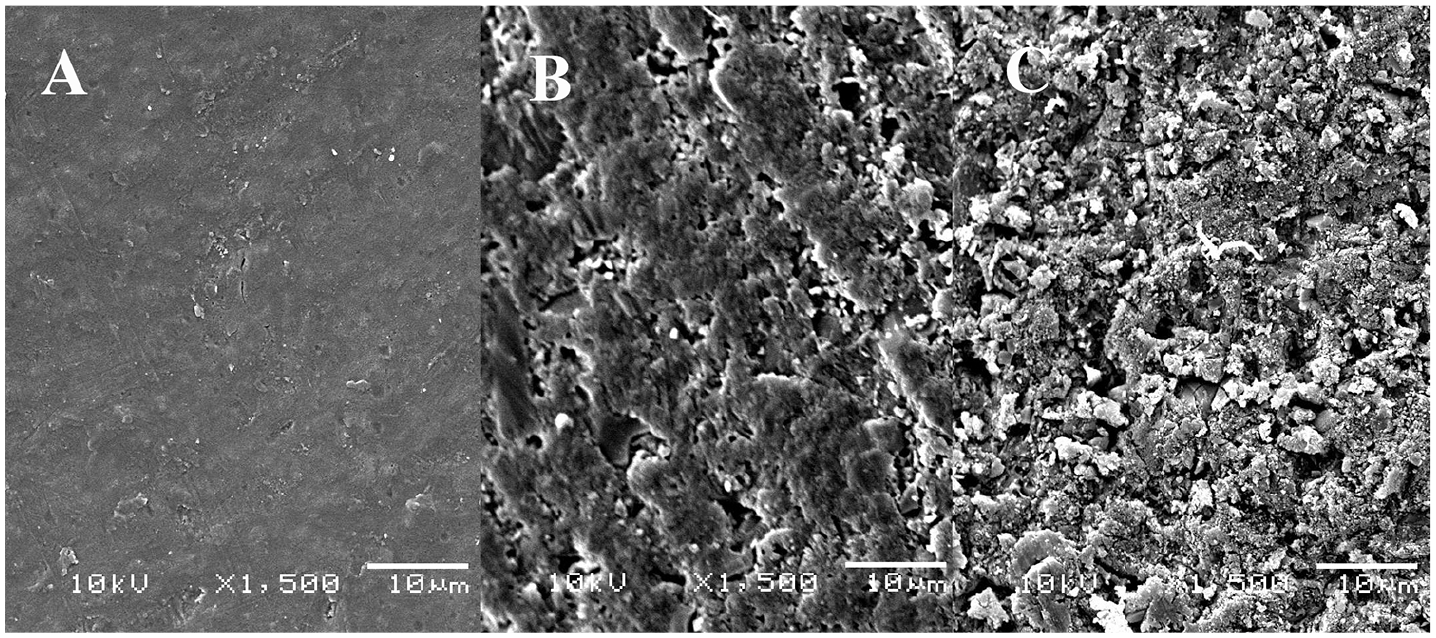
SEM micrographs (×1500) showing the surface topographies of the (A) light-cured, (B) polished, and (C) air-abraded Activa disc.
Discussion
The repair of aged resin-based materials is a challenging procedure due to decreased availability of unreacted carbon double bonds over time.24 –26 In this study, SBS test was used to investigate the effects of repair protocols (surface treatment and repair material) on the interfacial repair SBS of an aged bioactive resin-based restorative material (Activa). Despite the reported limitations of the SBS test, 27 it is commonly used to evaluate resin to resin repair bond strength. 15 Sau et al., reported that the shear loading of a specimen was clinically relevant because it induces different stresses (shear, tensile, and compressive), which usually occur during mastication. 28 The outcomes of the study indicated that both the surface treatment method and the type of repair material affect the bond strength with aged Activa at 24 h and after artificial aging by thermocycling. Thus, the null hypothesis was rejected.
Air abrasion has been recommended as an efficient surface treatment method for enhancing the repair of resin-based restorative materials.11,14,18,29 The air abrasion process in this study utilized silica-coated 30-m Al2O3 particles, which increased the surface area through deposition of the silica particles on the material surface, thereby the chemical adhesion of the repair material may be promoted after the application of silane. 30 Surface treatment with air abrasion resulted in significant improvement of the repair SBS, irrespective of the repair material or the employed primer. It was observed that the surface topography changes and irregularities produced by air abrasion to facilitate the foregoing are greater than those produced by polishing using #600 silicon carbide paper discs (Figure 4).
Silane and phosphate monomers were the active ingredients of the UP applied to group 3 and 7 samples. The molecules of the silane contained two functional groups, namely, a silanol group that reacts with the inorganic components such as filler particles of RBC and an organo-functional group that reacts with the methacrylate groups. 30 Silanes are known to chemically promote bonding with a composite air-abraded using CoJet Sand. 30 However, contrary to the observations of previous in-vitro studies,30,31 air-abrasion using silica coated Al2O3 particles and application of the UP did not produce any significant effect in the present study.
In this study, the UP did not improve the bond strength irrespective of the repair material. Considering that the chemical coupling of the silane with the composite depends on the surface availability of silica, 11 and, given the small amount (7%) of silica in the entire filler of the Activa, the silane did not significantly enhance the bonding with Activa. Silane coupling agent contributes minimally to improvement of the repair after roughening of the composite. 11 The present results agree with the findings of a previous study, which indicated positive effects of surface treatment by air abrasion and silica coating irrespective of the silane or adhesives used. 32
In addition to the micromechanical aspect of the repair, there is a chemical aspect that is a function of the reaction between the substrate and the adhesion promoter (primer) and repair material. It is recommended to repair RBC using the same material.24,31,33 Bulk-RBC was one of the two repair materials considered in this study as chemical bonding between RBC and hybrid materials such as RMGIC has been reported. 34 The repair of Activa using the same material was observed to produce a higher bond strength compared with the use of bulk-RBC, attributed to the greater compatibility between the resin contents of the substrate and repair materials in groups that Activa was applied to substrate with no UP or UA. However, when UP or UA was applied, the mechanical and physical properties of the two repair materials might explain the difference in the SBS obtained. When Activa was used as the repair material, there was less sensitivity to UP or UA. This is similar to the observation of Bacchi et al., 24 who found that the repair bond strength of RBC was less affected by surface treatment when the repair was done using the same material as the substrate. The application of a UA efficiently enhances the adhesion and improves RBC repair, 29 and this may explain the positive effect on the repair SBS when Bulk-RBC was used as the repair material in the present study.
Thermocycling protocols are not standardized in laboratory dental studies conducted to evaluate bond strength. 35 Thermocycling significantly decreased the repair SBS of all groups. Negative effect of thermocycling on bond strength of adhesively bonded materials is well-known. 36 The failure modes noticed in this study may reflect the repair bond strength. The adhesive failure observed in the two control groups may be attributed to a weaker repair SBS. SBS testing is characterized by uneven stress distribution and the inducement of cohesive failure. However, this may not entirely explain the high incidence of cohesive and mixed failures in the groups containing samples subjected to air abrasion. This may be explained due to observed high repair bond strength, the reduced strength of the aged Activa substrate and unhomogeneous stress distribution. Different frequencies of mixed and cohesive failures in groups repaired by active or Bulk-RBC might be attributed to repair bond strength obtained and the physical and mechanical properties of the two repair materials.
Conclusion
Surface treatment by air abrasion significantly enhances the repair bond strength of aged bioactive restorative material.
Footnotes
Contributorship
MM.A. and N.A. researched literature and conceived the study. MM.A., N.A. and F.A. prepared samples and performed the investigation. MM A., M.O., and A.A. were involved in protocol development. A.A. and A.M. did the statistical analysis. MM.A., A.A., and A.R., interpreted data. MM.A. wrote the first draft of the manuscript. A.R., A.A, and F.V. reviewed and edited the manuscript. F.V., M.O., A.M.M., and A.A. supervised the project. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Guarantor
Ali Alrahlah.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to the Deanship of Scientific Research, King Saud University for funding this study through the Vice Deanship of Scientific Research Chairs and Research Chair for Dental and Oral Rehabilitation, Engineer Abdullah Bugshan Research Chair for Dental and Oral Rehabilitation.