
Abstract
Background
The prevalence of falls in older adults has increased in Thailand and worldwide. Falls can cause injuries, disability, and death in older population.
Aims
The purpose of this study was to assess the effects of a home environmental modification program for fall prevention among the older adults in northern Thailand.
Design and methods
A quasi-experimental study was conducted. The study subjects were 80 older adults aged ≥60 years. They were categorized into 2 groups, 40 participants per arm. A questionnaire was employed for data collection. Frequency, percentage, mean, standard deviation, independent sample t-test, paired t-test, Chi-square test, McNemar’s test, and relative risk (RR) were utilized for data analysis.
Results
After the intervention, the experimental group had significantly higher mean scores of knowledge, social support, and home environmental modification compared to before the intervention and compared to the control group (p<0.05). Further, the proportion of falls in the experimental group was significantly lower than before the intervention, and in the control group (p<0.05). The program can reduce falls by 27.5% and the control group was more likely to have falls 6.0 times than the experimental group after the intervention.
Conclusions
The program on home environmental modification was effective in preventing falls for older adults. Therefore, healthcare providers, caregivers, health volunteers, and relatives of the older adults should apply this program as a guideline to prevent falls and their consequences in the target group.
Introduction
Falls is the second leading cause of unintentional injury deaths worldwide. Falls in older adults are the leading cause of severe injuries such as hip fractures, lacerated wounds, sprains, and subarachnoid hemorrhage. All of these illnesses can cause long-term care, and some of them might become disabled or die as a consequence. 1 Globally, it is estimated that 684,000 individuals die each year from falls, of which over 80% are in low - and middle-income countries. Further, older adults aged ≥60 years suffer the greatest number of fatal falls. 2 In Thailand, the death rate of falls in older people aged ≥60 years was higher than in other age groups. 3 There were approximately 3 million cases of falls per year that occurred in older adults, and 4 deaths every day, or around 1,500 cases per year. 4 Falls among older adults in northern Thailand are a significant public health concern, with prevalence rates varying based on location and population groups. In Phitsanulok Province, older adults who had a history of a fall was 17.7%. 5
It is estimated that older adults aged≥60 years worldwide increased from 15% in 2015 to 22% in 2050. 6 The population of older adults aged ≥60 years is increasing significantly, primarily driven by rising life expectancy. 7 In addition, high technology and advancements in medical science help to prolong life and increase the number of older adults. 8 In 2023, Thailand had 12, 116, 199 older adults aged≥60 years or 18.3 % of the 66, 208, 737 population, and it is expected that Thailand will become an aged society in 2073.9,10
As one gets older, health problems can arise, particularly since the rate of chronic diseases tends to increase significantly with age. Approximately 75% of Thai older adults had metabolic syndromes such as hypertension, diabetes mellitus, or dyslipidemia. 11 Some chronic diseases contribute to fall risk, such as stroke, osteoporosis, diabetes, hypertension, and obesity.12,13 Moreover, older adults have changes in physical deterioration, such as hearing loss and long-sightedness, a decrease in the amount and size of the musculoskeletal system, which affects the balance of the body, and muscle weakness. These conditions can also cause falls in older adults.14,15
The Bureau of Environmental Health, Ministry of Public Health, Thailand, developed a handbook of home environmental management for healthcare providers and caregivers to use as a guideline to prevent falls in older people. 16 However, the incidence of falls did not decrease and tended to increase every year. These resulted from village health volunteers, caregivers, and the relatives of older people still lacked knowledge and skills to support older adults for environmental modification in their houses. 17
The previous studies found that programs on home environmental modification helped to reduce incidence, injuries, and falls in older people. In addition, the samples in these studies gained more knowledge and skills to modify their home environment since the programs provided social support from village health volunteers and healthcare providers.18–21 Additionally, a systematic review of interventions reported that falls were reduced by 11%-26% after the interventions. 22 However, no study in northern Thailand confirms that social support can reduce falls in older adults. Therefore, our study proposed including not only village health volunteers and healthcare providers, but also caregivers and relatives of older adults involved in supporting the intervention program.
Prevention strategies to reduce falls and risk for older adults in the community should emphasize education, training, and creating safer environments. Our study aimed to assess the effects of a home environmental modification program for fall prevention in older adults aged ≥60 years, in northern Thailand. We employed the social support theory 23 together with the guidelines of the Ministry of Public Health 16 to develop the intervention program. The social support was expected to motivate older adults to make home environmental modifications for fall prevention via home visits. The program focused on giving knowledge, practicing, advising, and visiting the homes of older adults. The results from this study can be utilized as a guideline for fall prevention to reduce injuries, disability, and death, and improve the quality of life among older people in the future.
Specific objectives. 1. To compare mean scores of knowledge about home environmental modification, social support on home environmental modification, and home environmental modification between and within the experimental group and the control group before after the intervention. 2. To compare the risk difference between the experimental group and the control group after the intervention. 3. To compare the proportions of falls between and within the experimental group and the control group before and after the intervention.
Materials and methods
Study design
This quasi-experimental study was conducted between February and June 2023 to assess the effects of a home environmental modification program for fall prevention among older adults in northern Thailand. The reporting of this study conforms to the CONSORT statement.
Settings and participants
We randomly selected one province (Phitsanulok Province) out of eight representing the highest proportion of older adults in northern Thailand, via a simple random sampling. Then, one district, followed by one subdistrict, and 4 villages under the selected subdistrict were drawn by a simple random sampling, respectively.
The study subjects were 80 older adults aged ≥60 years. The sample size was calculated using the formula for testing two independent proportions. 24 The power was set at 80%, alpha (α) was 0.05, and the effect size was 40%. 25 The ratio of the experimental group to the control group was 1 to 1. We selected 80 participants who met the inclusion criteria from the selected villages via a systematic random sampling, and they were classified into two groups, the experimental group, and the control group. Each group contained 40 participants.
Inclusion and exclusion criteria
The inclusion criteria consisted of 1) being aged ≥60 years and still active, 2) being able to read and write the Thai language, 3) living at least 1 year in the study area, and 4) being willing to participate in the study.
The exclusion criteria were 1) being sick immediately while doing activities in the program, and 2) being unable to participate until the end of the program.
Research tools
This study utilized two tools: a questionnaire and a program focused on modifying the home environment. The questionnaire was developed based on the theoretical concepts, 23 guidelines, 15 and related study reviews19–21 which were composed of 5 parts. Personal characteristics included 8 items about the data of the older adults. Knowledge about home environmental modification was assessed with 10 true or false questions, giving a 1 score for each correct answer and a 0 score for each incorrect answer. Social support on home environmental modification consisted of 10 “5-level scale” questions starting from never, rarely, sometimes, often, and always, with the score ranking from 1 to 5. Home environmental modification was a 20 yes-no question: giving 1 score for the “yes” answer and 0 score for the “no” answer. Falls were assessed by the questionnaire, where an answer of “yes” was given a 1 score and “no” was given a 0 score. Falls refer to any type of falls, including mild, moderate, or severe conditions that occurred inside and outside the home areas of older adults 3 months before the intervention (baseline) and 3 months after the intervention started (outcome). All questions with an item objective congruence (IOC) index greater than 0.5 were considered to meet the standard criteria of the validity test. The reliability of the questionnaire was evaluated among 30 respondents who were not included in the study. The reliability test of social support was evaluated by Cronbach’s alpha coefficients. Knowledge and home environmental modification were assessed by the Kuder-Richardson Formula 20 (KR-20). 26 The reliability of knowledge, social support, and home environmental modification of the questionnaire was 0.74, 0.81, and 0.76, respectively.
The program on home environmental modification for fall prevention in older adults was developed from the guidelines of the Ministry of Public Health
15
and social support theory.
23
The program was verified by 5 experts in the fields of public health, environmental health, and geriatrics. We implemented the program for the experimental group within 12 weeks as follows. Week 1 aimed to educate the experimental group about the physical and mental changes, as well as the health problems, that occur in older adults. Week 2 proposed to train the experimental group on how to assess and analyze the risk of falls in older adults. Week 3 provided concepts and principles of home environmental modification. In this step, the research team demonstrated and allowed the participants to practice home environmental modification. (Weeks 1, 2, and 3 were conducted by the researchers for 3 hours per activity at the subdistrict health promoting hospital in the study area.) Week 4, the participants evaluated problems and obstacles after modifying the home environment at their houses. Week 5 provided knowledge for village health volunteers, caregivers, and healthcare providers about the home visit process to support information and suggestions about home environmental modification to the participants and their relatives when doing home visits. The researchers trained these participants for 3 hours at the subdistrict health promoting hospital. Weeks 6-11, village health volunteers, caregivers, and healthcare providers did home visits every 2 weeks (3 times) in the villages where the participants were located. The home visit included evaluation of home environmental modification, suggestions, and providing help to the experimental group if needed. Weeks 12, we followed up both groups to assess knowledge, social support, home environmental modification, and falls.
In this study, the control group received only routine suggestions about general health problems from village health volunteers when they made home visits about once a month.
Data collection
Pre-intervention stage: After the study was approved for conducting by the Human Research Committee of Naresuan University International Review Board, we then coordinated with the District Health Office in the study area to request permission to implement the program. Later, we met the directors of a subdistrict health promoting hospital that took responsibility for the study area to inform the objectives and steps for data collection. Next, we made an appointment with the study subjects to explain the research objectives, procedures, and ethical issues, including the consent to participate in this research. The written informed consent was provided for the participations. After the participants signed a consent form, the researchers explained to the experimental group and the control group separately about the objectives and process of this study. Participants were then requested to complete the questionnaire (pretest). The first data collection was conducted separately among the experimental group and the control group. Once the questionnaires had been completed, the researchers made an appointment with the experimental group to participate in the program.
Intervention stage: The program was carried out without blinding. Following this, the researchers implemented the program for the experimental group until it was completed (12 weeks). Subsequently, the second data collection (posttest) was performed at the end of week 12 after the program ended to assess the effects of the program in the experimental group and the control group, including knowledge, social support, home environmental modification, and falls. The researchers rechecked all completed questionnaires for quality control for data analysis.
After the study was completed, the researchers also visited the control group to implement the home environmental modification program for fall prevention, since it was effective in preventing falls in older adults. This process was not in the study design; however, it was for ethical considerations.
Statistical analysis
Personal characteristics and falls were presented by frequency and percentage. Mean and standard deviation (SD) were described for scores of knowledge, social support, and home environmental modification. The normality of data was assessed by the Kolmogorov-Smirnov test. A paired t-test was used to compare mean scores of knowledge, social support, and home environmental modification before and after the intervention within the experimental group and the control group. Independent sample t-test compared mean scores of knowledge, social support, and home environmental modification before and after the intervention between the experimental group and the control group. The chi-square test was calculated to see the difference in personal characteristics and falls between the experimental group and the control group. The risk in the control group and in the experimental group was calculated to estimate the relative risk (RR). The risk difference of falls between the control group and the experimental group explained the effect of the intervention program. McNemar’s test compared the difference in falls before and after the intervention within the experimental group and the control group. ANCOVA (Analysis of Covariance) was explored for primary analysis of baseline imbalances to ensure the reported effects of the home environmental modification program. A p-value <0.05 was considered statistically significant.
Results
Personal characteristics of the participants
The comparison of personal characteristics between the experimental group and the control group (Chi-square test) (n= 80).
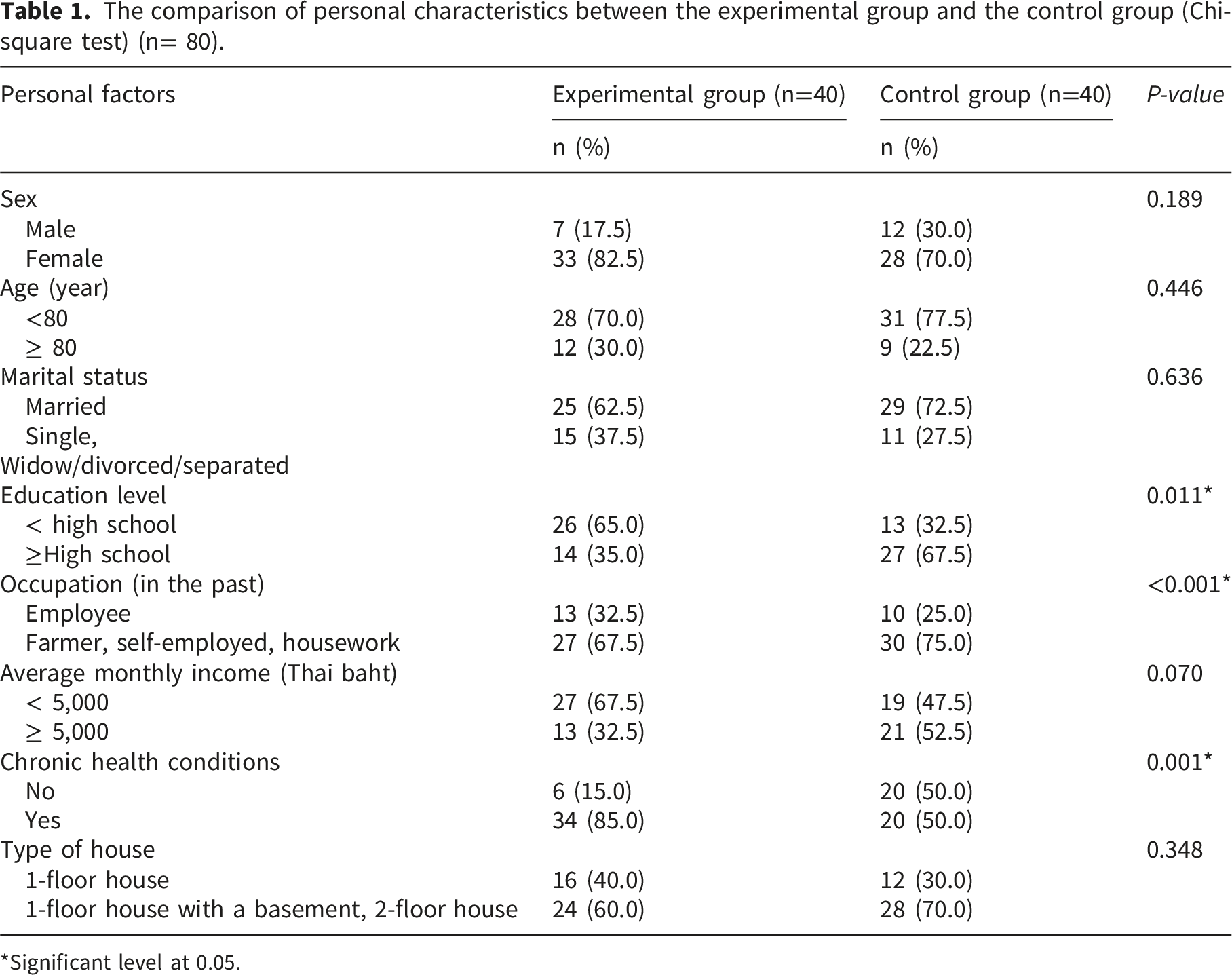
*Significant level at 0.05.
In the control group, 70.0% were female, and 77.5% aged less than 80 years. Most of them (72.5%) were married, and 67.5% finished high school or higher. Seventy-five percent were farmers, self-employed, or housework, and 52.5% had an average monthly income of more than 5,000 Thai baht. Half of them (50.0%) had chronic health conditions, and 70.0% lived in a 1-floor house with a basement or a 2-floor house (Table 1).
The comparison of personal characteristics between the experimental group and the control group indicated that education levels, occupation, and chronic health conditions were significantly different (p<0.05) (Table 1).
Comparison of knowledge, social support and home environmental modification
Comparison of mean scores of knowledge, social support modification, and home environmental modification compared between groups after the intervention, and within groups before and after the intervention (n= 80).

*Statistically significant (p-value < 0.05); gr. = group; SD = standard deviation.
Comparison of falls in older adults
The comparison of falls between groups after the intervention, and within groups before and after the intervention ((n= 80).

*Statistically significant p-value < 0.05; gr. = group, 95%CI = 95% confident interval; RR = relative risk.
Discussion
This study found that after the intervention, the experimental group had significantly higher mean scores in knowledge about home environmental modification, social support, and home environmental modification compared to before the intervention and compared to the control group (p < 0.05). Furthermore, the proportion of falls in the experimental group was significantly lower than before the intervention and lower than in the control group (p<0.05). However, there may have been a random error in our study, as there were imbalances in baseline characteristics (education level, occupation, and chronic health condition) between the groups. However, the previous study reported that these three factors were not associated with fall prevention behaviors among older adults. 27 Although baseline imbalances were observed, these variables were controlled for in the primary analysis using ANCOVA to ensure that the reported effects of the home environmental modification program remained robust. Furthermore, the magnitude of the improvement in fall prevention behaviors in the experimental group was substantially higher than what could be attributed to these baseline differences alone, suggesting that the program itself was the primary driver of change.
After the intervention, the experimental group had a significantly higher mean score of knowledge about home environmental modification than the control group. It was consistent with the previous study. 21 This might be because our program provided knowledge and skills about home environmental modification for the experimental groups to learn and practice. In addition, the experimental group could assess health conditions related to fall risks, such as physical deterioration and its impacts. These helped the experimental group have a greater chance of perceiving the risk of falls and their consequences. As a result, the experimental group gained more knowledge about home environment modification than the control group.
This study revealed that the experimental group had a significantly higher social support mean score than the control group. This finding was similar to the previous studies,28,29 which reported that the experimental group had a significantly higher social support mean score for changing their behaviors after the intervention. The increase in social support mean score in the experimental group might be due to the fact that our program was the organized participation of social support from key community persons such as village health volunteers, caregivers, and healthcare providers. These three groups were important in supporting older adults and their relatives in fall prevention in the community. Therefore, the experimental group had more opportunities to receive information, suggestions, or instruments about home environmental modification from these key persons when having home visits.
We found that the experimental group had a significantly higher mean score for home environmental modification than the control group. It was the same as the findings of the previous study. 20 After the experimental group gained knowledge and skills about home environmental modification from the program, they were more confident than the control group in modifying the environment in their houses. The experimental group also received more suggestions about home environment modification than the control group since village health volunteers, caregivers, and healthcare providers gave them when doing home visits. Moreover, these key persons evaluated the improvement of the home environment in the experimental group 3 times before the program ended. If the experimental group needed help, they could request it from the home visit team. The significant improvement in home environmental modifications observed in this study can be attributed to the sequential integration of theoretical knowledge and practical skill-building within the 12-week program. Specifically, the hazard assessment and analysis training in Week 2 empowered participants to transition from passive recipients of information to active evaluators of their own living spaces. This cognitive skill was further solidified in Week 3 through hands-on practice, where participants moved beyond ‘knowing’ what to change to ‘knowing how’ to implement those changes safely. Furthermore, the reflective evaluation in Week 4, where participants identified obstacles in their own homes, served as a crucial bridge between the classroom and real-world application. By focusing on problem-solving skills and providing continuous reinforcement through trained village health volunteers and caregivers (Weeks 6–11), the program ensured that the knowledge taught was not only retained but effectively translated into physical modifications. This multi-layered approach highlights that risk-awareness and self-evaluation skills are as vital as the physical materials used for fall prevention.
The program in this study reduced falls more than the programs in the previous study, 22 which reported a fall reduction between 11% and 26%. The control group experiences more falls than the intervention group. The finding in our study is in line with the previous studies.30,31 This might be due to the home environment in the experimental group being modified appropriately to prevent the risk of falls. Particularly, the experimental group modified their houses to good levels, such as having sufficient light on the stairs, in the restroom, and at doors, keeping the corridors of the houses clear of objects, having the same floor levels between the inside and the outside of the houses, and installing grab bars. 32 These might prevent falls since older adults could move around more conveniently. 33 The experimental group also received home visits from the key persons in the program to give them suggestions and knowledge. In contrast, the control group had less knowledge and fewer skills to modify the environment around their houses. As a result, the control group tended to have more falls than the experimental group. Consequently, after the intervention, the proportion of falls in the experimental group decreased significantly, whereas no difference was found in the control group.
Limitations and strengths
Our intervention program involved social support from village health volunteers, caregivers, and healthcare providers to observe the problems and give advice to older adults and their relatives for home environmental modification when doing home visits. These are very crucial for older adults to modify their home environment appropriately. As a result, the program can reduce falls by 27.5%. The results of this study can be generalized to older adults in other parts of northern Thailand since we selected settings and participants representing the same social context as this area. These are the strengths of our study. The limitation that may influence the outcome is other activities we did not explore in the program, such as physical activities and fall perceptions. We performed a quasi-experimental study that faced limitations related to reduced internal validity and an inability to definitively establish causation due to the absence of random group assignments. This lack of randomization may lead to selection bias and permit confounding variables to impact the results. Further, the self-developed questionnaire used in this study did not undergo advanced psychometric evaluations such as exploratory or confirmatory factor analysis. This may present a limitation in terms of the construct validity of the instrument and measurement robustness. Future research should consider a more rigorous psychometric validation of the scales to ensure the applicability across broader populations.
Conclusions
The program on home environmental modification using social support was effective in preventing falls in older adults in northern Thailand. After the intervention, the experimental group had significantly higher mean scores of knowledge, social support, and home environmental modification compared to their pre-intervention and the control group. The program can reduce falls by 27.5% and the control group was more likely to have falls 6.00 times than the experimental group after the intervention. This program can serve as a framework for fall prevention among older adults in northern Thailand and similar areas. Future research should incorporate physical activities and perceptions of falls into the program, evaluate fall occurrences over a longer period, and employ qualitative methods for deeper insights.
Clinical implications
The findings of this study provide a practical framework for integrating fall prevention into existing community health infrastructures. The clinical and public health implications are as follows. 1. Integration with Primary Care Networks: This 12-week program demonstrates that fall prevention is most effective when it moves beyond the hospital. By utilizing Subdistrict Health Promoting Hospitals (SHPH) as training hubs (Weeks 1–3), healthcare providers can shift from reactive care to proactive home-based risk management. 2. Empowering the Volunteer Ecosystem: A key implication is the formalization of the role of village health volunteers (VHVs). Instead of general check-ups, VHVs can be trained as “Home Safety Monitors.” This study shows that providing structured 3-hour training (Week 5) enables them to provide targeted social support and technical suggestions, making the intervention sustainable without requiring constant presence from specialized medical staff. 3. Standardizing Home Visit Protocols: The monitoring system (Weeks 6–11) serves as a model for “Integrated Care.” Clinical practice can adopt these structured follow-up schedules to ensure that home modifications are not just “one-time fixes” but are maintained through continuous social reinforcement and professional guidance. 4. Cultural and Contextual Adaptation: Specifically in Northern Thailand, where housing structures (e.g., high thresholds, slippery surfaces) and extended family dynamics are unique, this program suggests that clinical advice must be paired with hands-on demonstration and family caregiver involvement to improve adherence and reduce fall incidence effectively.
Supplemental material
Supplemental material - Effects of a home environmental modification program for fall prevention among older adults in Northern Thailand: A quasi-experimental study
Supplemental material for Effects of a home environmental modification program for fall prevention among older adults in Northern Thailand: A quasi-experimental study by Archin Songthap, Pattama Suphunnakul and Jutarat Rakprasit in Journal of Public Health Research.
Footnotes
Acknowledgements
The research team thanks all participants, organizations, and stakeholders in the study setting for supporting and cooperating with the research project until its completion. We thank Thailand Science Research and Innovation (TSRI) for financial support for this study.
Ethical considerations
This study was approved by the Naresuan University Institutional Review Board with a certificate of approval (Ref No. P3-0178/2022). Informed consent was obtained from all subjects. All methods were undertaken according to the Declaration of Helsinki.
Consent to participate
In accordance with the COPE guidelines, written informed consent was obtained from all participants or their legally authorized representatives prior to their participation in the study. The confidentiality of the participants was strictly maintained throughout the research process.
Author contributions
The authors have contributed to the manuscript as follows: A S: The principle investigation optimized the study proposal and protocol, conceptualization, supervision, project administration, methodology, formal analysis, writing, review, and editing. P S: Data curation, writing original draft preparation, investigation, and validation. J R: investigation, validation, and data collection. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Thailand Science Research and Innovation (TSRI) (grant number: FRB650022/0179).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Significance for public health
Falls in older adults is one of the major public health problems and are the second leading cause of unintentional injury deaths worldwide. Our study was conducted using a quasi-experimental study to implement a home environmental modification program for fall prevention among older adults in the community using social support from village health volunteers, caregivers, relatives, and healthcare providers. After the intervention, the experimental group had significantly higher mean scores of knowledge, social support, and home environmental modification than before the intervention, and the control group. The program can reduce falls by 27.5% and the control group was more likely to have falls 6.0 times than the experimental group after the intervention. The program can be utilized as a guideline to prevent the incidence of falls and their consequences for older adults in northern Thailand and other regions appropriately.
Supplemental material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.