
Abstract
Background
Air pollution is a leading global public health challenge, with PM2.5 exposure strongly associated with respiratory and cardiovascular morbidity. In developing countries like Pakistan, urban air pollution levels are particularly severe. In 2021, Peshawar was ranked 9th globally for pollution, with PM2.5 levels 12 to 16 times higher than WHO limits. This study investigates chronic exposure to heavy traffic emissions and its long-term effects on lung function in Peshawar’s roadside vendors, a highly exposed occupational group from an under-reported location.
Design and Methods
A cross-sectional study was conducted on 218 non-smoker male roadside vendors in Peshawar. Spirometry assessed FEV1, FVC, PEF, and FEV1/FVC ratio against GLI-predicted values adjusted for age and BMI. Duration of work and daily exposure hours were documented. Ground-based PM2.5 data (2019–March 2025) were recorded separately. Analysis was performed in SPSS using multivariate linear regression models.
Results
PM2.5 remained consistently high (mean range: 139–166 μg/m3) from 2019–2025, with notable occasional spikes observed. All spirometric indices declined with increasing exposure duration. Regression showed each additional year reduced GLI-predicted %FEV1 by 0.3 % (p=0.042) and %PEF by % 0.47 (p=0.018). Descriptive statistics showed the >20-year exposure group had the lowest GLI-predicted % means for FEV1, FVC, FEV1/FVC and PEF values. Normal spirometry predominated, but restrictive and obstructive patterns were also observed in earlier exposure groups.
Conclusion
Prolonged roadside air pollution exposure progressively impairs lung function, underscoring the urgent need for occupational and environmental public health interventions to safeguard high-risk informal workers.
Introduction
Clean air, essential for human well-being, is increasingly at risk due to widespread air pollution, leading to health hazards ranging from minor eye irritation and upper respiratory infections to chronic lung and heart diseases, increasing mortality rates. 1 According to WHO in 2019, ambient air pollution in urban and rural areas was responsible for approximately 4.2 million premature deaths annually, primarily due to exposure to fine particulate matter (PM2.5). 2 While air pollution is a global concern, its severity is notably worse in developing and lower-middle-income countries, where rapid urbanization has led to pollutant levels far exceeding WHO standards, with 98% of cities with populations exceeding 100,000 failing to meet air quality guidelines. 3
Pakistan is facing a similar fate. The 2019 State of Global Air report identified South Asia as having the highest annual PM2.5 exposure globally, with Nepal, India, Bangladesh, and Pakistan ranking among the worst-affected countries. 4 Pakistan ranks third globally in terms of air pollution-related mortality, with an estimated 128,000 deaths annually. 5 Within Pakistan, Peshawar which is a major city in the northwest, reflects the severity of air pollution in the region. According to the 2017 census, with over 4 million residents and one registered vehicle for every six people, 6 the city faces significant anthropogenic pollution from industries and vehicles. The 2021 World Air Quality Report ranked Peshawar as the ninth most polluted city globally and the third most polluted in Pakistan. The city’s PM2.5 levels have ranged from 61.40 µg/m3 to 80.09 µg/m3 annually, exceeding national standards by 4–5 times and WHO guidelines of <5 µg/m3 by 12–16 times. 7 IQAir data frequently categorizes Peshawar’s air quality as “Unhealthy” under the U.S. AQI scale. 8
While immediate health effects might not always be apparent, prolonged exposure to such pollution levels poses significant long-term health risks, raising serious public health concerns. Extensive research shows that prolonged exposure to PM2.5 correlates with decline in lung function parameters, such as Forced Expiratory Volume in one second (FEV1) and Forced Vital Capacity (FVC). For instance, the Framingham Heart Study linked long-term traffic-related air pollution and PM2.5 exposure to reductions in FEV1 and FVC, even at low levels. 9 Similarly, studies on workers exposed to high dust levels revealed accelerated declines in FEV1. 10 Research at UCLA and findings by Sekine et al. report similar trends.11,12 Limited regional studies like A. Raza et al. also found that brick kiln pollution in Pakistan significantly reduced FEV1 and FVC values among workers, emphasizing the impact of PM2.5 on respiratory health. 13 The mechanisms by which PM2.5 affects health are not fully understood. While larger particles (PM10) are typically trapped in the upper respiratory tract, smaller particles (PM2.5) penetrate deeper into the bronchi and alveoli. PM2.5’s complex composition—including organic, inorganic, and biological compounds—can disrupt physiological processes, triggering immune responses such as inflammation, oxidative stress, and altered cytokine production. 14 Additionally, PM2.5 may act similarly to cigarette smoke by constricting small airways through endothelin release and oxidative effects. These changes contribute to respiratory conditions such as asthma, chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, and cancer. 15
Lung function is typically assessed using parameters such as Forced Vital Capacity (FVC), the total air exhaled after a deep breath; Forced Expiratory Volume in 1 second (FEV1) and Peak Expiratory Flow (PEF), reflecting maximum exhalation speed. The FEV1/FVC ratio indicates the proportion of lung capacity exhaled in one second. Changes in these parameters signal lung damage and reduced respiratory function. Despite extensive research linking PM2.5 exposure to declining lung function, notable gaps remain. Many epidemiological studies focus on short-term pollution spikes, overlooking the effects of sustained exposure. Moreover, research in developing countries like Pakistan is very limited, despite these regions facing higher pollution levels and weaker regulations. This study provides data on at-risk worker populations from an under-reported region, addressing a gap in knowledge by assessing respiratory health in individuals regularly exposed to elevated PM2.5 levels. We examined asymptomatic and previously unrecognized declines in lung function and correlated these findings with years of occupational exposure to better understand the long-term health impacts on this group.
Design and methods
Study area and population
This cross-sectional study took place in Peshawar district, northwest of Khyber Pakhtunkhwa province, at six heavily polluted roadside locations: Hayatabad, Board Bazaar, Karkhano Market, University Town, Khyber Bazaar, and Saddar Bazaar as shown in Figure 1. The sample size was calculated to be 218 using the Cochrane formula. Only male roadside vendors and open-air shopkeepers aged ≥18 were recruited. The sampling technique used was convenient non-probability sampling due to the dynamic and mobile nature of study subjects. Inclusion criteria required participants to be permanently employed at the same location for at least two years, working six to seven days a week with a minimum of eight hours of daily occupational exposure to ambient air. Exclusion criteria included individuals with any pre-existing respiratory or any smoking status. Screening for pre-existing conditions or opportunistic/seasonal diseases (e.g., asthma, TB, ILD, influenza, pneumonia etc) were performed by medical doctors through taking an oral medical history, blood pressure measurement, and chest auscultation using a stethoscope. Written informed consent was obtained from all participants prior to enrollment. Participant anonymity and confidentiality were maintained, and ethical approval was granted by the Institutional Review Ethical Board (IREB) of Khyber Medical College, Peshawar (Approval No. 77/DME/KMC). Map of Peshawar with pins indicating the six heavily polluted roadside sites where spirometry was conducted.
Air quality measurement
The air quality data for this study were derived from a secondary source. The dataset, spanning from May 2019 to March 2025, was obtained from the BAM-1020 air quality monitoring station located at the US Consulate in Peshawar, 16 which provides real-time AQI and PM2.5 measurements. PM2.5 concentrations were summarized using descriptive statistics including mean, standard deviation, and range. In addition, median and interquartile range (IQR) values were reported to describe the distribution of the data, with the IQR representing the middle 50% of values. Use of the IQR in air pollution epidemiology accounts for skewed pollutant distributions and allows better comparison across pollutants measured in different units. 17 Data consistency throughout the years was confirmed through cross-referencing with historical records. 7
Lung function testing
Lung function was measured using the SpiroLab 4.0, a portable spirometer with rechargeable battery and built-in printer. Predicted spirometry values (FEV1, FVC, PEF and FEV1/FVC) and Z-scores were calculated using the Global Lung Function Initiative 2012 (GLI-2012) reference equations. These equations provide standardized predicted values based on age, sex, height, and ethnicity, allowing comparison of an individual’s measured lung function against a healthy reference population. The South East Asian GLI-2012 ethnicity module was applied for all participants to derive predicted values and Z-scores. 18 Measured values were interpreted against these standardized reference values. Participants’ age, height, weight, daily air exposure, and work duration were also documented separately. Testing followed American Thoracic Society guidelines, 19 supervised by a trained technician. Each subject performed three tests, with the best result used for analysis. Conducted between March 13 and 29, 2025, testing also involved daily calibration of the spirometer.
Statistical analysis
Statistical analysis was conducted using SPSS version 27.0. Descriptive statistics (mean, standard deviation) were calculated for age, height, weight, BMI, daily working hours, and years of work. Age was grouped into young adults (18–35), middle-aged (36–45), and older adults (46–60). BMI categories included underweight, normal, overweight, and obese, while work exposure was classified into 2–5, 5–10, 10–15, 15–20, and over 20 years. Cross-tabulations compared these categories with lung function parameters (FEV1, FVC, PEF, FEV1/FVC). Multivariate linear regression models for GLI-predicted percentage pulmonary functions adjusted for BMI and working hours per day were employed to access the association of spirometric indices with exposure duration.
Results
Demographic statistics of study population.

Descriptive statistics of study population.

Values are presented as mean ± standard deviation (SD). The values represent unadjusted spirometric measurements.
PM2.5 concentration
PM2.5 concentrations (in µg/m3) for years 2019-2025.

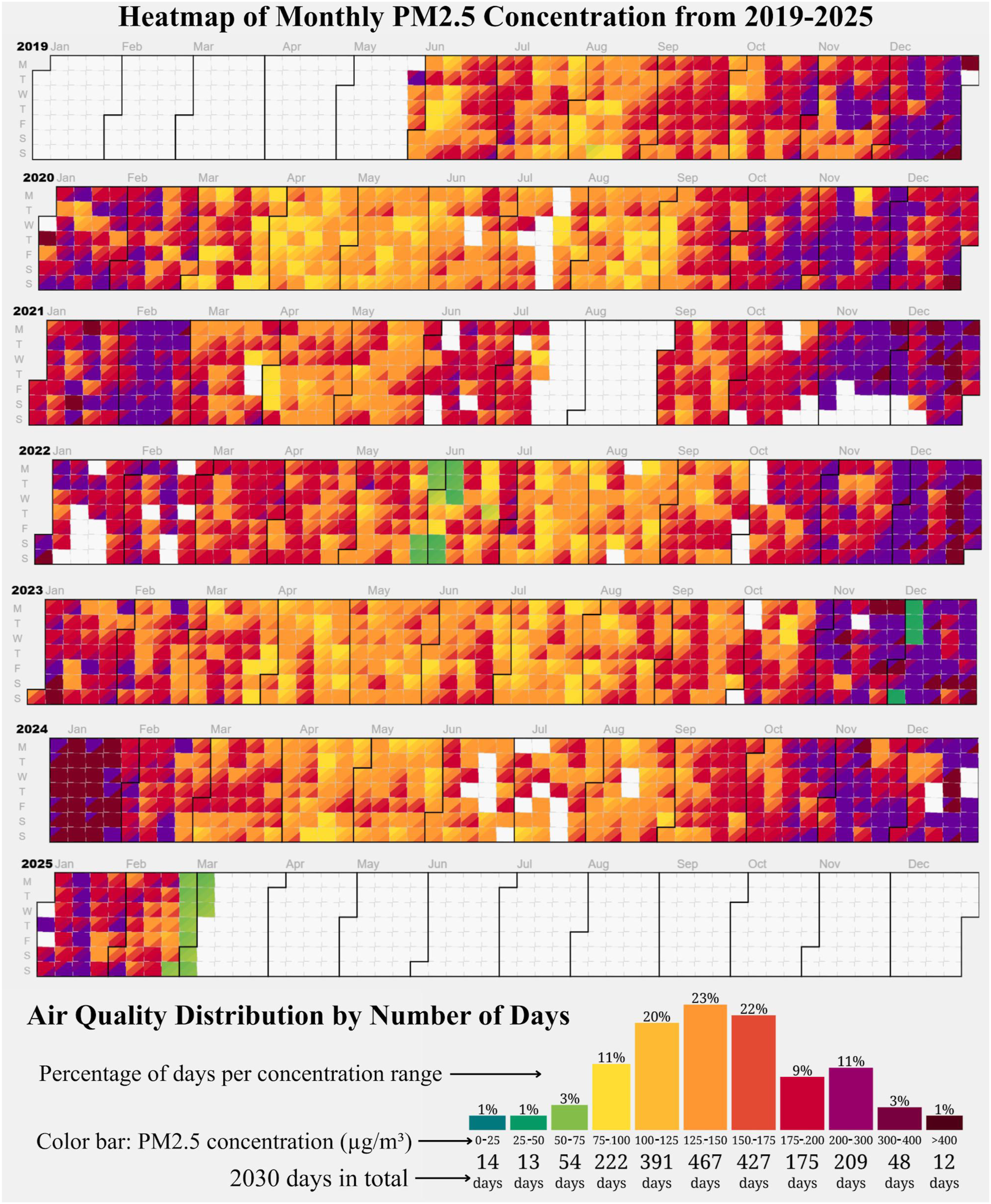
Heatmap showing average daily PM2.5 concentrations recorded by BAM-1020 air quality monitoring station from June 2019 to March 2025, with color intensity indicating pollution levels.
Association of predicted % pulmonary functions with years of work exposure
Multivariate linear regression model summary of years of workplace exposure on GLI-predicted pulmonary function indices (%), adjusted for BMI and working hours/day.

Note. β = unstandardized regression coefficient (change in predicted % per year of workplace exposure).
Discussion
Pakistan is a country suffering from severely worsening air quality. The present study demonstrates that vendors with prolonged exposure to elevated levels of roadside air pollution were associated with a statistically significant decline in lung function compared to those with shorter exposure durations. Unlike most previous investigations, this research focuses on the duration of work exposure rather than static area sampling of air pollutants. This approach is justified because personal exposure measurements differ from static area measurements, which may obscure true thresholds and disease patterns in epidemiological studies, 20 especially in low-resource settings such as Pakistan. Therefore, this analysis emphasizes long work durations in individuals whose livelihoods depend on daily roadside exposure, rather than relying on modeled air sampling to assess its causal relationship with lung function given that mean PM2.5 concentrations in this region have remained consistently 12 to 16 times higher than the WHO annual guideline of 5 µg/m3 for over two decades. 7
The regression analysis in Table 4 shows that years of work exposure was a significant predictor of Pred % FEV1 (accounting for hours/day and BMI), showing that each additional year of work exposure was associated with 0.3% decline in FEV1 per year. These findings align with several previous studies; For instance, a meta-analysis on occupational exposure to respirable quartz dust found a significant negative association of FEV1 and FEV1/FVC with increasing exposure, with a 4.6% reduction in predicted FEV1 compared to workers with low exposure. 21 Similarly, a study in Tokyo reported a -0.020 L/year decline in FEV1 in highly polluted areas compared to -0.009 L/year in least polluted areas. 12 The UCLA Population Studies of Chronic Obstructive Respiratory Disease found a decline of 23.6 ml/year (-0.0236 L/year) in FEV1 for individuals living in the highly polluted areas of Southern California, accounting for 71% of the decline attributed to smoking over one pack per day. 11 The Framingham Heart Study also linked higher PM2.5 levels to faster FEV1 decline (2.1 ml/year faster decline per 2 μg/m3 PM2.5 increase). 9 A similar study on workers with high dust exposure reported an accelerated FEV1 decline of 4.5 mL/year (0.004 L/year). 10 Conversely, The ESCAPE meta-analysis 22 and a multi-center study by Götschi et al. 23 in Europe found no significant association with lung function decline, likely due to biases in Götschi’s study 23 and inconsistencies across the ESCAPE meta-analysis. 22
While the changes in lung function observed in this research may seem small like most previous studies, evidence indicates that even small decrements in FEV1 are clinically relevant. Epidemiological studies consistently demonstrate that lower FEV1 is associated with an increased risk of cardiovascular disease 24 and overall mortality. Prior guideline-based literature suggests that a change of ≥100–200 mL in FEV1 or a decline of 5–10% in percent predicted values is often considered a clinically meaningful change beyond expected biological variability. 25 Such declines have been linked with worsening health-related quality of life, poorer functional status, and increased respiratory symptom. 26 Importantly, large population-based analyses demonstrate that decreasing FEV1 % predicted strongly stratifies survival probability in chronic respiratory disease, with markedly lower survival observed among individuals with severe impairment compared with those with preserved lung function. 27
Our findings were consistent with the gradual decline in the mean values of FEV1, FVC, PEF, and the FEV1/FVC ratio across the five exposure cohorts (Table 2). Zhou et al. 28 reported a 3.63% decline in FEV1/FVC after three years and a 7.15% decline after six years of high PM2.5 exposure. Similarly, Gupta et al. 29 found significant reductions in FVC, FEV1, and PEF among traffic police with over eight years of service compared to shorter tenures. Another study found that roadside vendors with over ten years of exposure had greater respiratory impairment than those with less than ten years, consistent with this research. 30 Similarly, in heavily polluted areas of Delhi, India, roadside hawkers had both FVC and FEV1 below 70% of predicted values, with an FEV1/FVC ratio of 78.28%, indicating reduced lung function. 31 In Chennai region, among street vendors, the exposed group showed lower lung function, with a mean FVC of 1.88 compared to 2.38 in the control group, a mean FEV1 of 1.71 versus 2.01, and an FEV1/FVC ratio of 86.97 compared to 87.23. 32 A slight upward trend in Pred % FEV1 and Pred % FVC was observed in our study going from 15–20 years to 20+ years exposure groups (Table 2). The observed upward trend in %FEV1 and %FVC may be attributed to younger individuals or those with better BMI, who typically have stronger baseline lung function. Additionally, smaller sample sizes in the longer exposure groups could introduce variability, as individuals with better initial lung function may maintain stable % predicted values rather than showing the expected decline.
Research indicates that long-term exposure to ambient air pollution is associated with restrictive rather than obstructive ventilatory patterns. 33 However, effects can vary depending on the type and duration of exposure. Pollutants such as PM2.5 exacerbate respiratory diseases like asthma and COPD in the short term while hindering lung function development in children over the long term. 34 Prolonged exposure to air pollution from brick kilns causes obstructive and restrictive impairments 13 while coal mine or silica dust exposure leads to restrictive, obstructive, or mixed pulmonary patterns. 35 In this study, spirometric impairments were few and mostly observed in early 2-15 years groups instead of the later ones. As explained earlier, this may be due to the small sample in later groups (>15-years categories) where small random variation like higher lung sensitivity or genetic predisposition can lead to misleading patterns. While this study only reports the concentrations of PM2.5, the observed impacts were likely due to PM2.5 in combination with other pollutants from vehicles and fuel exhausts. Evidence shows that exposure to both particulate matter and irritant gases like nitrogen dioxide (NO2) causes more severe lung damage than either alone. 36
To minimize the healthy worker effect, we ensured inclusion criteria that allowed for a diverse range of participants within the healthy population, including variations in age, BMI, and occupational exposure history where applicable. While participants were generally healthy, stratification was applied during data analysis to account for subgroups with differing baseline characteristics. Lung function showed a decline with age as expected. BMI generally decreases lung function, but interestingly, a higher BMI has been linked to a slower FEV1 decline in COPD patients, supporting the “obesity paradox” and suggesting a protective effect on lung function. 37 In this study (Table 2), the Pred % FEV1 increased similarly from 89% L (overweight) to 94% L (obese), potentially reflecting this effect.
Few studies in Pakistan have examined the effects of occupational exposure on lung function. Ali et al. 38 found that roadside workers exposed to traffic pollution had higher risks of asthma, cardiovascular symptoms, and increased hospitalization. In Karachi, Mubashir Zafar et al. 39 observed reduced FEV1, FVC, and FEV1/FVC values in petrol station workers. A comparative study in Peshawar also reported lower PEF measurements in men working in urban open shops compared to rural areas. 40
This research has several limitations. The small sample size and cross-sectional limits the generalizability and causal relationships of the findings. While longitudinal follow-up would be ideal for such study design, the temporary nature of participants’ jobs complicates this process, with many being lost to follow-up. Cumulative PM2.5 exposure was estimated using years of work as a proxy; however, this approach is prone to exposure misclassification because exposure among individuals may vary widely depending on job tasks, work location, use of protective measures, and residential or indoor environmental exposures. Additionally other factors like socioeconomic status, indoor use of biomass and ventilation, physical activity, and genetic predispositions could also introduce bias. The sample size was constrained by difficulty finding subjects who met the inclusion criteria of minimum 8 hours of daily work, 2 years of regional employment, and non-smoking status. This likely reduced statistical power and may have increased the risk of type II error as some subgroups, particularly those with longer exposure durations, included relatively few participants. It is also speculated that some participants may have been ex-smokers. In Table 3, PM2.5 data from 2019–2025 does not fully reflect historical exposures for participants who began working years or decades earlier. Moreover, the healthy worker effect may also have influenced our findings as workers who develop significant respiratory symptoms may quit their high-exposure jobs, leaving a relatively healthier population and underestimating long-term impacts in our sample.
Despite these limitations, the study possesses some important strengths. By deliberately selecting the most heavily polluted areas of Peshawar, the analysis targeted a vulnerable underrepresented group of individuals from a low socioeconomic background. This focus differs from most previous research, which has assessed lung parameters within the general population. During analysis, important confounding factors (age, sex, height, weight, ethnicity, work hours/day) were adjusted and systematically accounted for. Additionally, while we acknowledge that cumulative exposure metrics based on annual mean PM2.5 concentrations could be regressed against outcomes, such data is not available for the different years worked by participants, many of whom were exposed decades ago. Moreover, in low-resource settings such as Pakistan, historical air monitoring is sparse, and assumptions about past concentrations may not be reliable. Instead, work duration was used as a proxy for cumulative exposure, since personal exposure is known to differ significantly from static monitoring that has some inherent limitations as previously discussed. 20
The findings have crucial implications for public health and policy in Peshawar, calling for comprehensive and targeted health interventions. The underprivileged communities, often devoid of basic healthcare facilities, are the ones most affected by environmental pollution. Given that many individuals remain asymptomatic until significant pulmonary damage occurs, as observed in this research, regular occupational health surveillance and respiratory disease screening for informal workers are recommended, alongside the proper use of protective masks during traffic hours. These results also support the development of air quality regulations and pollution control measures to reduce exposure in high-risk populations. Future investigations could address the gaps identified in this study by exploring the effects of specific pollutants, indoor pollution, lifestyle variations over shorter time intervals, while including women to explore social and gender-related factors and improve generalizability (as they were excluded in this study). Prospective or longitudinal study designs would better evaluate the temporal changes in lung function and more precise exposure assessment, such as personal or location-specific monitoring, may provide more accurate estimates of individual exposure.
Conclusion
This study highlights the public health burden of chronic ambient PM2.5 exposure among roadside vendors in Peshawar. The progressive decline in lung function parameters, including FEV1, FVC, PEF, and the FEV1/FVC ratio, with increasing exposure underscores the considerable susceptibility of this underreported demographic to chronic respiratory impairment. Although the observed reductions may appear modest at the individual level, their cumulative impact has important implications regarding population health posing challenges for uplifting public health. These findings highlight the urgent need for health intervention, improved air quality regulation, and protective strategies for high-exposure, low-income communities in developing countries.
Supplemental material
Supplemental material - Long-term lung function decline from chronic workplace exposure in roadside vendors of Peshawar, Pakistan
Supplemental material for Long-term lung function decline from chronic workplace exposure in roadside vendors of Peshawar, Pakistan by Hamza Khan Khattak, Zmarak Ahmed Khan, Saadia Ashraf, Mahliqa Kirmani, Laiba Malik, Kainat Usman, Syed Abdullah, Kamil Ahmad Kamil, and Bushra Iftikhar in Journal of Public Health Research.
Footnotes
Acknowledgements
The authors have no acknowledgements to make.
Ethical considerations
The Institutional Review Ethics Board (IREB) of Khyber Medical College chaired by Dr Farooq Ahmed reviewed and approved the proposal for the study. The approval number as granted by the IREB is 77/DME/KMC.
Consent to participate
Informed consent from participate was obtained from all prior to enrollment in the study under the supervision of Ethical Committee. Written informed consent was obtained from all participants prior to their inclusion in the study. Participants were informed about the study objectives, procedures, potential risks, and benefits, and were assured of the confidentiality and anonymity of their data. Participation was entirely voluntary, and participants were free to withdraw from the study at any time without any consequences.
Consent for publication
This study does not include any individual details, images, or videos that would require consent for publication. Therefore, this section is not applicable. As this study does not include any identifiable individual participant data, images, or personal information that has been included in the manuscript.
Author contributions
The conceptualization of the study was carried out by Hamza Khan Khattak and Bushra Iftikhar. Data collection was conducted by Hamza Khan Khattak, Zmarak Ahmed Khan, Mahliqa Kirmani, Laiba, Kainat Usman, Abdullah Shah, and Saadia Ashraf. Data cleaning was performed by Hamza Khan Khattak, Zmarak Ahmed Khan, Kainat Usman, and Laiba. Data analysis was undertaken by Hamza Khan Khattak and Zmarak Ahmed Khan. The manuscript was written by Hamza Khan Khattak, Zmarak Ahmed Khan, Laiba, Mahliqa Kirmani and Abdullah Shah. Supervision was provided by Bushra Iftikhar. The manuscript was critically reviewed by Saadia Ashra, and Kamil Ahmed Kamil. All authors read and approved the final version of the manuscript. The submission of the manuscript and overall coordination were handled by Kamil Ahmed Kamil.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The sample data that support the findings of this study are available on request from the corresponding author, due to privacy concerns.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.