
Abstract
Background:
Antenatal care (ANC) is essential for ensuring maternal and child health. Despite efforts to improve maternal healthcare in Tanzania, many women still fail to complete the recommended number of ANC visits. This study examines the socioeconomic and demographic determinants influencing ANC utilisation using data from the 2022 Tanzania Demographic and Health Survey (TDHS).
Design and methods:
This study employed a retrospective cross-sectional approach using secondary data from the 2022 TDHS, focussing on women aged 15–49 who had a live birth within 5 years preceding the survey. Poisson regression was applied to identify factors associated with the number of ANC visits. Model fit was assessed using Deviance and Pearson Goodness-of-Fit tests.
Results:
Approximately 89.26% of women attended at least one ANC visit, while only 61.26% completed the recommended minimum of four visits. The average number of visits was 4.00 (variance = 4.06). Poisson regression revealed that Higher maternal education (IRR = 1.3002, p < 0.001) and household wealth in the poorer (IRR = 1.0959, p < 0.001), middle (IRR = 1.1277, p < 0.001), richer (IRR = 1.1624, p < 0.001), and richest (IRR = 1.2514, p < 0.001) were positively associated with increased ANC visits, while larger household sizes negatively affected utilisation. Regional disparities were evident, with women in the Central, Southern, Eastern, and Zanzibar zones attending more ANC visits compared to those in the Western zone. Goodness-of-fit tests confirmed that the model adequately fit the data (Deviance p = 0.2679; Pearson p = 0.9901).
Conclusion:
Despite high initial contact with ANC services, a substantial proportion of women do not complete the full recommended visits. Socioeconomic, demographic, and regional factors significantly influence ANC utilisation. Policies aimed at promoting women’s education, economic empowerment, and equitable access to maternal healthcare, particularly in underserved regions, are essential to improve ANC coverage in Tanzania.
Keywords
Introduction
Antenatal care (ANC) is a crucial component of maternal and child health, aimed at ensuring the well-being of both the mother and the foetus during pregnancy. Globally, ANC utilisation has improved over the past two decades, yet disparities persist, particularly in low- and middle-income countries (LMICs). According to the World Health Organisation (WHO), an estimated 86% of pregnant women worldwide receive at least one ANC visit, but only 65% complete the recommended minimum of four visits. 1 ANC provides essential health services such as nutritional counselling, infection screening, immunisation, and health education that are vital for reducing maternal and neonatal morbidity and mortality.2–4
Despite concerted efforts through regional and national health initiatives, Sub-Saharan Africa continues to experience some of the lowest rates of ANC completion globally. Socioeconomic inequalities, limited access to quality healthcare, and cultural factors contribute to this persistent gap. 5 In East Africa, while countries like Rwanda and Kenya have made notable improvements, others still struggle with ensuring timely and adequate ANC attendance among expectant mothers.
In Tanzania, maternal health remains a major public health concern. Despite policy frameworks such as the National Health Policy and the Reproductive, Maternal, Newborn, Child, and Adolescent Health (RMNCAH) strategy, many women still do not complete the recommended ANC visits.6,7 The 2022 Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) reported that while 89% of women attended at least one ANC visit, only around 65% completed the four or more visits recommended by WHO. 8 This discrepancy underscores the need to understand the determinants of ANC utilisation across different population subgroups.
Previous studies in Tanzania have focussed on the binary outcome of ANC attendance (yes/no) or explored individual factors in isolation, often using traditional logistic regression approaches.9,10 However, there is limited evidence on the count-based modelling of ANC visits using nationally representative data. Few studies have applied Poisson regression to evaluate the frequency of ANC visits in Tanzania, despite its appropriateness for analysing count data.11,12 This methodological gap restricts a comprehensive understanding of the factors influencing repeated ANC visits, which is essential for improving maternal health programs and achieving the Sustainable Development Goal (SDG), particularly target 3.1 which seeks to reduce the global maternal mortality ratio.
Although recent studies increasingly emphasise the timeliness and quality of antenatal care13,14 respectively, the present study specifically focuses on the frequency of ANC visits as a key utilisation indicator. This focus is justified by the continued policy relevance of visit frequency in monitoring maternal health service use in low- and middle-income settings, particularly in population-based surveys such as the Tanzania Demographic and Health Survey. Accordingly, this study applies Poisson regression analysis to the 2022 TDHS-MIS to examine the socioeconomic and demographic factors influencing the frequency of ANC visits in Tanzania, with the aim of informing targeted health interventions and policymaking to improve ANC utilisation and reduce maternal health disparities across the country.
Methodology
Study setting and period
This study utilised secondary data from the 2022 Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS), covering the period from February to July 2022, which corresponds to the survey implementation period as reported by the TDHS team. The nationally representative, cross-sectional survey was conducted by the Tanzania National Bureau of Statistics in collaboration with other government agencies. A multistage sampling design was employed. In the first stage, 629 enumeration areas (EAs), defined during the 2012 Population and Housing Census, were selected comprising 211 urban and 418 rural clusters. In the second stage, 26 households were systematically selected from each cluster, yielding a target sample size of 16,354 households.
For this study, analysis was restricted to a subset of 5802 women aged 15–49 years who had a live birth within the 2 years preceding the survey to reduce recall bias and ensure up-to-date information on ANC utilisation related to the most recent pregnancy. The study population consisted of women within the specified age range (15–49 years) who had complete data on antenatal care (ANC). Women who had not given birth within the reference period and those with missing or incomplete information on ANC utilisation were excluded from the study (Figure 1).

Procedures for sampling and exclusion to determine the final sample size in the TDHS-MIS, 2022.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cross-sectional studies 15 (Supplemental File 1).
Study variables
The outcome variable in this study was the number of antenatal care visits during the most recent pregnancy. Other important dimensions of ANC utilisation, including timeliness of initiation and content of care, were not analysed as primary outcomes and are acknowledged as limitations of the study. Since this is a count variable, it is well-suited for Poisson regression modelling.
Independent variables
The independent variables in this study encompass a range of demographic, socio-economic, and geographic factors that may influence antenatal care (ANC) utilisation. Maternal age and the age of the household head are continuous variables reflecting the age distribution of women and decision-makers in the household. Mother’s education is categorised into four levels: no education, primary, secondary, and higher education, highlighting educational attainment. The household wealth index is divided into five categories, poorer, middle, and richer, indicating economic status. Marital status includes never married, married, and widowed/separated/divorced. The number of living children is grouped as no children, 1–2, 3–4, and 5 or more, representing family size. Place of residence distinguishes between urban and rural settings. The sex of the household head is categorised as male or female. Household size is classified into small (≤3 members), medium (4–6 members), and large (≥7 members). The mother’s and husband’s occupations are categorised as not working, professional, sales/clerical, agriculture, and manual/other. Distance to a health facility is captured as either a big problem or not a big problem, reflecting access to healthcare services. Finally, the geographical zone includes nine regions (Western, Northern, Central, Southern Highlands, Southern, Southwest Highlands, Lake, Eastern, and Zanzibar), allowing for regional comparisons in ANC utilisation.
Model of the study
Given that the dependent variable “Antenatal Care (ANC) Utilisation” is a count variable (Number of ANC visits), the appropriate statistical approach is Poisson Regression. This model is used to examine how various independent variables influence the number of ANC visits made by women during their most recent pregnancy.
Mathematical formula
Let

The Poisson regression links the expected count to a set of explanatory variables using a log-link function:

Where:
Data processing
Data were extracted from the 2022 Tanzania Demographic and Health Survey-Malaria Indicator Survey (TDHS-MIS) and underwent rigorous data cleaning to ensure consistency with the official TDHS descriptive report. Variable recoding, generation, and labelling were performed before analysis. All analyses were conducted using STATA version 18.0.
Statistical analysis
Antenatal Care (ANC) utilisation was operationalised as a count outcome, defined as the total number of ANC visits made by a woman during her most recent pregnancy. Descriptive statistics (frequencies, percentages, means, and standard deviations) were used to summarise respondents’ characteristics and the distribution of ANC visits.
Bivariate analyses were conducted to examine unadjusted associations between ANC utilisation and explanatory variables using Poisson regression models. Variables with a p-value < 0.25 at the bivariate level were considered for inclusion in the multivariable model.
Multivariable analysis was performed using Poisson regression with a log-link function to identify independent factors associated with the number of ANC visits. Model assumptions were assessed by comparing the mean and variance of the dependent variable. The mean (4.0016) and variance (4.0560) of ANC visits indicated approximate equidispersion, supporting the use of the standard Poisson model.
Adjusted Incidence Rate Ratios (AIRRs) with 95% Confidence Intervals (CIs) and corresponding p-values were reported. Statistical significance was set at p < 0.05.
Results
Number of women experiencing antenatal care visits
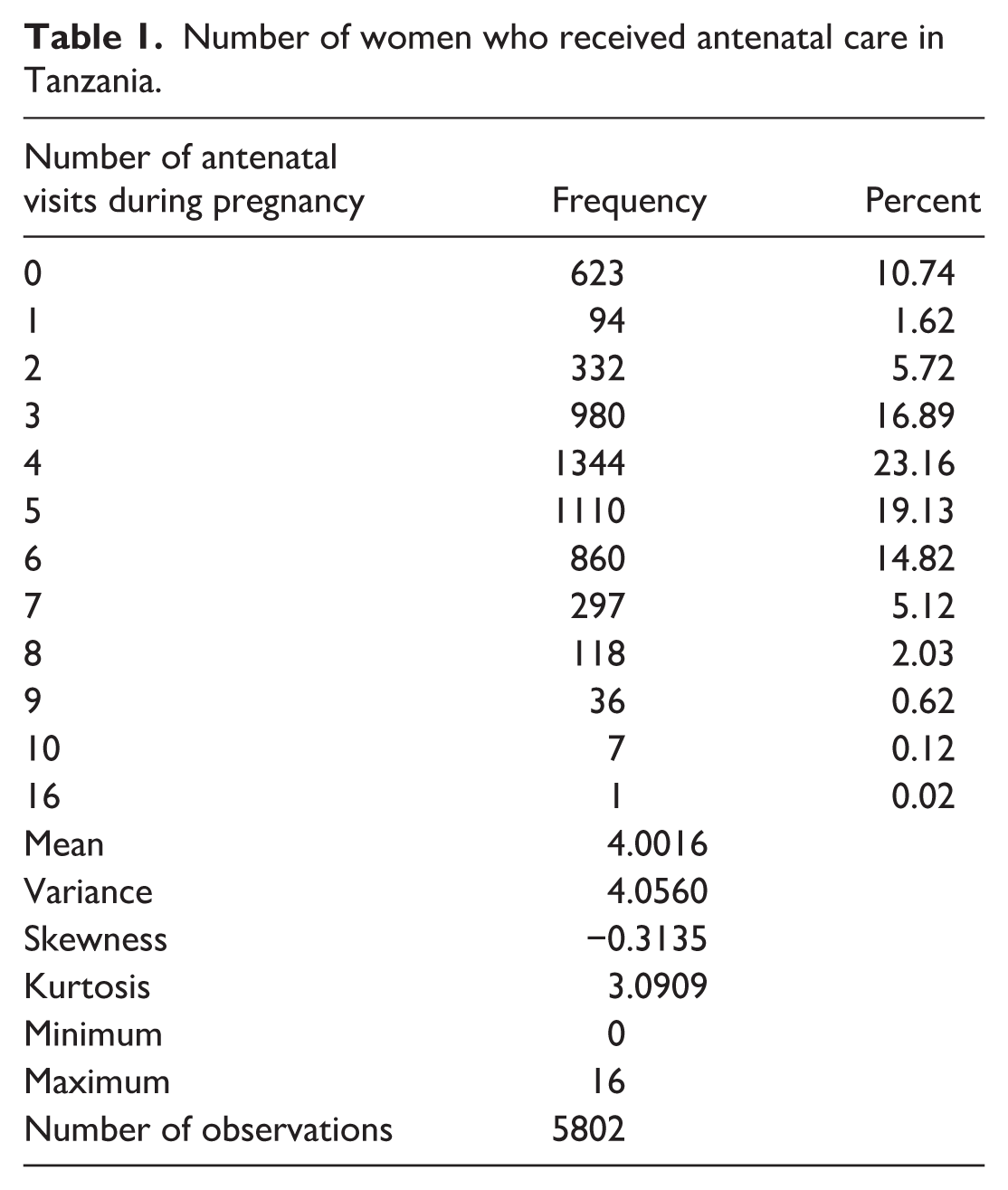
The distribution of antenatal care (ANC) visits during pregnancy reveals that 61.26% of women attended at least four ANC visits, meeting the minimum recommended level. Conversely, 38.74% of women had fewer than four visits. The mean number of ANC visits was approximately 4.0016, suggesting that, on average, women in the sample met the minimum recommended visits and a variance of 4.0560 (Table 1).
Number of women who received antenatal care in Tanzania.
Description of antenatal care utilisation among pregnant women
Table 2 presents variation in the mean number of ANC visits across different demographic, socioeconomic, and household characteristics. These differences highlight disparities in maternal healthcare access and utilisation. Maternal education shows a clear gradient; mothers with no formal education had the lowest mean ANC visits (mean = 3.44, SD = 1.99), while those with higher education reported the highest (mean = 5.90, SD = 1.96). Similarly, ANC utilisation increased with household wealth; the poorest households reported the lowest mean (mean = 3.38, SD = 2.02), whereas the richest households recorded the highest mean (mean = 4.83, SD = 2.06).
Number of antenatal care services utilisation by socio-demographic and economic characteristics of pregnant women in Tanzania.

Parity also influenced ANC visits; women with no children had the lowest average (mean = 3.14, SD = 2.59), compared to those with 1–2 children who reported the highest (mean = 4.33, SD = 2.02) suggesting increased care-seeking among experienced mother. Urban-rural differences were evident with rural dwellers recording the lowest mean (3.82, SD = 1.96), while urban residents had the highest (4.48, SD = 2.07). Smaller households (≤3 members) had higher utilisation (mean = 4.41, SD = 1.96) than larger ones (≥7 members; mean = 3.75, SD = 1.99).
Regarding occupational status, unemployed household heads were associated with lower maternal ANC utilisation (mean = 3.05, SD = 2.21), while professional heads had the highest (mean = 4.51, SD = 1.97). Similarly, among mothers themselves, non-working mothers reported fewer visits (mean = 3.64, SD = 2.18), while those in professional jobs had the highest, nearly five visits (mean = 4.99, SD = 2.11). Perceived access to healthcare also played a role; women who perceived the distance to health facilities as a major barrier reported fewer ANC visits (mean = 3.77, SD = 1.83), than those who did not see it as an issue (mean = 4.10, SD = 2.08). Regional differences were also notable, with the Western zone having the lowest average ANC utilisation (mean = 3.49, SD = 2.14) and the Eastern zone recording the highest (mean = 4.87, SD = 1.99).
Model evaluation
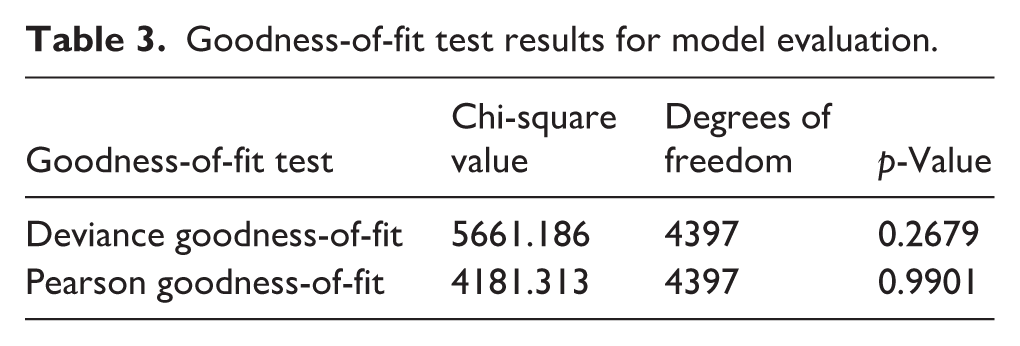
Table 3 shows that the Deviance Goodness-of-Fit and Pearson Goodness-of-Fit tests yield a p-value of 0.2679 and 0.9901, respectively. Both p-values are greater than the typical significance level of 0.05, suggesting that the model fits the data well and that there is no significant difference between the observed and expected values. This further supports the conclusion that the model fits the data well. Both tests indicate no evidence to reject the null hypothesis, asserting that the model adequately fits the data.
Goodness-of-fit test results for model evaluation.
Factors associated with the frequency of antenatal care visits
In the Poisson regression model, several variables were significantly associated with the frequency of antenatal care visits, including maternal education, household wealth index, size of household members, maternal and husband occupation, and geographical zone.
Maternal education was significantly related to the frequency of antenatal care (ANC) visits. Compared with women with no formal education, those who attained secondary education had approximately 10% more ANC visits (IRR = 1.10), while women with higher education recorded about 30% more visits (IRR = 1.30). Household wealth status also showed a strong positive gradient with ANC utilisation; women from poorer to richest households experienced between 10% and 25% higher ANC visit rates (IRRs ranging from 1.10 to 1.25) compared with those from the poorest households. In contrast, household size was inversely associated with ANC utilisation; women residing in larger households (seven or more members) had about 7% fewer ANC visits (IRR = 0.93) compared with those in smaller households.
Maternal occupation was significantly associated with antenatal care (ANC) utilisation. Compared with non-working mothers, women engaged in professional, sales/clerical, agricultural, and manual or other occupations recorded approximately 10%–17% higher ANC visit rates (IRRs ranging from 1.10 to 1.17). Similarly, the husband’s occupation emerged as an important determinant of ANC utilisation; women whose partners were engaged in professional, sales/clerical, agricultural, or manual occupations experienced about 10%–14% more ANC visits compared with those whose partners were not working (IRRs ranging from 1.10 to 1.14).
Geographical variation in ANC utilisation was also evident. Relative to women residing in the Western zone, those living in the Central, Southern, Eastern, and Zanzibar zones had significantly higher ANC visit rates, ranging from approximately 14% to 28% increases (IRRs between 1.14 and 1.28; Table 4).
Factors associated with ANC service utilisation among pregnant women in Tanzania.

Discussion
Our study found that a significant majority of women approximately 89.26% attended at least one antenatal care (ANC) visit. This aligns with findings from similar studies conducted in Southwestern Ethiopia (91.9%), 16 Ghana (98.3%), 17 Pakistan (83.5%), 18 Guinea (80.3%), 19 and Somalia (80%). 20
However, only 61.26% of women completed the recommended minimum of four ANC visits. While this rate is higher than those reported in Rwanda (54%), 21 sub-Saharan Africa (58.53%), 5 India (51.7%), 22 Nigeria (56.2%), 23 and Pakistan (57.3%), 18 it still indicates room for improvement.
The average number of ANC visits was 4.00, with a variance of 4.06, indicating considerable disparities in ANC attendance among pregnant women. 24 These findings highlight the need for targeted interventions aimed at increasing ANC utilisation, especially for women who face barriers such as limited access to healthcare facilities, financial difficulties, or lack of awareness about the importance of regular prenatal care.
The Deviance and Pearson Goodness-of-Fit tests confirm that the model provides an adequate fit to the data, as indicated by p-values of 0.2679 and 0.9901, both exceeding the 0.05 significance threshold. This suggests no significant difference between observed and expected values, reinforcing the model’s reliability in explaining the data. This study reported similar findings in Nairobi, Kenya. 25 The results provide strong evidence against rejecting the null hypothesis, further validating the model’s appropriateness for analysis. 26
The findings of this study reveal key socioeconomic and demographic factors influencing the frequency of antenatal care (ANC) visits in Tanzania. Maternal education emerged as a strong determinant of the frequency of ANC visits. In the Tanzanian context, higher educational attainment is likely to enhance women’s health literacy, awareness of pregnancy-related risks, and autonomy in healthcare decision-making, thereby promoting repeated ANC attendance. Similar associations between maternal education and ANC utilisation have been reported in previous studies in Tanzania and other sub-Saharan African settings.5,27
Household wealth was also positively associated with ANC utilisation, highlighting the persistent role of economic barriers in accessing maternal health services. In Tanzania, although ANC services are officially provided free of charge, indirect costs such as transportation, opportunity costs related to time away from income-generating activities, and informal expenses can limit sustained attendance among women from poorer households. This finding is consistent with evidence from Tanzania and other low-and middle-income countries, where wealthier households are better positioned to overcome financial and geographic barriers to care.23,28
The inverse association between household size and ANC visits suggests that women in larger households may experience competing domestic responsibilities and resource constraints that reduce their ability to attend repeated ANC visits. In Tanzania, extended family structures are common, and larger households may dilute both financial and social support for maternal healthcare, particularly in rural areas. Similar findings have been documented in studies from Nigeria and other sub-Saharan African countries. 23
Occupational status of both women and their partners was significantly associated with ANC utilisation. Employment may improve household income, social empowerment, and exposure to health information, all of which facilitate greater use of maternal health services. In the Tanzanian context, the influence of a husband’s occupation is particularly important, as men often play a central role in household decision-making regarding healthcare seeking. Previous studies have similarly highlighted the role of male socioeconomic status and involvement in improving maternal health service utilisation.28,29
Geographical disparities in ANC utilisation further reflect structural inequalities within Tanzania’s health system. Higher ANC visit frequencies in the Central, Southern, Eastern, and Zanzibar zones compared with the Western zone likely indicate differences in health infrastructure, urbanisation, availability of skilled health personnel, and regional development. National survey reports and previous studies have consistently shown that women residing in more urbanised and economically developed regions of Tanzania have better access to maternal health services than those in less developed regions. 8
This study contributes new national-level evidence from the 2022 TDHS by focussing on the frequency of antenatal care visits rather than mere ANC attendance. Using Poisson regression and reporting Incidence Rate Ratios, the analysis quantifies the socioeconomic and demographic factors associated with sustained ANC utilisation, providing deeper insights into maternal health-seeking behaviour in Tanzania. The results reveal that, despite widespread initial contact with ANC services, marked inequalities remain in the continuation of care, underscoring key areas for targeted policy and programmatic interventions. While recent literature highlights the importance of incorporating timeliness and quality dimensions into ANC measurement13,14 respectively, future studies using TDHS data should extend beyond visit frequency to align with these evolving analytical frameworks.
Strengths and limitations
A major strength of this study lies in its use of the 2022 Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS), a nationally representative dataset that boosts the findings’ applicability to the wider Tanzanian population. The extensive sample size and meticulous sampling approach enhance both the statistical power and the reliability of the estimates. Furthermore, the study offers significant insights into regional disparities along with the socioeconomic and demographic factors influencing ANC utilisation, which can guide targeted public health interventions and policy development.
Nonetheless, this study has some limitations. First, ANC utilisation was measured solely based on the number of visits, without incorporating information on the timing of initiation or the quality and content of care. Recent evidence suggests that these dimensions provide a more comprehensive assessment of ANC adequacy. 13 However, given the study objective and the analytical focus on visit frequency, the findings should be interpreted as reflecting patterns of ANC contact rather than overall quality-adjusted ANC utilisation.
Conclusion and recommendation
In summary, this study reveals that, although most women in Tanzania participate in at least one antenatal care (ANC) visit, a notable number do not complete the advised minimum of four visits. Socioeconomic and demographic factors- such as maternal education, household wealth, occupation, household size, and geographical location- significantly influence ANC attendance. These results emphasise the necessity for fair and focussed health interventions that tackle both demand- and supply-side obstacles to ANC utilisation.
To enhance ANC coverage and ensure continuity, it is advisable that health policies prioritise awareness campaigns, particularly in underserved areas, and promote women’s education and economic empowerment. Strengthening healthcare infrastructure in remote locations and integrating culturally sensitive approaches can also help bridge regional disparities. Furthermore, encouraging male involvement and supportive roles for partners could further improve maternal healthcare-seeking behaviour. Collaborative efforts among the government, community leaders, and development partners are crucial for enhancing maternal health outcomes in Tanzania.
Supplemental Material
sj-pdf-1-phj-10.1177_22799036261441323 – Supplemental material for Antenatal care utilisation in Tanzania: A Poisson regression analysis of the Tanzania Demographic Health Survey 2022
Supplemental material, sj-pdf-1-phj-10.1177_22799036261441323 for Antenatal care utilisation in Tanzania: A Poisson regression analysis of the Tanzania Demographic Health Survey 2022 by Edgar Elirehema Pallangyo, Dyness Kejo, Monica Chipungahelo, Zahara Daudi, Nsajigwa Reuben Mwalupani, Doris Katana and Amina Suleiman Msengwa in Journal of Public Health Research
Footnotes
Acknowledgements
The authors acknowledge the DHS program portal for providing data for the analysis.
Ethical considerations
This study was conducted using secondary data from the Tanzania Demographic and Health Survey (TDHS) 2022. The data collection for TDHS 2022 was carried out in compliance with all applicable ethical standards and protocols. The survey protocols were approved by the National Institute for Medical Research (NIMR) Ethics Committee in Tanzania and adhered to international ethical standards such as the Declaration of Helsinki. Since this study is based on publicly available and anonymised secondary data, no additional ethical approval was required for the analysis presented here.
Consent to Participate
Informed consent was obtained from all participants, and confidentiality was maintained.
Consent for publication
Not applicable.
Author contributions
EEP and DK conceived the idea and drafted the manuscript. EPP, ASM, and NRM operationalised the models and participated in data analysis. ASM, DK, ZAD and MC Critically revised and edited the manuscript. All authors reviewed the first draft of the manuscript and approved the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Clinical trial
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.