
Abstract
Evidenced-based community falls prevention programs can reduce falls in older adults. We sought to (1) describe the characteristics of program participants who met completion criteria by receiving the full program dose (completers) versus those who did not (non-completers), and (2) determine the differences in outcomes (falls, fear of falling and physical function) between the two groups. Data from ten programs from 2014–2019 were evaluated. Completers were older and reported more fear of falling and lower perceived health at baseline. A higher proportion of completers had reduced falls, decreased fear of falling, and were more likely to take actions to reduce fall risk. Both groups improved in physical function with no evidence of a difference between groups. While completers gained a greater benefit, both groups demonstrated a fall risk reduction. A larger loss of non-completers to follow-up may have impacted results. Targeting programs for individuals may improve completion rates.
Introduction
Falls are a significant health concern for older adults in the United States (US), with 14 million older adults reporting a fall in 2020 (Kakara, 2023). Falls are the leading cause of serious injury for people over 65 and fall injuries can result in loss of independence and mortality (Kakara, 2023; Vaishya & Vaish, 2020). Fall risk screening and fall prevention programs can reduce the incidence of falls (Brach et al., 2022; Johnston et al., 2019).
Evidenced-based falls prevention programs, which are programs evaluated by research and disseminated into community settings, aim to reduce falls and fall risk (Brach et al., 2022). Programs are offered as workshops or weekly classes (fixed duration and ongoing) and contain a variety of educational and exercise training interventions. The Administration for Community Living (ACL) awards grants to eligible US organizations (i.e., non-profits, state and local governments, community agencies, universities, tribal organizations) to implement falls prevention programs for older adults that meet ACL’s evidenced-based definition (Administration for Community Living, 2024; Kulinski et al., 2017). In 2023, ACL awarded eight organizations four-year grants totaling $4.3 million. The ACL awarded more than $50 million since the inception of the program in 2014 (Administration for Community Living, 2024).
Grantee falls prevention programs reached more than 85,000 participants in the first five years of the program (2014–2019) (Brach et al., 2022). These programs reduced fear of falling, self-reported falls, and self-reported falls resulting in injury (Brach et al., 2022). Remaining unknown is the impact of receiving the full intended dose of the program and the characteristics of those who complete the programs. Understanding the characteristics of program completers and non-completers and their outcomes post-program can influence dosage, recruitment and retention strategies.
We sought to (1) describe and compare the characteristics of ACL evidenced-based community falls prevention program participants who met completion criteria by receiving the full program dose (completers) and those that did not (non-completers), and (2) examine the differences in outcomes (falls, fear of falling and physical function) between the two groups. Our hypothesis was that completers would have better post-program outcomes (reduced falls, reduced fear of falling and better physical function) than non-completers.
Methods
Evidence-Based Program Repository
The ACL provides funding to the National Falls Prevention Resource Center to maintain a national administrative database of evidence-based falls prevention programs and participants. The database holds standardized program performance monitoring data which is required by the ACL for falls prevention grantees who receive funding (National Council on Aging, 2023). While organizations not receiving funding are not required to report data into the database, some voluntarily provide data. Data is collected by program leaders and host organizations, and entered into the central repository (Kulinski et al., 2017).
Programs with data provided in the repository include both education-focused programs (FallScape, Matter of Balance, and Stepping On) and exercise-focused programs (Enhance Fitness, Health Steps in Motion, Otago Exercise Program, Tai Chi for Arthritis, Tai Ji Quan-Moving for Better Balance, Stay Active and Independent for Life, and Stay Safe, Stay Active). Details on the individual programs’ format, duration, and intended outcomes are provided in supplemental table 1.
Data and Analysis
Data were collected pre- and post-program and included demographics, participant perception related to falls, self-reported falls (in previous three months pre-program and since the program started post-program). Physical function measures were collected in some programs. Study data spans September 2014 to December 2019. Participant perception was measured via surveys and included confidence in falls-related activities, number of falls, fear of falling, confidence in avoiding falls and actions taken to reduce falls (e.g., changes in the home, exercise, medication review, vision and healthcare screening, talking with loved ones about fall risk). Some programs also collected data on participant’s physical function that can predict fall risk including the Timed Up and Go (TUG, mobility) and repeated chair stands (functional strength). During the TUG, participants are timed for how long it takes them to stand up from a chair, walk ten feet, turn around, walk back to the chair, and sit back down. A time longer than 12 seconds suggests a higher risk of falls (Lusardi et al., 2017). The repeated chair stand test, also known as the 30 second sit to stand (30STS), measures the number of times a participant can rise from a chair and sit back down in 30 seconds (Jones et al., 1999). Age-based norms are provided; for example, less than 12 repetitions for men and 10 repetitions for women ages 70–74 suggest increased fall risk (Centers for Disease Control and Prevention, 2024; Jones et al., 1999) General norms for all people over age 65 are consistent with the age-based norms with a cutoff of 11 repetitions separating fallers from non-fallers (Roongbenjawan & Siriphorn, 2020).
Data were stratified by those participants who met the program completion criteria (completers) and those who did not (non-completers). A completer met the criteria of a full dose, which was either defined by the program designers or otherwise defaulted to two-thirds of the total sessions. Other data collected from participants include demographics, falls, perception of fall risk, and actions taken to prevent falls. A subset of programs also measured mobility and balance.
We used appropriate descriptive statistics to summarize the number of sessions attended by completers and non-completers of each program. We also used descriptive statistics to summarize participant demographic, health, fear, confidence and fall characteristics for completers and non-completers. The same was repeated for completers and non-completers restricted to those with post-completion assessments, which were compared using independent samples t- and chi-square tests, as appropriate based on data. Separately for completers and non-completers, we used Bowker’s symmetry tests to assess the statistical significance of pre- to post-program changes in fear of falling, number of (injurious) falls, and measures of confidence while accounting for the paired nature of data. We used chi-square tests to compare the proportion of participants with improvement between completers and non-completers. Finally, using a subset with available data, we used paired samples t-tests to assess significance pre- to post-program changes in physical function among non-completers, and independent samples t-tests to compare changes between completers and non-completers. SAS® version 9.4 (SAS Institute, Inc, Cary, NC) was used for all statistical analyses.
Results
Completion Status by Program
Participant Completion Rates and Attendance of Evidence-Based Falls Prevention Programs.
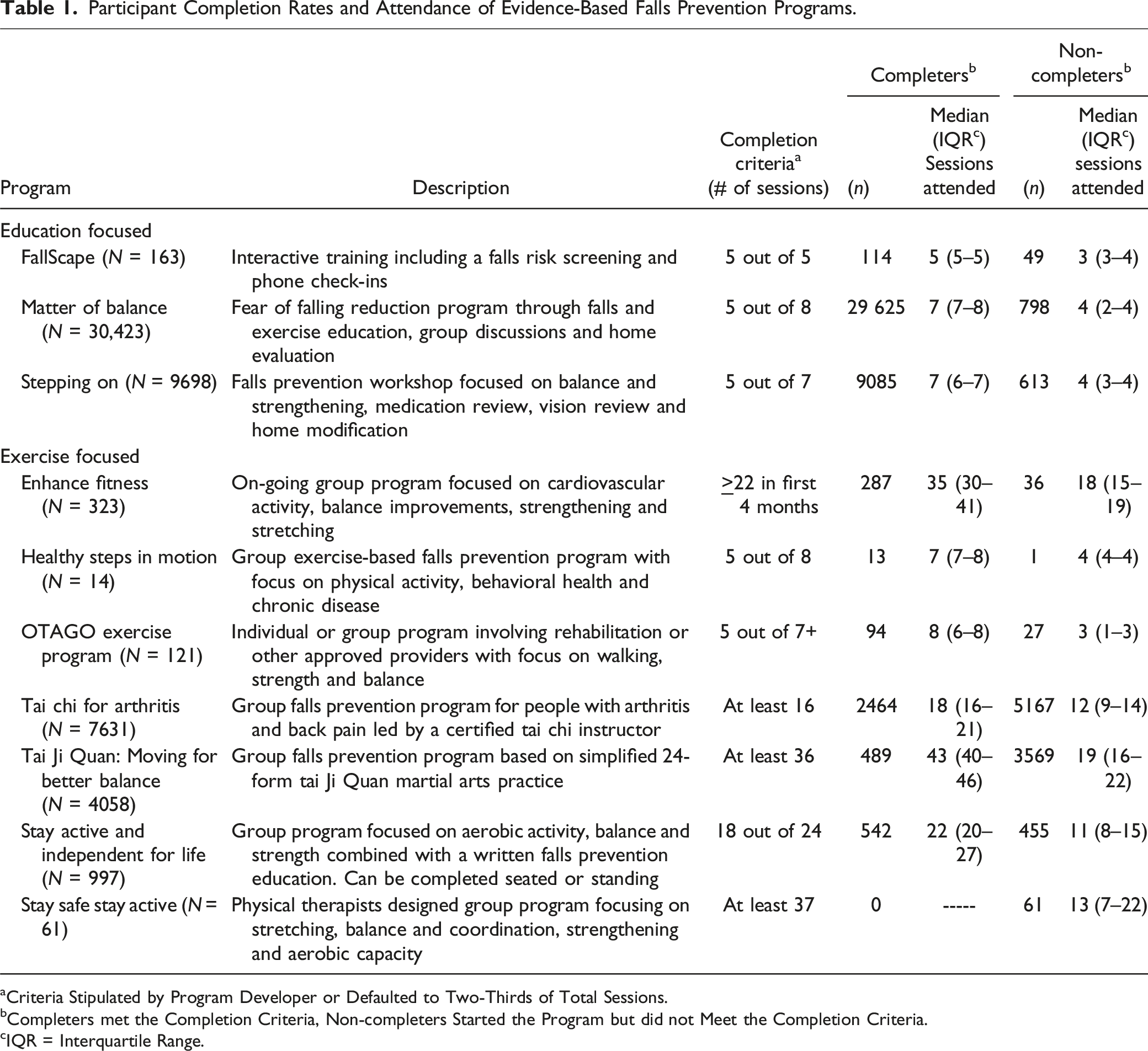
aCriteria Stipulated by Program Developer or Defaulted to Two-Thirds of Total Sessions.
bCompleters met the Completion Criteria, Non-completers Started the Program but did not Meet the Completion Criteria.
cIQR = Interquartile Range.
Participant Demographics
Demographics of Completers and Non-completers for Evidence-Based Falls Prevention Programs.
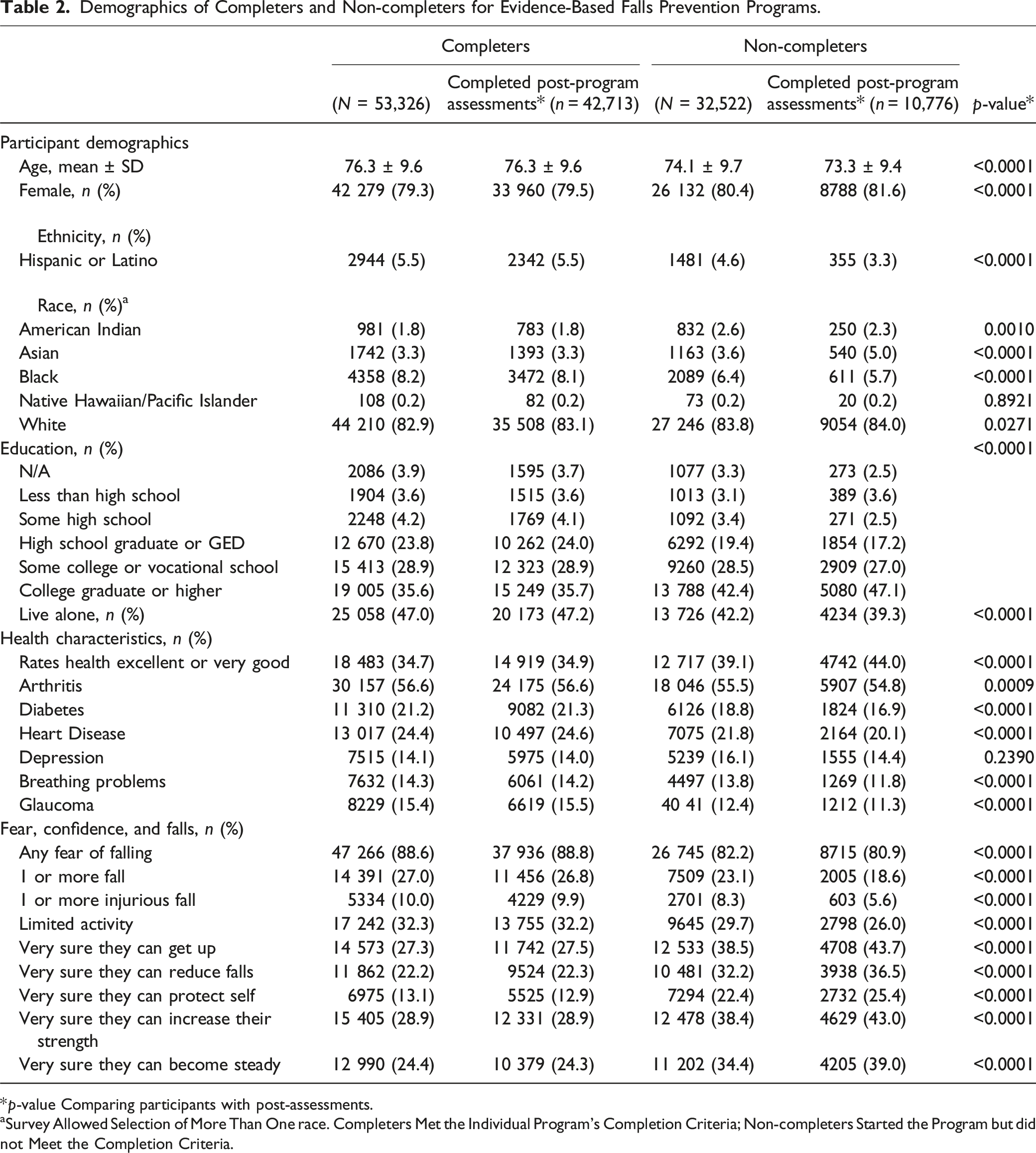
*p-value Comparing participants with post-assessments.
aSurvey Allowed Selection of More Than One race. Completers Met the Individual Program’s Completion Criteria; Non-completers Started the Program but did not Meet the Completion Criteria.
Changes in Falls and Falls Risk
Fear of Falling, Falls Reported and Injurious Falls Reported
A higher proportion of completers reduced their fear of falling compared to non-completers (34 vs. 25%), as well as reducing the number of falls (23% vs. 15%). A lower proportion of completers compared to non-completers had no change in their fear of falling (50% vs. 56%) and no change in number of falls reported (70% vs. 77%) (Figure 1 and Supplemental Figure 1). Change in fall status indicators for completers and non-completers of falls prevention programs.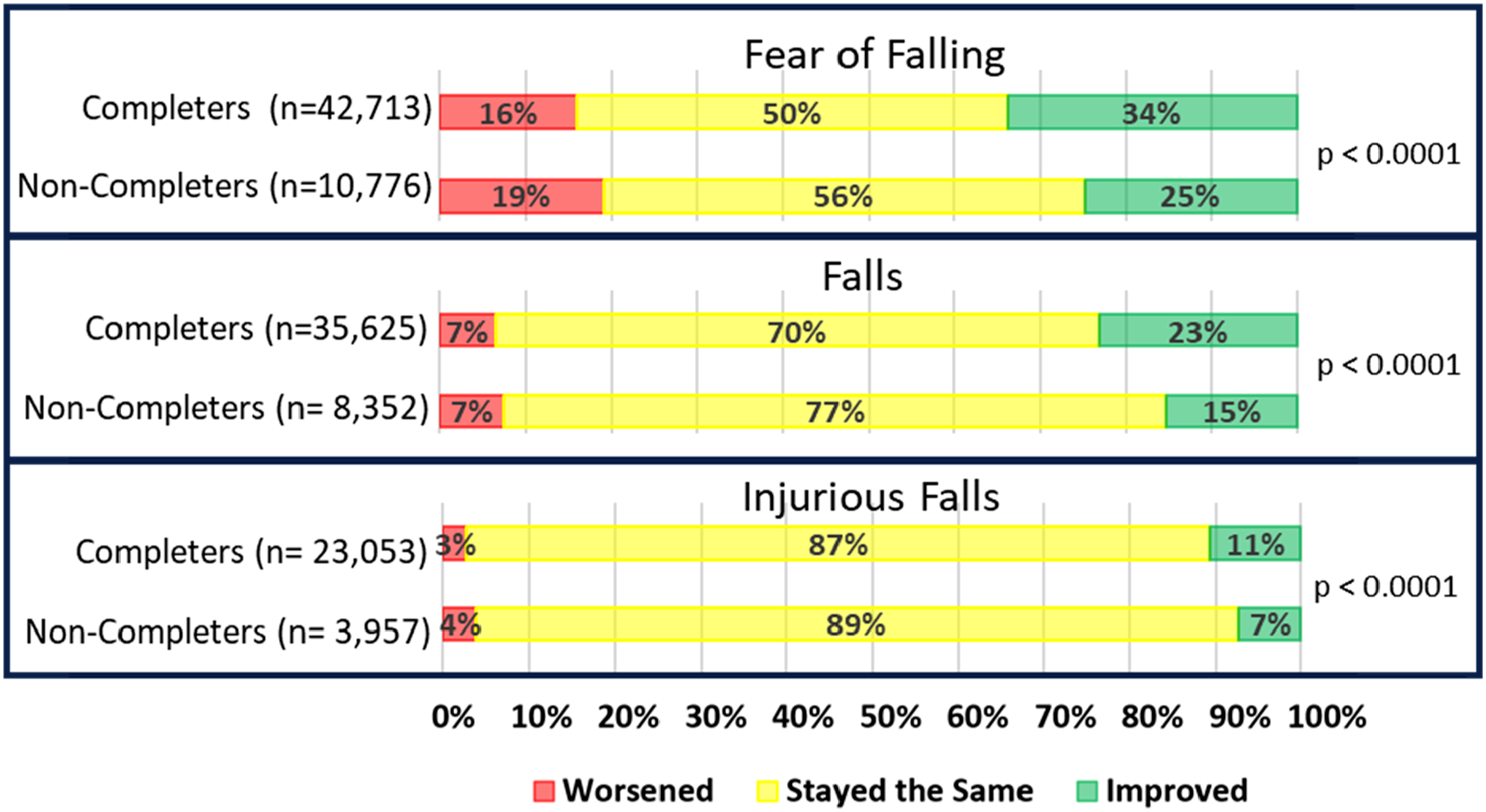
Falls Confidence
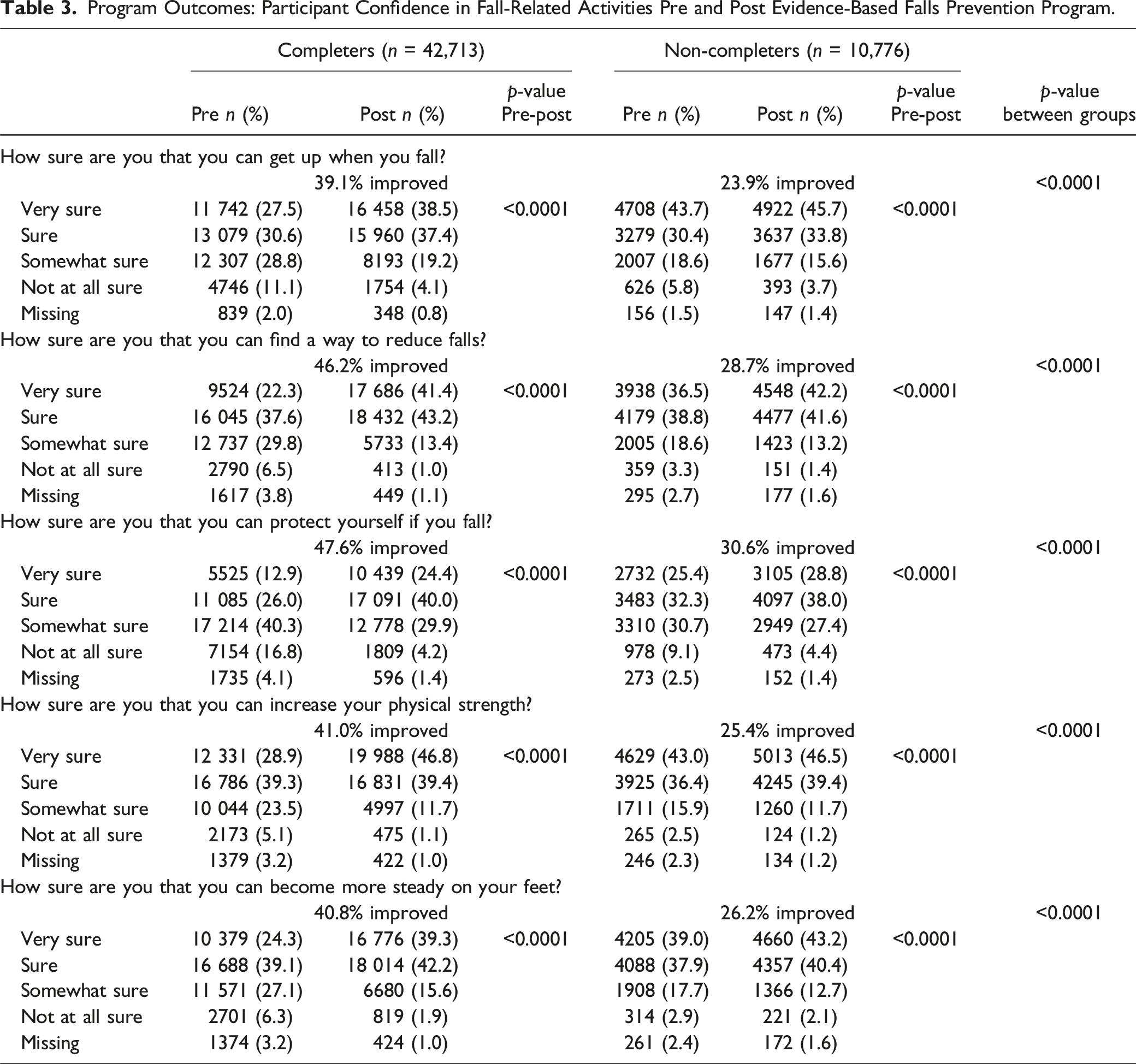
Program Outcomes: Participant Confidence in Fall-Related Activities Pre and Post Evidence-Based Falls Prevention Program.
Actions to Reduce Fall Risk
Completers were more likely to declare they intended to take actions to reduce falls post-program than non-completers (Figure 2). Completers were more likely than non-completers to state they would make changes in their home (42% vs. 27%), complete exercises at home (63% vs. 52%) and talk to someone about reducing fall risk (48% vs. 38%). Actions taken to reduce falls by completion status. Completers N = 42, 713; Non-Completers N = 10,776.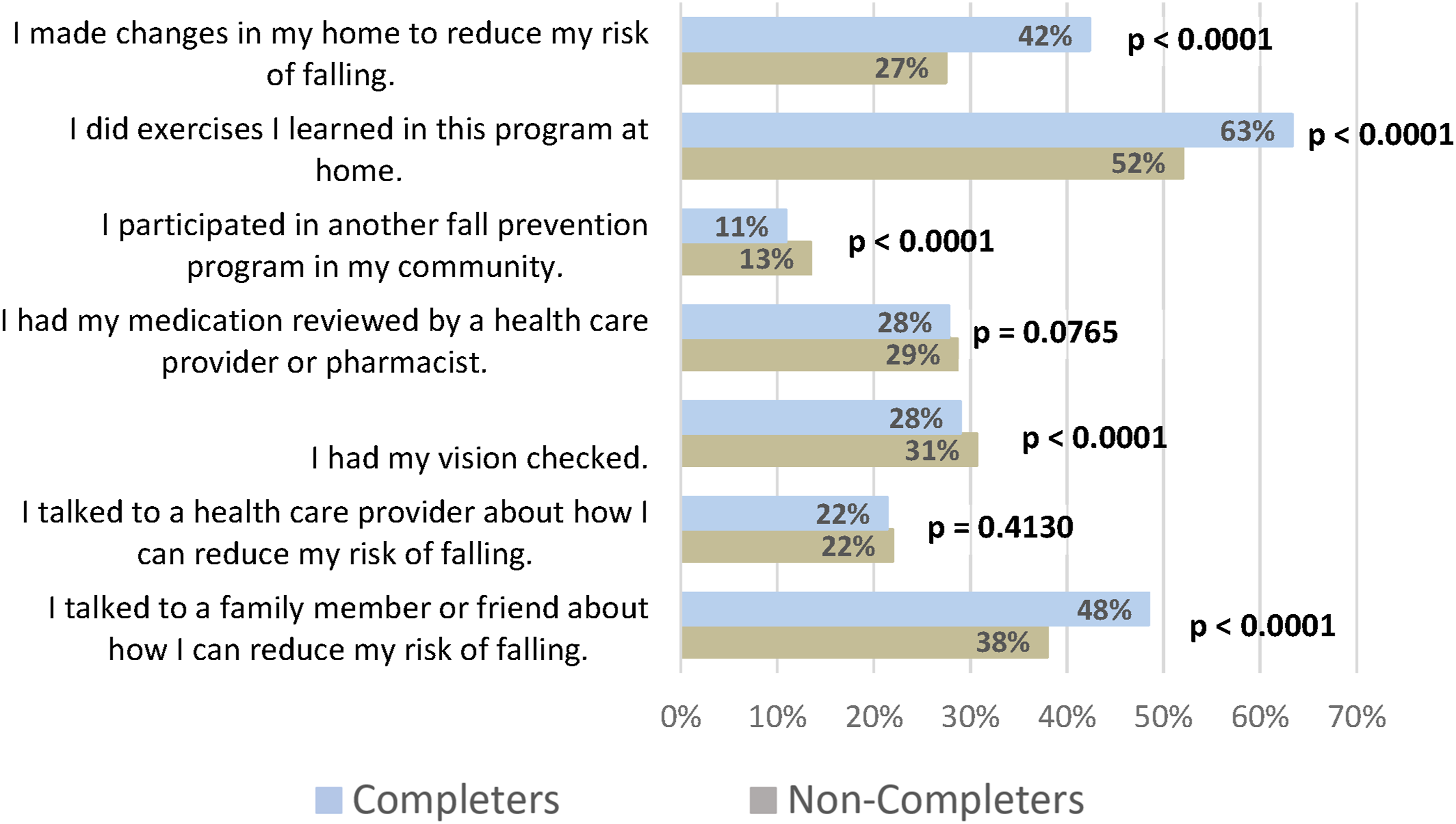
Changes in Physical Function Measures Related to Fall Risk
Pre- to Post-program Change for Timed Up and Go and Repeated Chair Stands by Program Completion Status.
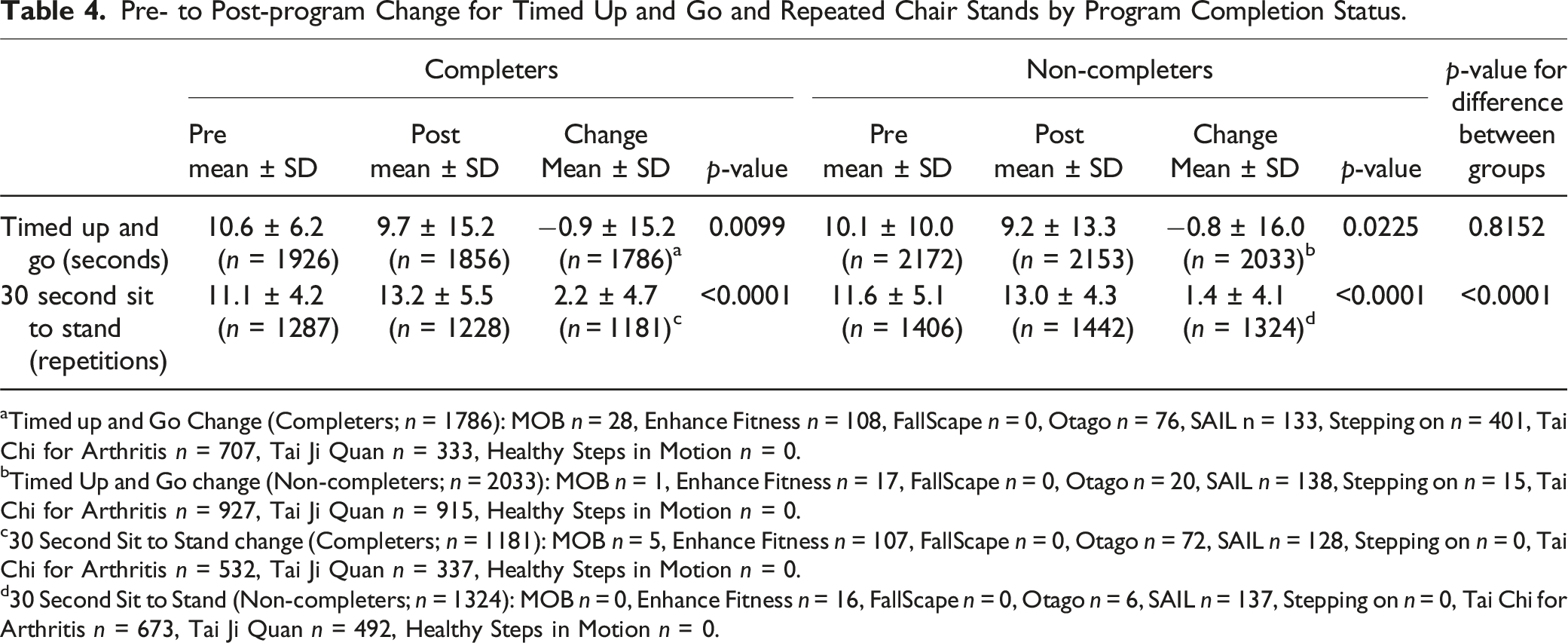
aTimed up and Go Change (Completers; n = 1786): MOB n = 28, Enhance Fitness n = 108, FallScape n = 0, Otago n = 76, SAIL n = 133, Stepping on n = 401, Tai Chi for Arthritis n = 707, Tai Ji Quan n = 333, Healthy Steps in Motion n = 0.
bTimed Up and Go change (Non-completers; n = 2033): MOB n = 1, Enhance Fitness n = 17, FallScape n = 0, Otago n = 20, SAIL n = 138, Stepping on n = 15, Tai Chi for Arthritis n = 927, Tai Ji Quan n = 915, Healthy Steps in Motion n = 0.
c30 Second Sit to Stand change (Completers; n = 1181): MOB n = 5, Enhance Fitness n = 107, FallScape n = 0, Otago n = 72, SAIL n = 128, Stepping on n = 0, Tai Chi for Arthritis n = 532, Tai Ji Quan n = 337, Healthy Steps in Motion n = 0.
d30 Second Sit to Stand (Non-completers; n = 1324): MOB n = 0, Enhance Fitness n = 16, FallScape n = 0, Otago n = 6, SAIL n = 137, Stepping on n = 0, Tai Chi for Arthritis n = 673, Tai Ji Quan n = 492, Healthy Steps in Motion n = 0.
Discussion
The baseline characteristics of falls prevention program completers and non-completers were different. Non-completers tended to be younger, more educated, self-rated healthier, less likely to report fear of falling and more likely to report less falls. Other baseline demographic and health measures were significantly different between completers and non-completers with post-program assessments. These small differences need to be interpreted with caution as they are likely due to the large sample size and the resulting statistical power rather than truly meaningful differences (Brach et al., 2022).
Non-completers had better baseline falls-related characteristics (less reported falls, better confidence in fall-related activities, reduced fear of falling) compared to completers, which may have impacted their decision not to complete programs. The non-completers also had better baseline falls risk profiles which left less room for improvement compared to completers. These findings of completers having more complicated fall risk profiles are consistent with previous studies on falls prevention program adherence. Prior researchers concluded that if falls had an extreme interference with social activities or participants had lower baseline functional mobility (lower TUG scores), participants had better adherence (Batra et al., 2013; Davis et al., 2021). This phenomenon is noted in other health education programs as well. A systematic review of diabetes education programs found that two major reasons for non-attendance were no perceived benefits, and the belief of already having enough knowledge on the topic (Horigan et al., 2017).
Completers improved their fall risk indicators more than non-completers. However, both groups had improvements. With these findings of clinically relevant improvement even with partial dosages, it is important to consider that fall risk may be reduced even with lower than target doses.
Both completers and non-completers improved in physical function characteristics. However, both groups had baseline average TUG scores below and 30STS repetitions above fall risk cutoffs suggesting lower risk even at baseline. Current study findings suggest using these physical function screening measures alone to assess fall risk could potentially misclassify individuals as low risk. Our findings support the need for a multifactorial approach to fall risk assessment for more accurate classification and recommended interventions. The American Geriatrics Society prefers screening and classifying as risk or no risk, rather than the World Falls Guidelines of high or low risk (Eckstrom et al., 2024). Both guidelines have screening questions, (e.g., fear of falling, falls) and physical function measures (e.g., TUG, gait speed) recommendations as part of a screening at least annually (Eckstrom et al., 2024; Montero-Odasso et al., 2022). For those at risk with mobility concerns, a tailored individual approach led by a physical therapist is recommended by the American Geriatrics Society and supported by the World Falls Guidelines (Eckstrom et al., 2024; Montero-Odasso et al., 2022).
While both education-focused programs and exercise-focused programs have evidence to support fall risk reduction, their mechanisms and outcomes are distinct. Education focused programs provide information on several characteristics including medication changes, home changes, vision checks, and exercises one can do on their own. While they may include the topic of exercise, it is usually informational or a one-time exercise session only. Participants do not repeatedly exercise with others or with feedback from a trained instructor for multiple sessions like the exercise-based programs. Participants in some exercise-based programs can continue indefinitely by either repeating a fixed-length program or continuing in an ongoing program. Exercise-based programs have additional benefits outside of continued reduced fall risk, including improving overall health, improving quality of life, and promoting socialization for older adults (Izquierdo et al., 2021; Kohn et al., 2016). Collecting data in the future about those who participate on an ongoing basis can provide more comprehensive information on program impact. Additionally, while education-based programs change fall risk indicators immediately post-program, understanding the long-term impact will help to identify if education programs need to be repeated at regular intervals. Data on longer term outcomes on fall risk reduction is limited and mixed at one-year post-program with some showing maintenance of reduced fall risk and others showing no maintenance of benefit (Berggren et al., 2008; Lee et al., 2013; Yoshikawa et al., 2020). A systematic review of exercise-based falls prevention trials with long-term follow-up suggests that benefits can be sustained for up to two years for multi-component programs lasting longer than six months when compared to control (Finnegan et al., 2019). Remaining unknown is the duration of falls risk reduction for education-focused programs and shorter duration exercise-focused programs. More comprehensive information about participants at six months to one-year post-program will provide a deeper understanding of the public health impact of falls prevention programs.
Current study findings suggest that falls prevention programs are most effective for those with higher risk factors including previous falls, fear of falling and lower confidence in fall-related activities. Potentially, recommendations for programs could be individualized after the initial risk assessment to target the most appropriate community programs based on the fall risk profile, exercise habits and interest to get the most benefit and facilitate completion (Robins et al., 2016). While this ideal may not work in communities where there are few community programs, approaching recommendations from a patient-centered perspective could improve initiation of fall risk reduction activities. The Center for Disease Control and Prevention established a primary care screening algorithm in 2017, the Stopping Elderly Accidents, Deaths and Injuries (STEADI) toolkit (Centers for Disease Control and Prevention, 2024). The algorithm classifies older adults as at risk or not a risk and suggests interventions, including community exercise or falls prevention programs for at risk individuals (Centers for Disease Control and Prevention, 2024). The American Geriatrics Society supports the STEADI assessment and further recommends individual evaluation by a physical therapist for those with mobility and balance concerns to stratify high and low risk (Eckstrom et al., 2024). Using the STEADI algorithm and the American Geriatrics Society recommendations as a starting point, program recommendation could be additionally targeted to education-based programs or exercise-based programs or both (Figure 3). Those with falls in the previous year or who are afraid of falling would enter a fall risk category where education and exercise-focused programs would be recommended. Those without falls or fear would receive recommendations for optional exercise-based programs based on their interest. Additionally, for the not at risk category, general group community exercise programs and home-based individual exercise programs could be considered, opening more possibilities to include a person’s preferences (Barmentloo et al., 2020). People may attend a falls prevention program on a short-term basis if they are motivated to reduce falls, but if they do not enjoy or find benefit in certain types of exercise, may not complete the program or not continue on an on-going basis (Collado-Mateo et al., 2021). Offering on-going exercise programming which includes balance components could support long-term behavior change (Finnegan et al., 2019, 2021). Individualizing program recommendations based on risk, existing habits and interest may increase the likelihood of behavior change to reduce fall risk and improve overall health. Refining Stopping Elderly Accidents, Deaths and Injuries (STEADI) Algorithm with fall risk reduction education and exercise (Centers for Disease Control and Prevention, 2024; Eckstrom et al., 2024).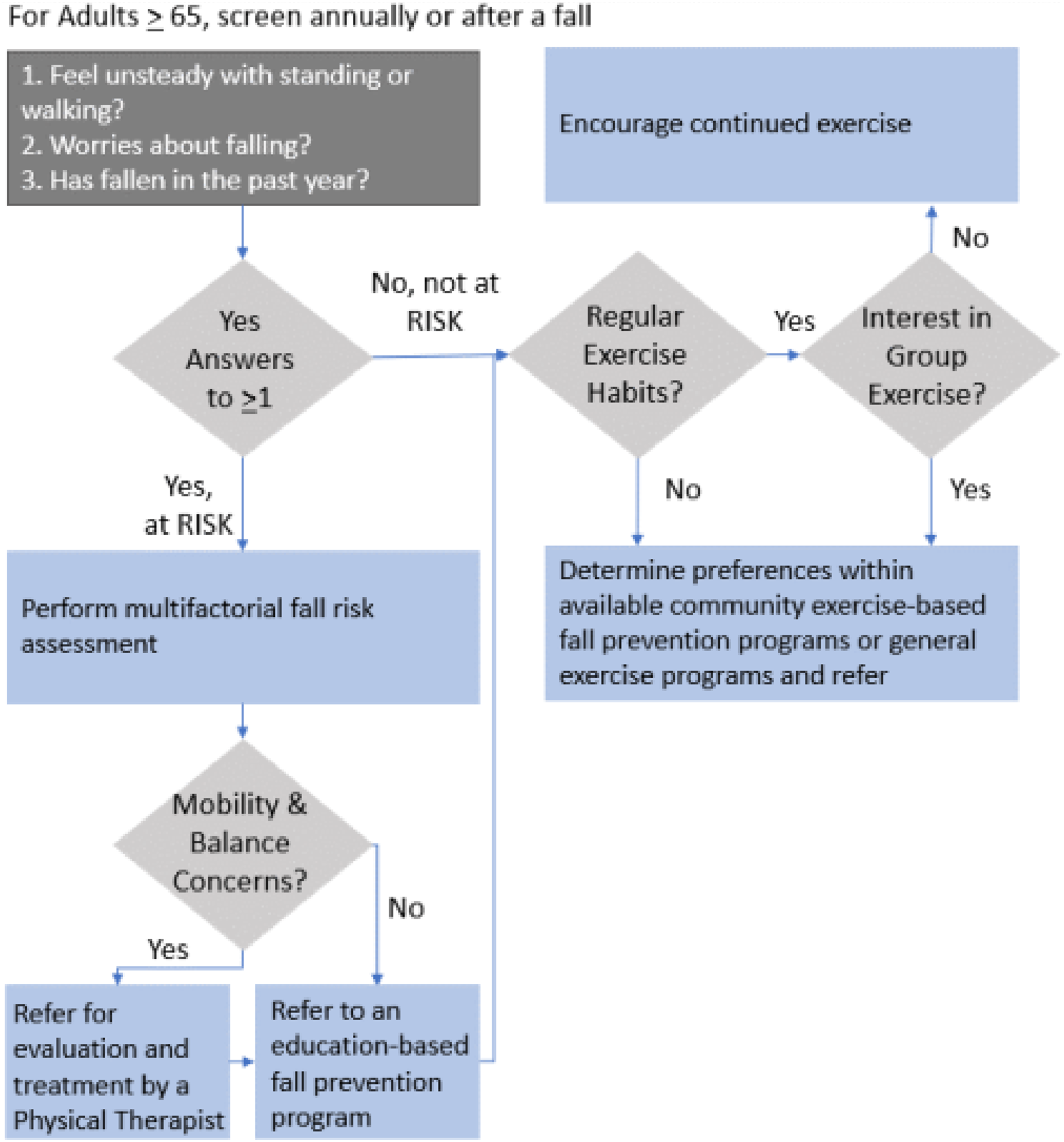
Strengths and Limitations
Strengths of our study include the large dataset of active community implemented evidence-based programs which allows for robust analysis of programs. Notably, we would like to emphasize our data comes from a real-world administrative database rather than data collected for research purposes. Limitations to the present study include data availability, heterogeneity in programs, participants having lower fall risk profiles at baseline, and lack of diversity among the participants. Many participants were lost to follow up: 20% of completers and 67% of non-completers did not complete post-program assessments. While completion of baseline and post-program surveys are encouraged, they are optional and subject to the host organization’s determination. This high loss of data in the non-completers could inflate the outcomes. Further, programs are varied in their intervention approaches, number of sessions and total participants skewing outcomes towards larger programs.
Conclusions
Evidenced-based fall prevention program completers tend to be older and at greater fall risk than non-completers who opt out of programs early. While completers had the greatest benefit, both completers and non-completers demonstrated fall risk reductions and improvements in physical function. Targeting education-focused and exercise-focused programs for individuals based on a multifaceted evaluation of fall risk, current exercise habits and interest may facilitate greater adherence and completion. Further research into long-term outcomes will help to identify the duration of benefit after education-based and limited duration exercise-based programs.
Supplemental Material
Supplemental Material - Characteristics of Evidenced-Based Falls Prevention Program Completers and Non-Completers and Difference in Outcomes
Supplemental Material for Characteristics of Evidenced-Based Falls Prevention Program Completers and Non-Completers and Difference in Outcomes by Elizabeth W. Regan, Kathleen Cameron, Angelica Herrera-Venson, Gardenia A. Juarez, Subashan Perera, Jennifer Vincenzo, and Jennifer S. Brach in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the NIH University of Pittsburgh Claude D. Pepper Older Americans Independence Center (JSP and GAJ), the Foundation of Physical Therapy Research’s Center of Excellence in Physical Therapy Health Services and Health Policy Research and Training Grant (EWR), the Research Registry and Developmental Pilot Grant (P30 AG024827, NIHK76AG074920, NIH R01 AG071520) (P30 AG024827) (JSB and SP), the (NIHK76AG074920) (JLV), and the (NIH R01 AG071520) (GAJ). This publication was supported by the Administration for Community Living (ACL), U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $23,565 funded by ACL/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by ACL/HHS, or the U.S. Government.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.