
Abstract
Background:
Social determinants of health (SDOH), the conditions in which people live, work, play, and learn, are largely responsible for health inequities seen among individuals with disabilities. However, less is known about relationships between SDOH and poor housing for disabled adults. Using state-level SDOH proxy variables for economic stability, education, healthcare access, and the social and community context, this secondary data analysis examined the interrelated effects of SDOH proxy variables on poor housing for disabled adults in the United States.
Design and methods:
We used quantitative comparison and regression analysis of national, state-level estimates from the 2023 Annual Disability Statistics Compendium and 2021 American Community Survey data to investigate poor housing outcomes for disabled adults. We intentionally examine state-level estimates of prevalence rates, rather than individual-level data, to better understand the systemic nature of SDOH relationships for disabled adults.
Results:
Compared to non-disabled adults, a higher percentage of disabled adults reside in poor housing, have lower state-level employment rates, have higher rates of high school-only education, lower rates of 4-year college degrees, and have lower voter turnout. SDOH proxy variables of employment and education were consistently strong predictors of state-level poor housing for both disabled and non-disabled adults. When all four SDOH proxy variables were included in the regression analysis, they accounted for 62.6% and 62.7% of the variability in state-level poor housing for disabled and non-disabled adults, respectively.
Conclusions:
Findings suggest that including SDOH domains provides a robust model for understanding housing challenges for both disabled and non-disabled adults.
Keywords
Introduction
Over 70 million U.S. adults report having a disability, 1 yet people with disabilities remain an understudied population. 2 Disability is defined as “any condition of the body or mind that makes it more difficult for the person with the condition to do certain activities and interact with the world around them.” 3 The National Institutes of Health (NIH) recently designated people with disabilities as a population with health disparities. 4 They are also protected legally in the United States by the Fair Housing Act, Section 504 of the Rehabilitation Act, and the Americans with Disabilities Act to ensure equal access to housing. These important designations are a critical first step to deepening our understanding of the impact that disparities, including housing disparities, have on people with disabilities.
Existing disparities for people with disabilities are rooted in the same upstream social and economic conditions that were first introduced by Sir Michael Marmot and the World Health Organization (WHO) Commission on Social Determinants of Health. 5 The subsequent and pivotal WHO 2008 report entitled “Closing the Gap in a Generation” 6 serves as the basis for public discourse supporting the idea that health disparities are socially produced and therefore must be eliminated though policy change and social justice. This groundbreaking approach led to informing Healthy People 2020 7 which transitioned from focusing on individual factors to emphasizing social determinants as influencing health. Thus, using a Social Determinants of Health (SDOH) lens is ideal for exploring predictors of poor housing for disabled adults.
SDOH and disability
Previous work has compared disabled and non-disabled individuals across the myriad conditions in which people live, learn, work, and play that affect health. Cumulatively, these SDOH are largely responsible for health inequities seen among individuals, findings that are consistent with Sir Michael Marmots original ideas. 5 When compared to non-disabled people, individuals with disabilities have poorer health, 8 experience greater rates of poverty, 9 and experience higher rates of material hardship, even when working full time. 10 However, there is a paucity of studies focused on housing as a social determinant of health for people with disabilities.
Social determinants of health are grouped into five domains: the neighborhood and built environment, economic stability, education access and quality, healthcare access and quality, and the social and community context 11 as seen in Figure 1, adapted from the Office of Disease Prevention and Health Promotion. 12 These domains are critical to developing a comprehensive understanding of individuals’ health and well-being, as well as the interrelationship among domains, where the impact of one domain reverberates into consequences elsewhere. In this analysis, we build from the premise that home, housing, and community are tenants of an inclusive society.

Social determinants of health.
Urban scholarship has explored the relationships between housing access and social inequality, demonstrating the importance of housing policy, planning, and community engagement in creating mechanisms that promote housing equity or exacerbate existing housing inequalities. Social factors associated with historic oppression and inequality such as race, education, and socioeconomic status predict the likelihood of access to safe and dignified housing for individuals, groups, and geographic communities. 13 Therefore, we posit that using a SDOH lens is critical to understanding housing disparities that are known to exist for disabled adults.
Housing and disability
The recent shift from institutional care to community-based support for adults with disabilities has been especially important for ensuring greater safety, self-determination, and life satisfaction. 14 In fact, home care recommendations are created under the assumption that living conditions for disabled adults are ideal when planning for home discharge after hospitalization or rehabilitation. 15 However, research has demonstrated that housing for disabled adults is inadequate, which has important consequences for both disabled adults and the communities in which they live. We believe it is important to consider both the cost and condition of housing for adults within the SDOH framework. Therefore, we intentionally selected state-level poor housing (as defined by the Annual Disability Statistics Compendium (ADSC)) as the proxy dependent variable for this study because housing takes on multiple aspects of both economic (affordability) and social (livability) dimensions.
Economically, housing costs remain a central feature of the ongoing housing crisis, a situation rooted in the affordability crisis from the Great Recession of 2008 and further intensified by the COVID-19 pandemic. 16 Affordable housing research almost uniformly defines a household as being “cost burdened" if 30% or more of gross household income is being spent on rent or mortgage, plus utilities. A household exceeding 50% of gross income is considered “severely cost-burdened.” 17 While both rental and homeownership can create cost burdens and housing insecurity for individuals, renting can be further compounded by market failures and a lack of adequate rental insurance. Dundon and Camp 18 highlight the vulnerability of renters, particularly low-income minority renters, in the context of managed retreat programs designed to relocate people from disaster-prone areas.
Socially, housing cost burdens and housing insecurity interrelate to additional problems around liability. For instance, housing insecurity can restrict social networks and generate barriers to education and employment. 19 In addition, those without secure housing report significantly poorer well-being. 20 While worse physical health is generally associated with poverty, it is more pronounced in populations without secure housing. 21
Beyond affordability, housing quality and accessibility are also critical issues for disabled individuals. The built environment has profound impacts on daily life affecting health and safety outcomes for people with disabilities. 16 For disabled individuals with mobility impairments, access and usability are key factors to independent living and community participation. 22 However, research indicates that most housing units are not designed to meet the needs of people with disabilities, including physical home design which fails to accommodate the need to access and move within the home space. 23 Housing is a key element that can either promote or hinder the long-term well-being of disabled adults from living in their communities. 15 The paucity of affordable, accessible, and livable housing perpetuates the exclusion and marginalization of people with disabilities.
Existing research has established that people with disabilities are more susceptible to community displacement, housing insecurity, poor housing conditions, and higher housing-cost burdens. 15 Sellers et al. 24 found that in addition to having a higher housing cost burden, disabled adults were also more likely to live in older housing and have incomplete kitchens and plumbing when compared to their non-disabled counterparts. Moreover, older, and lower quality housing for people with disabilities was, in fact, not affordable when using regression analyses to predict housing cost burden for disabled adults. When housing type was examined between high- and low-poverty states, more adults with disabilities lived in mobile homes in high-poverty states, 25 suggesting that people with disabilities may seek lower-cost housing such as mobile homes out of necessity. Importantly, inaccessible housing and low-quality housing for people with disabilities likely perpetuates their health and safety disparities. 16 In this context, people with disabilities who reside in poor housing may be at even higher risk for poor health than previously described. We build on the concept that a lack of affordability, access, and livability for people with disabilities equates to a general issue of poor housing which must be considered in the context of SDOH to fully grasp factors which hinder health and well-being. Therefore, we set out to explore relationships between poor housing and SDOH for disabled adults.
Purpose
While prior research has demonstrated greater housing insecurity, poor housing conditions, and higher housing-cost burden for people with disabilities, no studies have explored the relationships between state-level SDOH proxy variables and poor housing for disabled adults. Doing so is important to better understand the interrelationships of SDOH factors on housing challenges that are known to exist for this already disadvantaged population. While using a SDOH lens to examine these factors provides a theoretical strength in this case, it does present an analytical challenge, because no standard variables or measures exist for the five domains of social determinants. Therefore, our analysis used available state-level proxy variables that represent the five social determinants domains described in the literature – economic stability, education, healthcare access, and social and community context – to explore their cumulative impacts on the built environment for both disabled and non-disabled adults. Using state-level proxy variables for each of the five SDOH domains, we identified two specific research questions (1): do social determinants proxy variables differ for disabled and non-disabled adults? and (2) what social determinants proxy variables are predictive of poor housing for both disabled and non-disabled adults?
Method
Design
This study employed an analysis of cross-sectional state-level data for all 50 U.S. states and the District of Columbia for an N = 51. We intentionally used aggregated state-level data, rather than individual data, to better understand the systemic nature of SDOH relationships for people with disabilities. Data for this study came from tables 1.3, 3.1, 3.2, 7.5, 9.1, 13.5-13.8, and 16.3 of the 2023 ADSC, which compiles information about disabled populations from various data sources. 26 The ADSC data used in this study is based on annual, state-level estimates, sourced primarily from the 2021 American Community Survey (ACS) which is a nationally representative, monthly survey from the U.S. Census Bureau.
Unless otherwise noted, all metrics in this study come from the ACS, are analyzed, and reported as rates, and are calculated separately for disabled (percentage of the population with a disability) and non-disabled (percentage of the population without a disability) adults. We maintained each measure as a percentage of the population, rather than the population count, to adjust for relative variability in group and state population sizes.
We intentionally included only adults aged 18–64 years for this study, as it is this age group which retains the fewest social protections, especially regarding health insurance coverage, education, and housing, when compared to those under age 18 or adults aged 65 and older.
For this study, disability is defined as reporting one or more of six disability metrics: hearing difficulty, vision difficulty, cognitive difficulty, ambulatory difficulty, self-care difficulty, and independent living difficulty. It is important to recognize that the five traditional SDOH domains 11 are complex and multifaceted. Moreover, there is no standard measure or variable for each of the five domains. Therefore, we selected variables that serve as proxies for each SDOH domain. We used these specific proxy variables because they were determined to be the closest measure based on available ACS measures and ADSC data. These SDOH domains are reported in Figure 1:
Neighborhood and Built Environment is operationalized by the proxy variable of poor housing which is defined by the ADSC 25 as the percentage of adults living in a home with two or more housing difficulties. Housing difficulties include residing in a home lacking a complete kitchen, lacking complete plumbing, being overcrowded (two or more residents per bedroom), and having housing cost burden (over 35% of household income spent on housing costs).
Economic Stability is operationalized by the proxy variable of state employment rate. This rate is calculated as the proportion of adults ages 18–64 who reported having worked during the prior week.
Education Access and Quality is operationalized by the proxy variable of educational attainment of a 4-year college degree. This proxy variable was developed by the research team by dichotomizing educational attainment as the percentage of adults ages 25 and older that have at least a bachelor’s (4-year) degree or a higher-level of education versus those who have less than a 4-year degree. We also reported the percentage of adults whose highest level of educational attainment is a high school diploma or equivalent (e.g. GED) in Table 1,but did not include this in our multivariable analyses.
Healthcare Access and Quality is operationalized by the proxy variable of health insurance coverage, which is reported in the ADSC as the percentage of community-dwelling adults ages 18–64 with health insurance coverage. This measure included any form of health insurance coverage, regardless of type.
Social and Community Context is operationalized by the proxy variable of voter turnout which is defined by the ADSC as the percentage of eligible voters that voted in the 2020 presidential election. Voter turnout data was sourced from the Current Population Survey’s November 2020 Voting and Registration Survey, with state-level estimates calculated by Schur and Kruse. 27
Descriptive statistics: State-level SDOH proxy variables by disability status, adults 18–64.

Sources: 2023 Annual Disability Statistics Compendium (2021 American Community Survey, Public Use Microdata Set; November 2020 Current Population Survey, Voting and Registration Supplement).
p < 0.001.
Data analysis
To determine state-level SDOH contexts for disabled and non-disabled adults and identify the interrelationship between SDOH and poor housing, we used secondary, state-level proxy variables for all 50 U.S. States and the District of Columbia (N = 51) in a three-phase approach. In phase I (Descriptives and Difference Testing), we conducted descriptives statistics for each SDOH proxy measure by disability status and then conducted paired sample t-tests to test for differences between disabled and non-disabled adults to answer the first research question.
In phase II (Individual Modeling), a series of ordinary least squared (OLS) regression analyses were conducted to predict poor housing for disabled (Model A) and non-disabled (Model B) adults, using the four remaining SDOH proxy measures. Each model included the SDOH rates for both disabled and non-disabled adults, to understand the broader context of state-level SDOH and their interrelationship with poor housing in the disability context.
Phase III (Combined Modeling) included all four predictor SDOHs into one model, predicting poor housing rates separately for disabled (Model A) and non-disabled adults (Model B), to understand the cumulative state-level impacts of the four SDOH, and to uncover any distinct differences in SDOH’s influence between these two groups. All analyses were conducted using the Statistical Package for the Social Sciences (IBM SPSS). Due to the small sample size of this study, all analyses reported statistical significance at the traditional p-value cutoffs (0.001, 0.01, 0.05) as well as measures trending at p ≤ 0.1.
Results
Phase I
Table 1 presents descriptive statistics and paired sample t-tests for each of the SDOH proxy variables at the state-level by disability status (N = 51).
On average, 11.4% (SD = 2.30) of each state’s adult population has a disability. This finding, which differs from the national average of approximately 25%, can be explained by our decision to only include adults aged 18–64 years. Significant differences between disabled and non-disabled adults were evident across all state-level SDOH domains. For every SDOH proxy measure, rates significantly differed between disabled and non-disabled populations (p < 0.001). In terms of the Housing and the Built Environment (poor housing), states on average had a higher proportion of disabled adults living in poor housing (13.94%, SD = 3.04), compared to non-disabled adults (6.97%, SD = 2.01). Economic Stability (employment) differences were substantial, as disabled adults had lower average state-level employment rates (38.18%, SD = 5.39) compared to non-disabled adults (76.09%, SD = 3.30), illustrating a 37.91% gap in the average employment rate.
Educational Access and Quality (educational attainment) also differed between disabled and non-disabled adults. More disabled adults (64.01%, SD = 4.39) have a high school-level education as their highest degree when compared to non-disabled adults (54.87%, SD = 6.68). More non-disabled adults completed a 4-year college degree (37.59%, SD = 7.02), whereas only one in five disabled adults completed a college education (19.25%, SD = 4.04). Using health insurance coverage as a proxy for Healthcare Access and Quality, disabled adults had about a 1% advantage in the average health insurance coverage rate (89.30%, SD = 5.01), compared to non-disabled adults (88.03%, SD = 4.61). Finally, in using voter turnout as a proxy for Social and Community Context, states had higher voter turnout rates for non-disabled voters (67.76%, SD = 5.69), compared to disabled voters (62.62%, SD = 6.35).
Phase II
Table 2 displays four models using OLS regression analyses, one for each SDOH domain. We predict state-level poor housing rates for both disabled (Subset A) and non-disabled (Subset B) adults.
Predicting state-level poor housing rates for disabled and non-disabled adults.
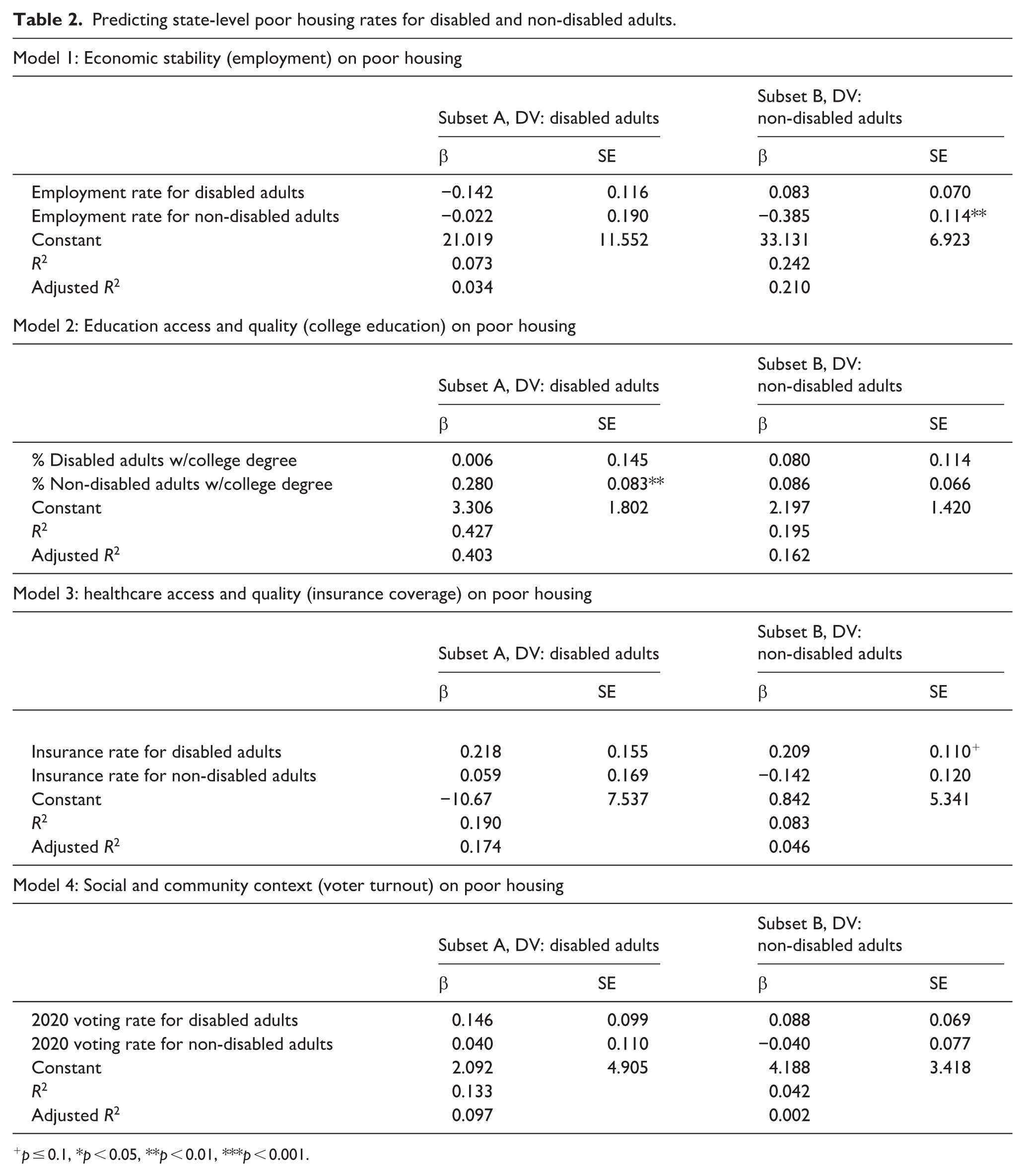
p ≤ 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
Model 1 examined the predictive ability of Economic Stability (employment) on the Neighborhood and Built Environment (poor housing). Employment rates provided little explanation for state-level variation in disabled adult poor housing rates (Model 1A, R2 = 0.073). When controlling for the employment rates for non-disabled adults, employment rates for disabled adults did not significantly predict poor housing for rates disabled adults (p = 0.228). In Model 1B, employment for non-disabled adults had a negative relationship (β = −0.385, p < 0.01) with poor housing for non-disabled adults, with employment explaining 24% of the state-level variability in poor housing rates (R2 = 0.242). Thus, as employment for non-disabled adults increases, state-level poor housing decreases for non-disabled adults.
Model 2 examined the predictive ability of Educational Access and Quality (college education) on the Neighborhood and Built Environment (poor housing). Model 2A found that state-level college education explains roughly 43% of the variability in state-level poor housing rates for disabled adults (R2 = 0.427). Thus, as state-level rates of non-disabled college education increases, so does the state-level rates of poor housing for disabled adults (β = 0.280, p < 0.01). For non-disabled adults as reflected in Model 2B, education’s explanatory power for poor housing (R2 = 0.195, R2adj = 0.162) was half of the explanatory power for non-disabled adults (R2adj = 0.403, difference of 0.265). Model 2B, on the other hand, examined disabled and non-disabled state-level college education and its ability to predict state-level poor housing for non-disabled adults, and neither disabled nor non-disabled college education rates were found to significantly predict poor housing rates for non-disabled adults.
Model 3 of the regression analyses examined the predictive ability of Healthcare Access and Quality (insurance coverage) on the Neighborhood and Built Environment (poor housing). While Model 3A did not find state-level health insurance coverage for either disabled or non-disabled adults to be statistically significant predictors of poor housing for disabled adults, the full model explained 19% of the variability in state-level disabled adult poor housing (R2 = 0.190). Conversely, while Model 3B did find state-level health insurance coverage for disabled adults to have a trending effect (p ≤ 0.1), the model explained even less of the variability in state-level poor housing for non-disabled adults (R2 = 0.083). When comparing these models, Model 3B had one-third of the explanatory power (R2adj = 0.046) relative to Model 3A (R2adj = 0.174) with a difference of 0.128.
Finally, Model 4 sought to understand the impact of the Social and Community Context (voter turnout) on the Neighborhood and Built Environment (poor housing). Using state-level voter turnout rates for the 2020 election for both disabled and non-disabled adults, we found neither to be significant predictors of state-level poor housing rates for the two adult populations. Thus, voting rates provided little explanation for variability in state-level poor housing rates, with R2 and adjusted-R2s of 0.133 and 0.097 (Model 4A); and 0.042 and 0.002 (Model 4B) for disabled and non-disabled adults, respectively.
Phase III
Table 3 presents two multivariate OLS regression models, combining all four SDOH proxy variables to predict the Neighborhood and Built Environment (poor housing) for disabled adults (Model A) and non-disabled adults (Model B) to understand the interrelationship between the four SDOH domains and their combined ability to predict poor housing.
Combined SDOH models predicting state-level poor housing rates.

p ≤ 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
In examining the results in Model A for predicting state-level poor housing rates for disabled adults, two of the four SDOH proxy predictors are significant at the p < 0.05 level. There is a negative relationship between employment rate for non-disabled adults and poor housing for disabled adults (β = −0.342, p = 0.042). Thus, as state-level employment rates increase for non-disabled adults, state-level poor housing rates decrease for disabled adults. In addition, there is a positive relationship between a college degree for non-disabled adults and poor housing for disabled adults (β = 0.225, p = 0.020).
Taken together, all four SDOH proxy variables account for approximately 63% of the variability in poor housing for disabled adults (R2 = 0.626). Notably, none of the state-level SDOH rates for disabled adults significantly predicted poor housing rates for disabled adults. Instead, SDOH proxy variables for non-disabled adults directly impacted the housing conditions of disabled adults.
When examining Model B, which predicted state-level poor housing rates for non-disabled adults using all four SDOH domains, we found the model is similarly robust, explaining nearly 63% of the variability in state-level poor housing for non-disabled adults (R2 = 0.627). Employment rates for both disabled (β = 0.121, p = 0.034) and non-disabled adults (β = −0.559, p < 0.001), and the percent of non-disabled adults with a college degree (β = 0.127, p = 0.046) were significant predictors of state-level poor housing rates for non-disabled adults. Thus, as state-level employment rates of disabled adults increase, so too does state-level rates of poor housing for non-disabled adults. In addition, as state-level employment rates of non-disabled adults decrease, state-level poor housing rates increase for non-disabled adults, and as the state-level rates of college educated non-disabled adults increases, state-level rates of poor housing for non-disabled adults increases. Finally, voter turnout for disabled adults was also trending toward significance as a predictor (β = 0.081, p = 0.092); thus, as state-level voter participation rates increase for disabled adults, so does the percentage of non-disabled adults in poor housing.
Discussion
For optimal well-being and inclusion, it is critical for people with disabilities to live fully within their communities and maintain adequate housing. 28 Further, persons with disability are protected under various laws to prevent discrimination and provide opportunities to remain in their communities through the Fair Housing Act, Section 504 of the Rehabilitation Act, and the Americans with Disabilities Act. In requiring “Affirmatively Furthering Fair Housing,” safe, accessible, and affordable housing has been defined as a fundamental human right and a critical determinant of long-term well-being for individuals who wish to remain at home and in their community. 29 Housing accessibility and affordability are key aspects of remaining housed within communities.
Therefore, we applied an SDOH framework to understand the interrelationships between five state-level SDOH proxy variables for disabled and non-disabled adults and poor housing outcomes. Not surprisingly, we found that all five state-level proxy variables differed significantly between disabled and non-disabled adults. We found disabled adults to be worse-off for the majority of SDOH proxy variables, which is consistent with prior research focused on disability-related disparities. This further amplifies that adults with disabilities, in many respects, continue to be left behind. This study also demonstrated that using a SDOH lens provides a robust model to understand and predict poor housing in the disability context (Figure 2).

(a) Predicting poor housing rates for disabled adults. (b) Predicting poor housing rates for non-disabled adults.
Our analyses found that Economic Stability (employment) varied greatly when we accounted for disability status, with disabled adults at a greater disadvantage. Disabled adults not only had far-lower state-wide employment rates than non-disabled adults, but employment rates were far more variable for disabled adults. This is consistent with prior research demonstrating that employment rates of disabled adults are far more sensitive to economic changes, as seen with greater declines in employment for disabled adults after the Great Recession. 30
Employment rates for non-disabled adults partially explain the housing quality of disabled adults, and vice-versa. Notably, only non-disabled adult state-level employment seems to protect against poor housing in phase II of our analysis. While we found that employment rates significantly influence housing quality for both disabled and non-disabled adults, the context of its effects differ by disability status, and only when employment rate was included with the other three SDOH proxy variables in the full, phase III model. This suggests that the broader context of state-level economic stability influences poor housing, not just the economic stability of the population under examination.
Our combined SDOH model demonstrates the interrelated context of employment. As state-level employment rates increase for both disabled adults and non-disabled adults, state-level poor housing rates decrease for disabled adults. However, the same is not true for non-disabled poor housing rates, where increasing employment rates for disabled adults increases poor housing rates for non-disabled adults. We interpret this as an indication that higher state-level employment rates may either provide more resources for housing support or reduce the demands on existing housing resources for disabled persons.
Considering that a larger proportion of non-disabled adults exist in the overall workforce, it is possible that non-disabled state-level employment rates may be indicative of the overall state-level economic outlook, which may have the potential for a positive spillover effect for disabled adults. However, this was not evident when looking at employment rates for disabled adults just prior to the Great Recession. 30 Generally, the inclusion of employment rate as a single proxy variable for Economic Stability in our analyses fails to capture the nuances of this SDOH domain. Thus, further exploration is needed to better understand this SDOH domain’s effects on housing quality in the context of disability.
We also found disparities in Educational Attainment and Quality (college degree attainment), given the lower, state-level educational attainment rates among disabled adults. While we would expect that higher state-level college education rates for disabled adults would be associated with better quality housing (by way of improved socioeconomic resources that protect against poor housing), this was not evident in our analyses. In fact, we found the inverse to be evident: when first examining state-level college education rates alone to predict poor housing in phase II of our analyses, state-level rates for non-disabled adults were significant predictors of an increase in poor housing for disabled adults. Subsequently, when all four SDOH proxy variables were included in the phase III regression model, higher state-level college education rates for non-disabled adults predicted poor housing for both disabled and non-disabled adults.
While a “resource-scarcity” mindset might explain why higher state-level college education rates of non-disabled adults limit opportunities for disabled adults, the positive relationship between state-level college education and poor housing for non-disabled adults was surprising. It is certainly possible that higher educational attainment rates of non-disabled adults disproportionately benefit non-disabled adults and therefore leads to greater inequalities in income and employment opportunities for disabled adults, thus leaving behind persons who can no longer afford or maintain adequate housing and exacerbating existing inequalities. It is also possible that states which experience an influx of educated workers may choose to prioritize economic development and middle-class housing initiatives over social services such as disability benefits, accessible housing programs, and rental assistance. Thus, such policy shifts can further disadvantage disabled individuals, reinforcing the cycle of poor housing conditions and economic insecurity.
This counterintuitive finding may also be an indication of the educational disparities that emerge in educational attainment between disabled and non-disabled persons. That disabled adults had much lower rates of educational attainment with college degrees than non-disabled adults may be due to the lack of legal and institutional supports in higher education compared to primary education. Thus, we speculate that where non-disabled educational attainment is higher, disabled adults may be left behind in finding or maintaining adequate housing because of the limited employment opportunities that result from lower educational attainment to begin with. In this case, disabled adults may be getting priced out of the market through cost-burdens or forced into sub-standard housing.
The lack of significance when predicting poor housing with state-level college education rates for disabled adults suggests that educational attainment alone does not lead to universally improved housing outcomes, even when controlling for the influences of other SDOH proxy variables. These findings are counterintuitive to the common assumption that higher levels of educational attainment universally translate to improved living conditions. Despite higher levels of educational attainment, disabled adults with a college degree may continue to face systemic barriers such as employment discrimination, lower or fixed incomes, and a lack of affordable, accessible housing. Collectively, these findings emphasize the presence of complex dynamics underlying the relationships between state-level disability, educational attainment, resource allocation, and housing conditions.
Our findings provided little insight into the effects of healthcare access and quality on housing. Disabled adults had a small, but significant advantage in health insurance coverage rates when compared to non-disabled adults. This higher rate of health insurance coverage for disabled adults, however, may be explained by the disability population’s reliance on public health insurance, rather than a true advantage of healthcare quality and access. For disabled, working-age adults, the state-level average for public health insurance utilization was 53.73% (SD = 7.65). While our primary data source did not publish comparable state estimates for non-disabled adults, estimates for public insurance coverage for all adults (ages 19–64) was 18.7%. 31
While state-level insurance coverage rates were nonsignificant in their relationship to housing quality for disabled adults, one interesting finding emerged in phase II of our analyses: higher insurance coverage rates for disabled adults predicted higher rates of poor housing among their non-disabled counterparts. While we found only trending significance for this relationship, it suggests that additional complexities remain unexplored. The limited explanatory power of these models underscores the critical need for future studies aimed at understanding the nuanced interactions between healthcare quality, housing quality, and disability within the SDOH framework. Such research should focus on integrating these domains to better understand state-level policy tensions, resource allocations, and their implications for achieving equitable health and housing outcomes.
We encountered inherent challenges measuring Social and Community Context, as this SDOH domain focuses on “the characteristics of environments where people live, learn, work, and play.” 11 Average voter turnout rate for disabled adults was lower than non-disabled turnout rates by 5.14%. While statistically significant, the gap between disabled and non-disabled voter turnout has narrowed in the last decade, thanks in large part to improved accessibility through mail-in ballots and early voting which are heavily utilized by disabled voters. 27 It is worth noting that Belt 32 referred to adults with disabilities as “the canaries in the coal mine,” since they often identify structural inadequacies in voting that affect the entire system. However, recent, structural changes are encouraging for increasing the civic participation of disabled adults.
On the other hand, this may indicate that voter turnout may no longer be a useful proxy variable for civic participation. Voter turnout rates were nonsignificant in our multivariable analyses, although voter turnout for disabled adults was trending toward significance as a predictor (β = 0.081, p = 0.092) demonstrating that as state-level voter participation rates increase for disabled adults, so too does the percentage of non-disabled adults in poor housing. We find this outcome to be somewhat counterintuitive and suggest future study to understand the impact of voter participation on housing. Future SDOH research should explore other ways that the social and community context can be adequately captured at the state-level, particularly in the context of disability, as some established measures such as incarceration rates, disability-related hate crimes or discrimination rates may not be widely accessible or reliable.
While we presumed that our proxy variables would demonstrate some degree of impact, we did not consistently find these relationships when looking at predictors of poor housing. In both separate and combined analyses of the four SDOH proxy variables predicting poor housing rates, only employment and college education rates had a significant influence on state-level poor housing rates. In comparing outcomes between disabled and non-disabled adults, state-level outcomes for disabled adults had little bearing on poor housing for disabled adults. In the cases of employment and education, the context of non-disabled adults’ experiences has a significant influence on housing quality for disabled adults. One possible explanation for these findings is that the state-level rates for non-disabled adults are better-representative of structural phenomena, compared to rates for disabled adults. This explanation accounts for why disabled adult outcomes are best predicted by non-disabled adult social determinants. However, that also emphasizes the need for thoughtful legal and policy decisions as some populations directly impact the outcomes of others, potentially leaving them behind.
Our analysis focuses on a singular outcome (housing) of community well-being and inclusion. However, our findings highlight the complex and multifaceted nature of poor housing, as well as the interrelated domains of SDOH on housing outcomes. Using this lens, we emphasize the interrelated but not interdependent aspects of SDOH domains and how the inclusion of disabled individuals must grapple with a holistic approach across all SDOH domains.
Future research should continue to explore the complex interrelationship between disabled and non-disabled populations, as well as build out better proxy variables for SDOH domains. Multi-level modeling may be instructive in further understanding the interplay between state, county and individual factors that influence housing quality for disabled adults, as well as addressing smaller geographies of social and community context.
Study limitations
The results of this study must be considered in the context of several limitations. While using a SDOH lens to examine these factors provides a theoretical strength, it also presents an analytical challenge, because no standard variables or measures exist for the five domains of social determinants. Moreover, since this study used state-level data across all SDOH domains using proxy variables to represent these domains, the sample size of 51 limited the number of variables we could include in our analyses. While we recognize that each SDOH area is complex and multifaceted, we prioritized statistical power to obtain meaningful study results. We are hopeful that future studies can include county-level data (not currently publicly available) that would enable us to expand the number of predictor variables and thus the dimensionality of SDOH domains without sacrificing statistical power.
In addition, we were limited to the variables that exist in public, national data sources, which naturally limited our availability of SDOH domain proxy variables. For instance, this study demonstrated that voter turnout is not a good proxy variable for the social and community context. Moreover, a more nuanced application representing education may be more insightful for future studies to understand housing challenges for disabled adults. With these limitations in mind, we opted to conceptualize the five SDOH domains using clear, understandable, and publicly available proxy variables to understand their relationship with poor housing in the context of disability. We believe this first attempt at using state-level data deepens our understanding of poor housing and is an important step in identifying future directions for disability research in the context of housing.
Finally, we recognize that disability is much more complex and nuanced than simply the presence or absence of disability. The challenge is that state-level data for SDOH proxy variables by disability type is not currently publicly available. Future research to better understand differences between disability types at the community level is critical.
Regardless of its limitations, this study amplifies the reality that disabled adults, in many aspects, are simply left behind. Compared to non-disabled adults, a higher percentage of disabled adults reside in poor housing, have lower state-level employment rates, lower rates of 4-year college degrees, and have lower voter turnout. With the guidance of a SDOH lens, we argue that structural-level effects provide the largest explanation for disabled adults in poor housing. When better outcomes for non-disabled adults spill-over, disabled adults can benefit, as we see in the case of employment improvements. However, the inverse is also true. When the benefits to non-disabled adults lead to competition or exclusion, disabled adults are negatively impacted and these penalties hit harder. This double jeopardy points to the disenfranchisement of disabled adults as a structural effect and highlights the need to fully incorporate a SDOH perspective in research, policy, and law to address how the interrelated aspects of living space, work, and play impact individual well-being, In addition, our research highlights how changes to one population (non-disabled adults) can dramatically impact the outcomes and well-being of another population (disabled adults) both positively and negatively.
Conclusion
Results from this study suggest that people with disabilities continue to lack an equitable chance of achieving the safe, accessible, and affordable housing they deserve. By using state-level, rather than individual-level, data, results from this study corroborate that issues directly impacting adults with disabilities are related to broad, “upstream” factors rather than factors determined by behavioral and psychosocial factors. Furthermore, these results demonstrate that SDOH domains are interrelated but not interdependent, and that complex relationships exist between social determinants of health for disabled adults. From this vantage point, it is evident that SDOH are all deeply and closely interwoven, magnifying that SDOH are not just a “one topic” issue, but rather a dynamic set of issues that need to be accounted for collectively. Most importantly, results from this analysis continue to demonstrate that people with disabilities are left behind across a number of SDOH domains. Thus, there is an urgent need to re-examine policies and practices for all disabled people, and to adopt those that support greater housing inclusion, accessibility, and affordability for the betterment of society. According to Hahn 33 while incorporating SDOH into practice will expand public health benefits, it will also require new collaboration, research, policy, and practice.
Footnotes
Acknowledgements
The authors wish to gratefully acknowledge the U.S. Census Bureau and the Disability Statistics Compendium authors for their valuable contributions which served as the basis for this research.
ORCID iDs
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.