
Abstract
Aims:
People with intellectual disability experience stark health inequalities, often because of poor access to mainstream healthcare. This scoping review aimed to identify factors that influence access to healthcare for people with intellectual disability using Levesque and colleagues’ comprehensive framework of healthcare access.
Method:
This review followed Joanna Briggs Institute guidelines. Articles were identified and retrieved from CINAHL, PsycINFO, PubMed and EMBASE. Two reviewers completed abstract and full-text screening, addressing any conflicts at each stage. Data was extracted and coded deductively, according to the supply (healthcare provider) and demand (healthcare seeker) dimensions of Levesque and colleagues’ framework.
Results:
Following search and screening, 66 references were included for review. Barriers to healthcare were more frequently identified in the literature compared to facilitators, with most information relating to supply-side dimensions. Barriers were related to inaccessible health information, low health literacy, stigma and discrimination by healthcare providers, and lack of organisational support, training and resourcing in both healthcare and support sectors. Facilitators often involved specialist workforces, strong interpersonal skills among healthcare providers, and advocacy from supporters. Importantly, findings indicated that both sociohistorical processes and support networks are necessary to understanding access experiences for people with intellectual disability.
Conclusions:
Keywords
Background
Equitable access to healthcare is a fundamental human right that improves health outcomes and underpins quality of life [1]. Despite this, people with intellectual disability experience a range of healthcare barriers such as inaccessible health information [2], complex health systems [3], poor communication [4], untrained providers [5, 6] and inconsistent implementations of reasonable adjustments [7]. These barriers have serious consequences for the wellbeing and life expectancy of people with intellectual disability. International studies report a median age of death between 50 and 54 years old for this group [8–10] and common causes of death – for example, circulatory and respiratory diseases and cancer – are largely unrelated to the aetiology of the disability. This suggests that many deaths could be prevented with improved healthcare access. Nonetheless, a comprehensive review of access to healthcare has not yet been undertaken. To address this gap, this scoping review explores the experiences of healthcare access for people with intellectual disability, their support networks, and healthcare professionals, using Levesque et al.’s person-centred framework of access [11].
Challenges faced by people with intellectual disability accessing healthcare are often attributed to historic policies of institutionalisation, whereby people with disability were made to live in state-run facilities. Facilities were responsible for providing all the necessary services and supports, essentially segregating people from mainstream society and services [12]. Institutionalisation was rooted in the perspective that disability is a characteristic of a person (i.e. the medical model), as opposed to an outcome of societal barriers to participation (i.e. the social model) [13]. Despite recent expansive reform, these policies have persistent consequences for how people with intellectual disability experience healthcare today.
Namely, as people with intellectual disability transitioned to more mainstream health services, the models of care used by services failed to mature to address the diverse medical and support needs of this population. Likewise, the training needs of health professionals were overlooked resulting in an ill-equipped health sector. These failures were made by both the health services themselves and the broader policy and healthcare initiatives. As a result, healthcare providers still assume support to be the responsibility of informal supporters (e.g. family carers) or the disability sector [14], and fail to engage in effective collaboration with all stakeholders. Compounding these issues are the continued experiences of ableism within both social and medical systems [15]. Ableism reinforces the historic disempowerment of people with intellectual disability to form expectations of services, to make demands, or to advocate for their own healthcare. It also influences healthcare providers’ approaches towards patients with intellectual disability, their ability to form working relationships, and their assumptions and perceptions about prognoses and quality of life [16]. Thus, people with intellectual disability not only face unique barriers to healthcare access (e.g. ableist attitudes, lack of expertise among providers), but also the barriers experienced by the general population are further exacerbated for this group due to their being overlooked in public health initiatives (e.g. lack of publicly available health information in alternative communication formats). Addressing these sociohistorical and systemic access issues first requires understanding how to conceptualise healthcare access for this group.
Earlier frameworks of healthcare access tended to focus on either the role of the healthcare provider and the performance of health systems, or on the healthcare user and their ability to seek and obtain care [17, 18]. Healthcare access is now understood to involve dynamic interactions between both providers and users. It is determined by the availability of resources and opportunities within health services, and a person’s capacity to act on such opportunities to access care [19, 20]. This has also been conceptualised as the ‘fit’ between the needs of the person and the ability of the healthcare service to meet those needs [19].
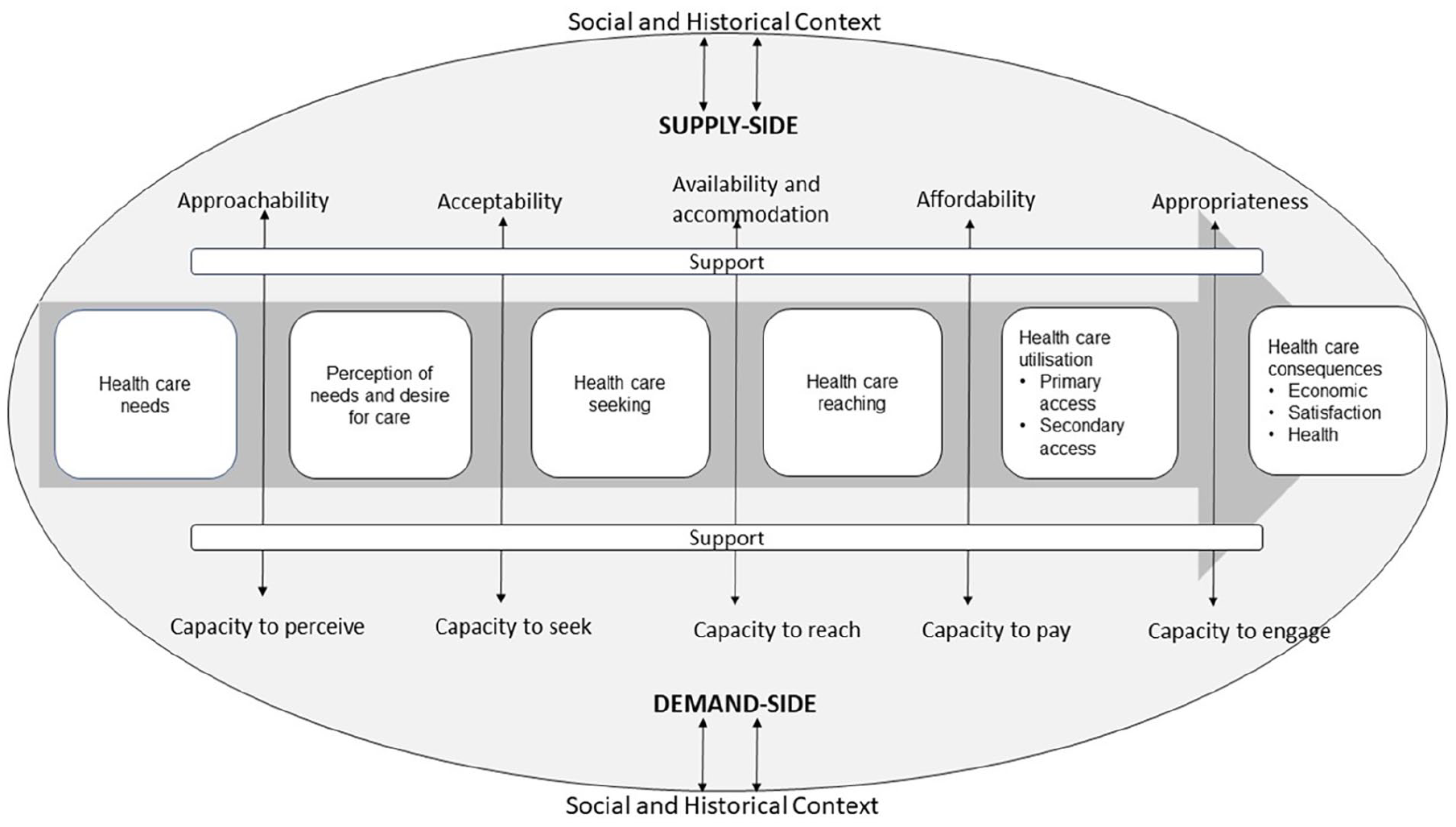
Levesque et al. [11] further developed these concepts with a framework of access that identifies both supply- and demand-side determinants along the entire healthcare journey (see Figure 1). The supply-side determinants refer to health services and include their approachability, acceptability, availability and accommodation, affordability, and appropriateness. The social and individual determinants on the demand-side refer to the healthcare user’s ability to perceive, seek, reach, pay and engage in healthcare. Stages of the healthcare journey are conceptualised up to and including the utilisation and quality of healthcare. This is a particularly useful feature of the model for understanding access in populations that face stigma and inadequate care even after ‘reaching’ a service, including people with intellectual disability [15, 21]. While Levesque et al. use the terminology of ‘ability’ on the demand-side, this review uses the term ‘capacity’ to reflect arguments that people can access healthcare only when the right supports are available (i.e. when they have the capacity to).
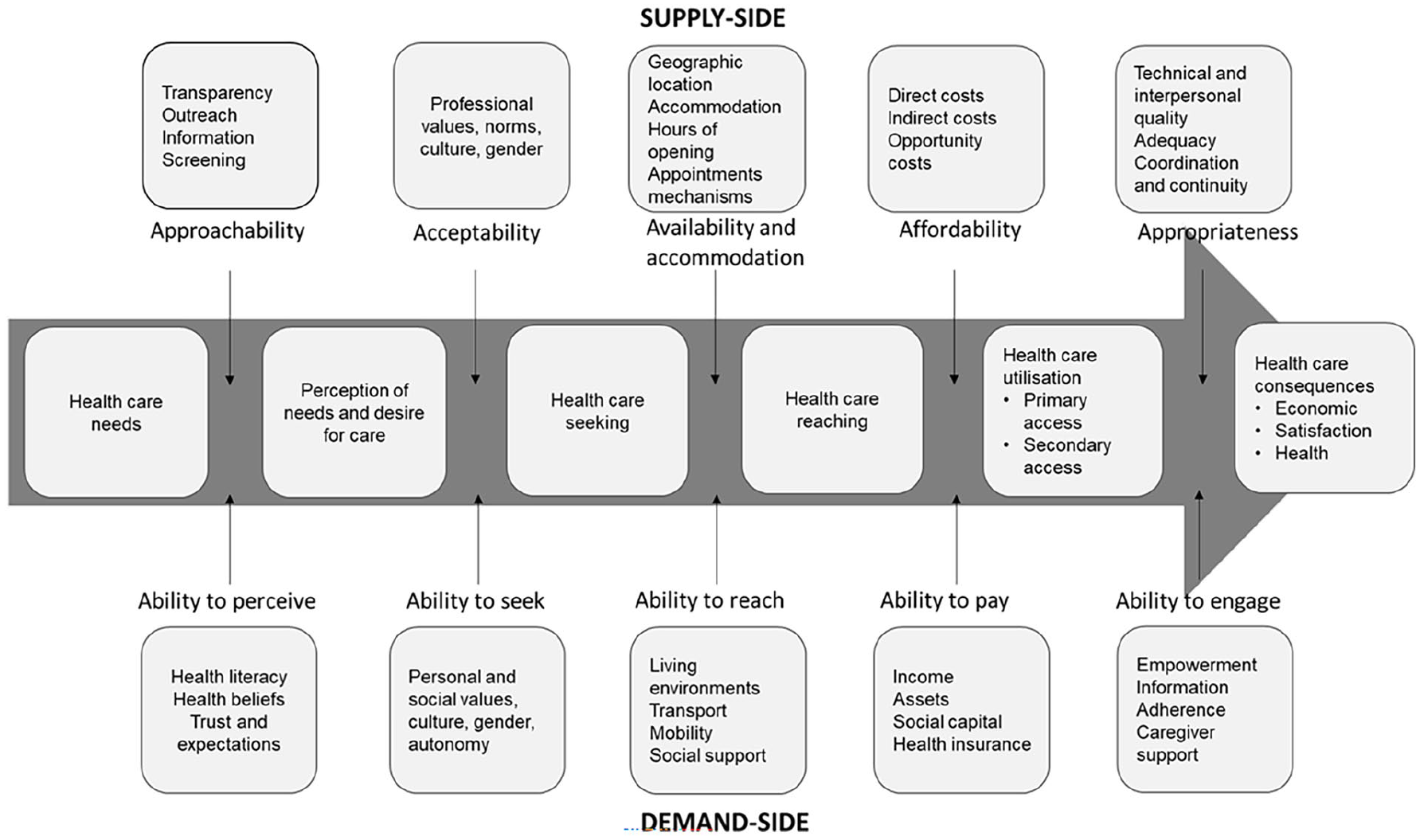
Levesque et al.’s model of healthcare access demonstrating both supply- and demand-side dimensions influencing healthcare access across the healthcare journey.
Levesque et al.’s framework has been successfully used and modified to explore healthcare experiences across diverse populations and contexts [22]. This includes identifying challenges in healthcare access for Indigenous peoples [23] and deaf and hard-of-hearing communities [24], as well as in how people with intellectual disability and their supporters access disability services in Australia [25]. This highlights the model’s adaptability to the unique characteristics, experiences and factors affecting access for different populations. To the best of our knowledge, there is only one prior scoping review of healthcare access for people with intellectual disability that uses Levesque et al.’s framework [26]. These authors focussed on studies investigating Australian general practice, with half the included papers associated with the same research group in Queensland. Conclusions about barriers and facilitators on the demand- and supply-side were thus context-limited. The authors identified consultation times, training of general practitioners, and communication between patient and provider as important factors influencing access. In contrast, there are currently no reviews summarising the broader experiences of healthcare access for people with intellectual disability internationally and across a variety of healthcare contexts.
Aim
The current review aimed to explore the experiences of healthcare access, including barriers and facilitators, from the perspectives of people with intellectual disability, their support networks, and healthcare providers. This allows for the identification of potential best practice, systemic and universal barriers, and conceptual considerations for how to understand access for this group. It also provides the opportunity to examine how well Levesque et al.’s conceptual framework captures experiences of healthcare access for people with intellectual disability. To achieve these aims, evidence from the literature was interpreted using Levesque et al.’s model and considerations of any revisions to the model were made based on this interpretation of the literature.
Methods
Research question
The research question guiding this review was ‘what are the experiences of people with intellectual disability, their support networks, and healthcare providers when accessing healthcare?’
Eligibility criteria and search strategy
The review followed the methodology laid out by the Joanna Briggs Institute in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist [27]. A protocol is available on Open Science Framework (https://osf.io/9fkz4). Eligibility criteria were decided using the Population, Concept, Context (PCC) framework [28]. The population of interest was people with intellectual disability, their support networks, and healthcare staff working with people with intellectual disability. Sources considered for inclusion had to focus on healthcare access. Access is defined as a multidimensional concept encapsulating factors that either enable or impede the likelihood of reaching out to, receiving, and/or maintaining quality healthcare. These factors may be structural, environmental/social, financial, or personal, and may be a characteristic of the service provider, the population, the wider community, or another entity [11, 19]. Broad healthcare contexts were considered, encompassing primary, secondary, tertiary, clinical and community contexts.
Original studies, both qualitative and quantitative, which investigated access to healthcare for people with intellectual disability were considered for inclusion. Textbooks, editorials, reviews, conference abstracts, opinion and commentary papers were all excluded as were articles that were not available in English. There was no limit placed on year of publication, as it was predicted that many of the issues impacting access for people with intellectual disability would be similar across time.
An initial search in EMBASE was completed to identify relevant studies and note any keywords and common title and abstract words and phrases. Search terms were selected, and a full search strategy was developed in consultation with a working group composed of intellectual disability and public health researchers (see Supplemental materials). Because this review was interested in access across any healthcare context, the search terms were kept general. Search terms used included intellectual disability, learning disability, access, and healthcare. A final search was conducted in EMBASE, MEDLINE, CINAHL and PsycINFO, on 6 June 2023. A second search of the literature was conducted on 10 June 2024 to ensure the search was up to date. From this, five publications were identified and included in the final review.
Study selection
All retrieved papers were saved to EndNote, and duplicates were removed. The remaining papers were then transferred to Covidence to facilitate the screening of titles and abstracts during the selection process. Two reviewers completed blind independent title and abstract screening of all papers using the PCC criteria. After initial screening, the full texts for the remaining items were then uploaded to Covidence and were also blindly and independently screened by the same two reviewers. Any arising conflicts were resolved through discussion between the reviewers until consensus.
Data extraction and analysis
A data chart tool was developed in Excel for the purposes of this review. This tool noted the design and characteristics of each study, as well as the participant group(s) included and the healthcare setting in which it took place. The chart involved mapping barriers and facilitators to access identified in studies according to the supply- and demand-side dimensions of Levesque et al.’s framework. Given that past studies found adjustments of the model were required to better reflect experiences of other vulnerable populations [23, 24], there was a final column added to the chart for noting any key points or conclusions that did not easily fit into Levesque’s framework. One reviewer performed pilot data extraction on three randomly selected texts to examine the functionality of the charting tool. Texts were then divided between two reviewers for data extraction, due to resourcing practicalities. Regular discussions were had between the two reviewers about approaches taken and challenges experienced, and adjustments were made where required. This ensured consistency in our approach. The findings were then discussed with the working group to guide interpretation.
Quality review
While not a requirement of a scoping review, a quality assessment of the literature was performed using Hawker et al.’s [29] critical appraisal tool for assessing studies from different paradigms. This tool involved scoring publications according to nine quality criteria using 4-point scales ranging from 1 – Very poor to 4 – Good. Criteria assessed the quality of a publication’s abstract, introduction, method, sampling, analysis, reporting of ethics and bias, reporting of results, generalisability, and reporting of implications. Scores between 9 and 23 are considered to be of ‘poor’ quality, between 24 and 28 are ‘moderate’, and those between 29 and 36 ‘good’.
Results
Characteristics of studies
The initial search returned 1078 publications and the second search identified a further five recently published items resulting in 1083 publications imported from databases (Figure 2). After removing duplicates and undertaking title and abstract, and full-text screening, 66 publications were included in the review. The characteristics of all 66 studies are available in the Supplemental materials. All publications were empirical, with most using qualitative methods (n = 45), followed by mixed methods (n = 12) and quantitative methods (n = 9). Studies were from middle-to-high-income countries including the UK (n = 40), other high-income European countries (n = 11), Australia (n = 7), Malaysia (n = 1) and North America (n = 6), or a combination of European and North American countries (n = 1). Publications included participants with intellectual disability (n = 33), formal and informal supporters (n = 41) and healthcare providers (n = 30).
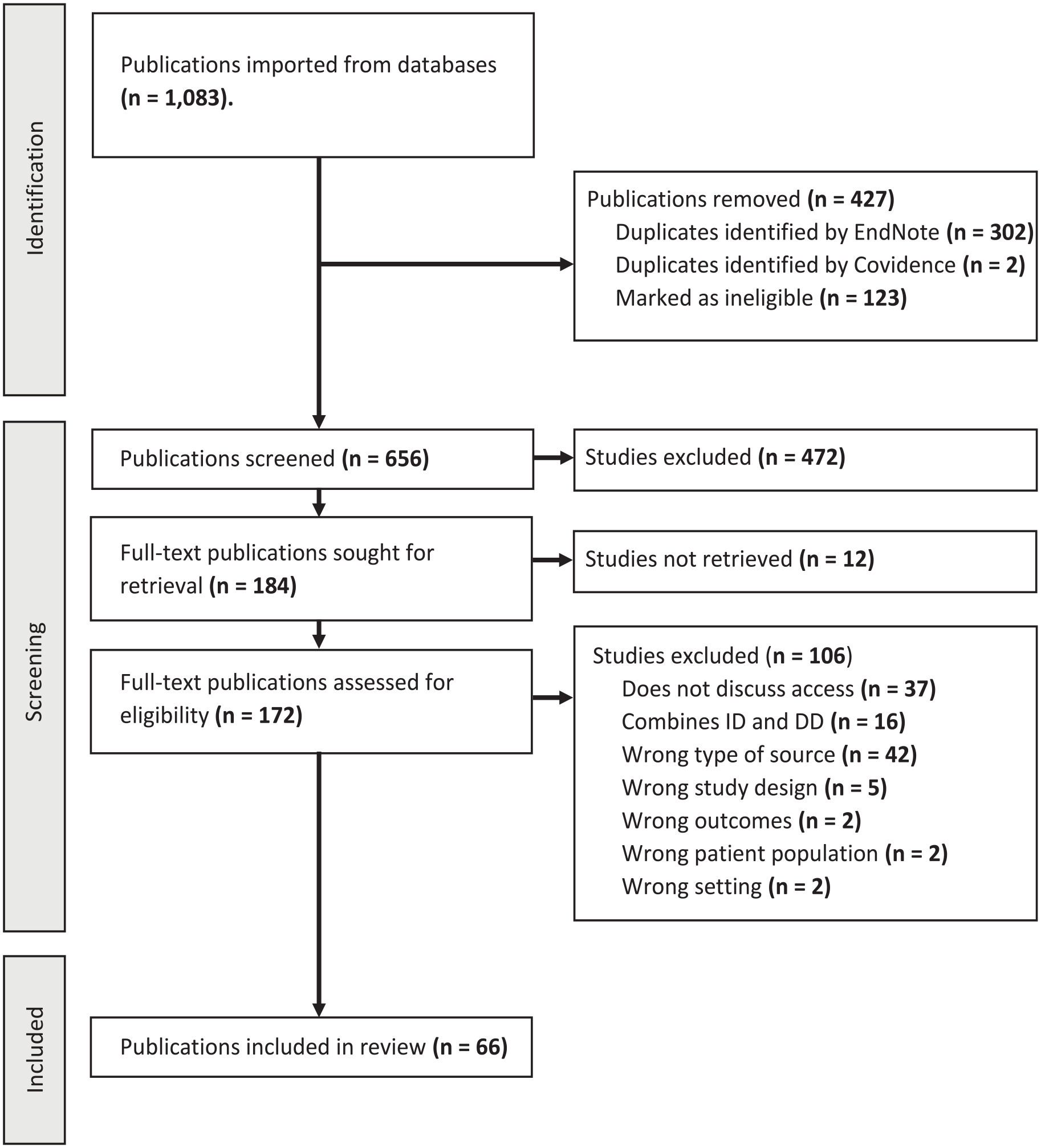
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram of search and data extraction.
Quality assessment
The overall quality of included publications was acceptable, with an average score of 30 and a range of 16–36. Forty-three studies were graded as ‘good’, 20 as ‘moderate’ and 3 as ‘poor’ quality. The most common issue was a lack of reflexivity, with most qualitative studies failing to reflect on or acknowledge potential biases of the researchers. Other issues were failures to identify aims or research questions, detail the method used, provide descriptive information about participant samples, or generate ideas for future directions.
Findings
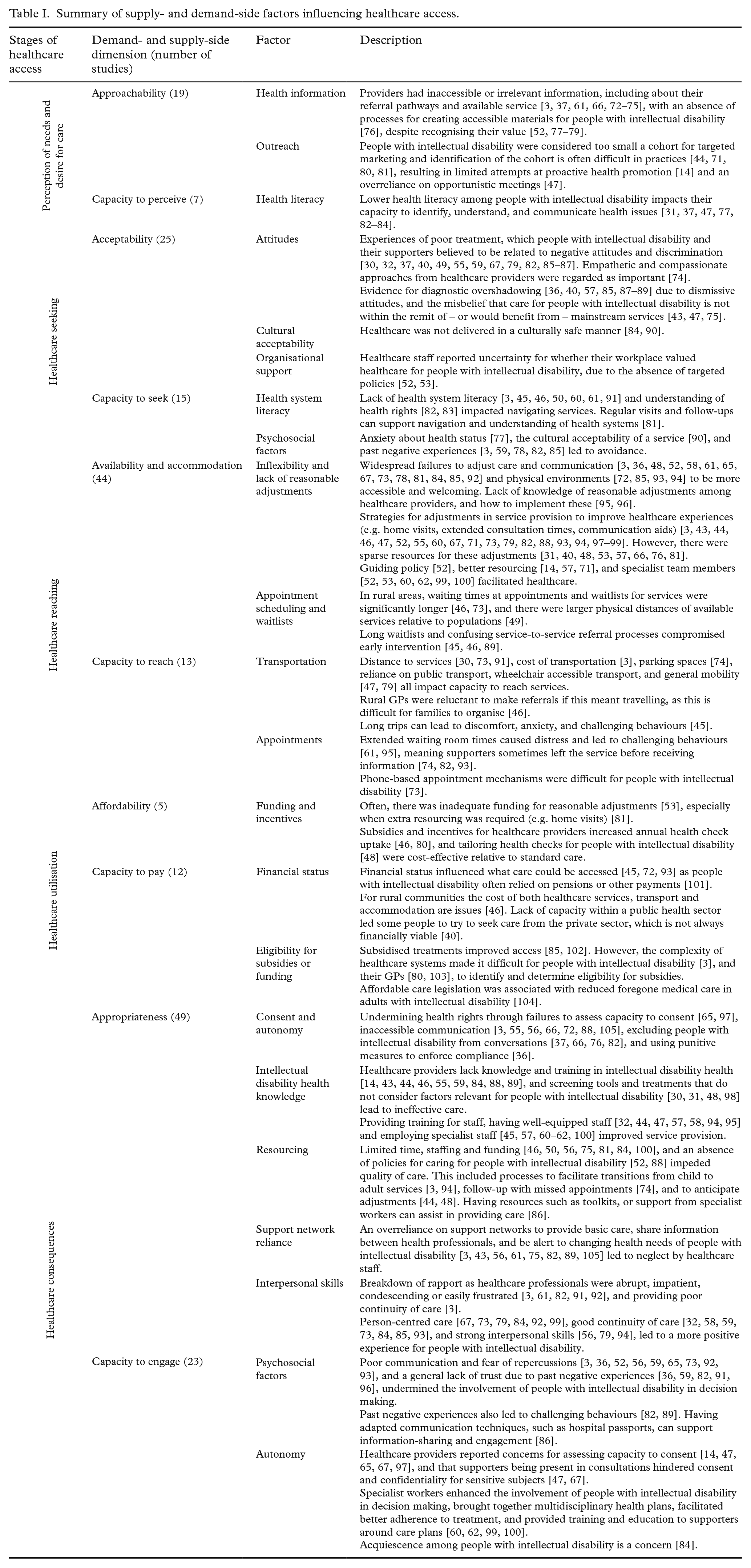
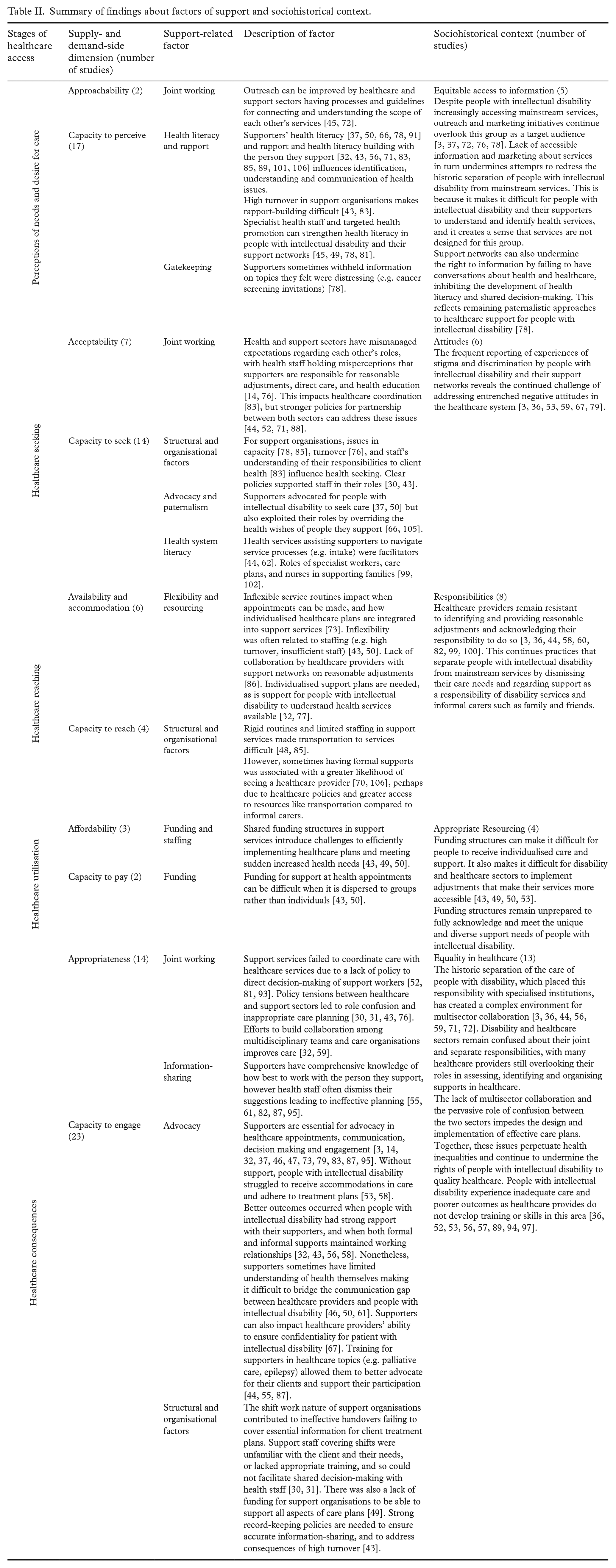
Barriers and facilitators to healthcare access that were identified in this review are reported in Table I according to their respective dimensions of Levesque et al.’s conceptual framework. Interestingly, our interpretation of the findings indicated that support and sociohistorical context have a significant influence on access experiences. These findings are outlined in Table II, and are not as readily accounted for by the conceptual framework, suggesting that adjustments should be made to the model to integrate these factors. This section describes the key findings from the studies included in this review.
Summary of supply- and demand-side factors influencing healthcare access.
Summary of findings about factors of support and sociohistorical context.
In Table I, studies identified more barriers than facilitators, with most evidence related to supply-side factors of acceptability (n = 25), availability and accommodation (n = 44), and appropriateness (n = 51). Comparatively less focus was on the demand-side, and most information here regarded the capacity of people with intellectual disability to engage (n = 23). There was limited information on factors that influenced affordability of services (n = 5) and the capacity to reach (n = 14) and pay for (n = 13) services.
On the supply-side structural barriers among healthcare organisations were frequently reported, including a widespread lack of policy, training and knowledge in intellectual disability health. Stigmatising beliefs held by healthcare professionals were also identified, as were practices that undermined the autonomy of people with intellectual disability and their ability to consent to healthcare. These key barriers reflect inequalities faced by people with intellectual disability when their needs are ignored, and they are discriminated against in healthcare systems. Demand-side barriers were commonly related to limited health literacy and understanding of health rights, and financial and transportation difficulties. Further, the stigma experienced by people with intellectual disability from their healthcare workers was found to have contributed to psychosocial barriers on the demand-side, such as anxiety, distrust, and avoidance of health services. Facilitators on both the supply- and demand-sides included specialist health staff, targeted training and policies for health and support professionals, policies guiding reasonable adjustments, and targeted outreach and funding initiatives.
While many of the barriers and facilitators aligned with the framework, interpretation of the evidence suggested two additional considerations important to understanding the experiences of people with intellectual disability. First, Table II demonstrates that the role of supporters emerged as a separable dimension on both supply- and demand-sides. On the supply-side, support networks utilised their personal knowledge of, and rapport with, the people they support to provide guidance to healthcare staff. Moreover, the policies, processes and resources of formal support organisations interact with those of health services and can either help or hinder access [30–32]. For the demand-side, supporters had a role in identifying health problems, connecting to services, and promoting adherence to treatment plans.
Second, Table II demonstrates how many of the barriers and facilitators identified reveal the ongoing influence of sociohistorical processes on access. This included a lack of access to information about health and services, lasting negative attitudes among healthcare staff, failures of disability and health sectors to develop joint working initiatives and negotiate their responsibilities, under-resourcing for providing support, and ultimately inequalities in healthcare experiences. By acknowledging the sociohistorical context within which access occurs, we can understand how many of the barriers experienced by people with intellectual disability result from, perpetuate or amplify healthcare inequalities due to broader negative attitudes toward this group.
Discussion
This scoping review applied Levesque et al.’s model of healthcare access to understand the experiences of people with intellectual disability, their support networks and healthcare providers. Common structural barriers identified on the supply-side included a lack of training and policy and inadequate provision of care. Low health literacy and psychosocial factors (e.g. fear and anxiety) on the demand-side were reported among people with intellectual disability and their supporters. Availability of specialist staff, communication strategies, advocacy, and reasonable adjustments were endorsed as facilitators. While these findings fit within the dimensions of Levesque et al.’s model, interpretation of the evidence importantly suggested that greater integration of the sociohistorical context and support networks in the model can inform our understanding of healthcare access for people with intellectual disability.
On the supply-side, findings of widespread absences in policies and processes that consider healthcare support for people with intellectual disability (both in health and disability services) revealed the continued systemic neglect of the healthcare of this group. There were also barriers consistent with those experienced by the general population (e.g. low health literacy, poor communication and medical mistrust). While these barriers are common for many groups, they are often amplified or sustained for people with intellectual disability. This is because initiatives to address these barriers frequently overlook the needs of people with intellectual disability. For example, poor communication in healthcare is experienced by people with and without intellectual disability [4, 33, 34]. However, initiatives by healthcare services to improve their communication for patients are often designed for the communication needs of people without intellectual disability (e.g. interpreters, teach-back techniques and plain language) [35]. Alternative communication techniques (e.g. easy read, non-verbal communication and assistive devices) are less frequently considered or implemented.
Moreover, people with intellectual disability and their supporters frequently reported inequalities in healthcare systems such as inadequate care, lack of consent and inclusion in decision making, and discrimination. Discrimination and inadequate care contribute to anxiety and avoidance in people with intellectual disability and their supporters. Issues in care also have implications for demand-side processes, as evidence demonstrated that support is essential for people with intellectual disability to have the capacity to seek and reach appropriate services and engage in their own healthcare. Despite intentions to address institutionalisation and de-segregate healthcare, services evidently remain confused about their roles and responsibilities to this group [3, 36–39]. Indeed, studies published prior to and over the last 10 years found consistent issues in access, implying that they are deeply entrenched. Confronting the historic consequences of institutionalisation requires developing a workforce that has the training and resourcing necessary to uphold the health rights and respect the support needs of people with intellectual disability [36, 40]. While Levesque et al. acknowledge the sociocultural influences in their model [11], this review indicates that ongoing historic challenges encompass the healthcare experience. The revised model in Figure 3 proposes that sociohistorical influences feed into both supply-side accessibility and demand-side capacity to access, as visualised with arrows. These influences cause specific barriers for people with intellectual disability (e.g. exclusion from decision making and consent in their own care) and exacerbate general barriers experienced in the healthcare system (e.g. health literacy and accessibility of health information).
Modified framework of healthcare access for people with intellectual disability, which illustrates the proposed roles of support and the sociohistorical context in influencing the healthcare access experiences of people with intellectual disability.
The current failures of healthcare systems to meet the needs of people with intellectual disability also highlight the pivotal role of support [41]. Everyone relies on support to some extent and in some form (e.g. social support, formal support) when managing their health [42]. Support needs are often complex and diverse, particularly for people with intellectual disability. This review demonstrated that support influences both the supply- and demand-sides of access and can act as either a facilitator or barrier throughout the healthcare journey. When using their roles to advocate for people with intellectual disability in health spaces and developing their own health skills and knowledge, supporters become critical to facilitating access [32, 43–46]. However, gatekeeping and paternalistic approaches to support undermine the autonomy of people with intellectual disability and limit their access to their own healthcare [37, 47].
Further complications arise from formal support organisations from their own policies and processes. Conflicting policies between health and support sectors can limit joint working. This review found that organisational issues in support sector staffing, culture, funding and policy all impeded access to health services for people with intellectual disability and influenced support sector collaboration with health services [43, 48, 49]. Furthermore, inadequate training and processes for support staff impede their ability to navigate health systems and coordinate care, ultimately limiting the support they can provide [45, 50]. Acknowledging the broad and influential role of supporters (formal and informal), both in their interactions with health services and the people they support, is a necessary feature of a model of healthcare access for people with intellectual disability. We have represented this in rectangles running across all supply- and demand-side dimensions in the model, as shown in Figure 3.
There are many areas where action can be taken to address issues in access equality and improve healthcare for people with intellectual disability. For example, stronger health legislation can act as an impetus for improving health services for this population. While existing anti-discrimination acts (e.g. the UK Equality Act 2010 and the Australian Disability Discrimination Act 1992) provide foundational work to protecting the rights of people with intellectual disability, Australia’s recent Disability Royal Commission recommends the right to equitable access to healthcare be enshrined in legislation and key policy agreements [51]. Legislation that is enforced creates an obligation to design and implement national guidelines that specifically consider the provision of accessible information and reasonable adjustments and protect consent for people with intellectual disability [52, 53]. Such guidelines already exist for the general population, however engrained social inequalities of people with intellectual disability often mean that general policies are not effective for addressing barriers for this group. Guidelines should have measurable outcomes and regular evaluation to ensure transparency, commitment and accountability. In addition, support for people with intellectual disability often takes place within complex systems of disability and healthcare sectors, as well as other sectors relating to the person’s intersectional experiences. Inter-sector agreement on roles and responsibilities needs to be established. Doing so, however, requires organisations to identify the practical challenges or concerns faced by their staff to facilitate healthcare access and address these in their workforce development goals, policies and processes [31]. Policies are central to guiding decision making for staff, to establishing organisational priorities and values, and providing the necessary support to healthcare and support staff in their roles.
More broadly, national initiatives to address negative attitudes toward people with intellectual disability that remain in society will also improve healthcare experiences. Consistent with findings from this review, the World Health Organization outlines how societal attitudes influence healthcare systems through discrimination in healthcare policies, processes, and governance, and through delayed healthcare seeking due to lack of community support or awareness [54]. Governments should engage in efforts to improve the visibility and inclusion of people with intellectual disability in communities. What this might entail has been debated, but would require large-scale restructuring of models for specialist schools, group homes, and other forms of segregated services [38]. Indeed, enabling greater choice for people with intellectual disability about their education, employment and living arrangements creates an expectation for collaborative and inclusive health systems too.
There are also implications for healthcare practice. Current models of care have not been updated or designed to consider the needs of people with intellectual disability, which creates barriers for healthcare workers trying to address the inequalities faced by, and meet the complex health and support needs of people with intellectual disability. Current models also impede joint working and coordination with support networks. Redeveloping service delivery offers an opportunity to explicitly include critical areas such as training needs for staff in disability and health sectors, and opportunities for facilitating understanding between these sectors. Models could also be designed to offer better processes for overcoming key barriers in communication, assessments of consent, and provision of reasonable adjustments [53, 55–59].
As mainstream workforces are presently ill-equipped, there remains an important role for specialist support and knowledge (e.g. learning disability nurses in the UK). Literature included in this review regarded specialist staff as essential to providing advice to healthcare professionals and support networks, facilitating reasonable adjustments, and anticipating functional support needs [52, 53, 60–62]. Future services models should therefore consider the role of specialist workforces. They should also consider the vital role of support as found in this scoping review, and ensure policies and practice enable supporters to be present and included in healthcare to the extent that is reasonable, while also maintaining the consent and autonomy of patients with intellectual disability. Most importantly, updating models of care must be a codesigned endeavour, including the expertise of people with lived experience of intellectual disability, as well as healthcare professionals, disability sector staff, formal and informal carers, and other support networks. Collaboration on new models of care will be a central mechanism for enhancing healthcare access and correcting the failures of health services to include people with intellectual disability in their own care.
While interventions targeting the structures and delivery of healthcare services on the supply-side are often discussed, interventions to support and empower consumers on the demand-side are comparatively lacking [63]. Support networks and specialist health workers were frequently identified as having a central role in advocating for people with intellectual disability to ensure their health needs were met [32, 37, 50, 60]. Advocacy is often described as a way of acting to promote or protect the interests of a person or group with minimal conflict of interest [64]. There were fewer examples of advocacy used to uphold the autonomy and consent rights of people with intellectual disability, or of people with intellectual disability self-advocating for their own rights. This gap is concerning given the findings that healthcare staff and supporters can undermine consent through gatekeeping, failing to facilitate shared decision-making or adapt communication [3, 36, 37, 47, 65–67]. The ongoing systemic advocacy by intellectual disability organisations could change government and sector priorities to better respect the rights of patients with intellectual disability [68]. Importantly however, interventions aimed at building skills for self-advocacy in people with intellectual disability could protect against gatekeeping and paternalistic approaches both by health workers and support networks [69].
A strength of this study was the inclusion of evidence from multiple countries and healthcare contexts. This allowed for identification of systemic and universal barriers, as well as the different strategies being adopted to address these barriers. Participants also provided diverse perspectives on the issue as studies included health staff, support networks, and people with intellectual disability. Nonetheless, it is possible that some relevant papers were missed as the search terms for this scoping review were limited to select keywords and to English-language papers to make the search more manageable. However, given the consistency and similarity in barriers highlighted across studies that were included, any missed papers would be unlikely to significantly change the findings of this review.
Areas for further research have also been identified. Using Levesque et al.’s model to chart the literature revealed a weaker evidence base for barriers and facilitators regarding affordability and capacity to pay. Yet people with intellectual disability are more likely to experience poverty or be socioeconomically disadvantaged, suggesting these dimensions would be an influential part of their healthcare experience and should be investigated further. Likewise, rurality is an issue known to impact healthcare access for the general population and people with intellectual disability. Only four studies in this review explored how rurality impacted people with intellectual disability [46, 49, 70, 71]. Rurality may have been less represented in other studies as they tended to focus on the experiences of people with intellectual disability in metropolitan areas. It is also possible that many of the qualitative studies did not include questions designed to elicit responses about barriers faced by people in more rural communities, or that while there are specific barriers to access in rural communities, other barriers could be more prominent for participants when reflecting on their experiences. That is, when people report on their access experiences, they may more readily draw on appropriateness and capacity to engage. These domains featured most prominently in the data analysed. In contrast, other known issues such as capacity to pay or reach – while still important – are not as readily reported. Given that we know financial and rural experiences impact healthcare access, future research should aim to investigate these factors more explicitly.
In addition, the articles included in this review were representative of high-income countries only, as there were no relevant English-language studies published from low-income countries. Representation of intersectional issues and experiences were also lacking, as the studies did not capture the experiences of LGBTQIA+ people with intellectual disability, and only a small number of studies identified issues for women, Indigenous peoples, and culturally and linguistically diverse communities. Future work should seek to include diverse voices and experiences among people with intellectual disability. While the quality of included studies was generally acceptable, any efforts to address these research gaps will need to give particular attention to reflexivity in their methodology and ensure clear reporting on this process. These were key areas of weakness among many of the included publications.
Conclusions
Using Levesque’s comprehensive model, this review has contributed to the understanding of healthcare access for people with intellectual disability. The results represent findings across a number of countries and healthcare contexts and reveal the universal nature of the challenges people with intellectual disability face. The barriers and facilitators identified in this study will inform future efforts to design inclusive healthcare systems, and improve the support provided to people with intellectual disability as they navigate their health and healthcare. Importantly, interpretation of the literature also indicated that integrating both the sociohistorical context and the complex nature of support networks is necessary to understanding access for people with intellectual disability.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948251317243 – Supplemental material for Access to healthcare for people with intellectual disability: a scoping review
Supplemental material, sj-docx-1-sjp-10.1177_14034948251317243 for Access to healthcare for people with intellectual disability: a scoping review by Maryann Barrington, Karen R. Fisher, Ben Harris-Roxas, Catherine Spooner, Julian N. Trollor and Janelle Weise in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Health and Medical Research Council research grant (grant no. 2006240).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.