
Abstract
Objectives:
Chronic illnesses have been linked to elevated risks of hospitalization and mortality during the COVID 19 pandemic. While many studies have examined how specific comorbidities influence outcomes among hospitalized COVID 19 patients, less is known about how the pandemic affected all cause mortality among comorbid individuals in the general population. Our objective is to assess how the number of pre pandemic comorbidities interacted with COVID 19 and whether all cause mortality risks for individuals with comorbidities changed during the pandemic.
Methods:
This is a population-based retrospective cohort study, where we analyzed the entire Danish population aged 45 years and older using nationwide registry data. We examined COVID 19 specific and non COVID 19 mortality in 2020–2021 to capture both direct and indirect pandemic effects. Survival analysis techniques were applied to estimate mortality patterns across comorbidity levels.
Results:
Kaplan–Meier curves indicated that traditional comorbidity gradients persisted for non COVID mortality, whereas COVID 19 mortality showed a relative equalization across comorbidity groups. Gender and educational disparities remained evident.
Conclusion:
The findings highlight the need for preparedness strategies that protect medically vulnerable groups while addressing persistent social inequalities. They also demonstrate the importance of population wide approaches for understanding the full mortality impact of pandemics.
Introduction
The COVID-19 pandemic has highlighted the critical role of underlying health conditions in shaping health disparities. Chronic illnesses have shown a clear link with a higher risk of hospitalization and mortality during this crisis, primarily due to shared characteristics with infectious diseases, such as heightened inflammation and weakened immune responses.
Numerous studies have explored the connection between comorbidities and hospitalization risk, focusing on post-hospitalization health outcomes in COVID-19 patients. Multiple meta-analyses have consistently shown that comorbidities are major risk factors for COVID-19 mortality.1–5 Chronic diseases, particularly cardiovascular and metabolic conditions, substantially increase the likelihood of severe outcomes in infected individuals. 6 Across studies, hypertension, diabetes, obesity, cardiovascular disease, respiratory disorders, cancer, and acute kidney injury consistently emerge as key comorbidities associated with elevated risk.7–10 Furthermore, a systematic review and meta-analysis including more than 4 million COVID-19 patients found that individuals with multiple long-term conditions had a 2.5-fold higher risk of death compared with those without multimorbidity. 11
Different comorbidities can have varying effects, as seen in a New York study where diabetic patients had a higher likelihood of invasive interventions, while hypertensive patients had a lower risk. 12 Age and age-comorbidity interactions also produce differing outcomes: younger adults with comorbidities faced higher risks, while older individuals’ frailty reduced the relative impact of comorbidities on outcomes.13,14 This is consistent with the higher overall frailty of older individuals, which makes the effect of having a comorbidity compared to not having it, less determining for a negative health outcome, while having a comorbidity at early age is a much stronger discriminatory factor for poor health outcome.
In Denmark’s initial COVID-19 wave, male patients, especially older individuals with comorbidities like hypertension, diabetes, and chronic pulmonary disease, had a higher risk of hospitalization and ICU admission. Those with chronic pulmonary disease, active cancer, and multiple comorbidities faced a significantly elevated risk of death. 15 A higher Charlson Comorbidity Index correlated with increased COVID related risks across age groups and genders. 16 Hypertension, coronary artery disease, and diabetes were common comorbidities among COVID-19 patients at North Zealand Hospital, with all ICU patients having at least one comorbidity. 17 Cardiovascular comorbidities had a modest effect on poor outcomes compared to other conditions. 18 Post-hospitalization studies yielded mixed results, with one study showing a higher risk for men and another identifying comorbidity, age, and gender as independent risk factors for death.19,20
Subsequently, a study found lower ICU admissions, reduced organ support usage, and shorter ICU stays among hospitalized COVID-19 patients, though mortality rates remained high, particularly among males, older individuals, and those with comorbidities. 21 A nationwide study involving blood donors aged 17–69 revealed a lower infection fatality rate among those under 51 without comorbidities, while older individuals without comorbidities had a higher infection fatality rate for men compared to women. 22
To summarize, comorbidities appear to play a potentially detrimental role in worsening COVID-19 outcomes in Denmark. Most studies have focused on the first wave, potentially impacted by issues in estimating infection fatality rates, and mostly on hospitalized individuals only, capturing a selected segment of the population only. However, the pandemic may have had differing effects on the mortality risk of comorbid individuals not hospitalized, either directly or indirectly. Understanding the direct and indirect effects of a pandemic is essential for capturing its full impact on population health. Direct effects, such as deaths caused by the infectious agent itself, represent only part of the overall burden. Pandemics also generate indirect consequences that can substantially alter mortality patterns, particularly among individuals with pre-existing health vulnerabilities. While cause-specific mortality captures deaths assigned to a particular cause, all-cause mortality reflects the total number of deaths from any cause. This distinction is crucial because all-cause mortality provides a more comprehensive measure of the pandemic’s impact, capturing both deaths caused by infection and those arising indirectly from healthcare disruptions, delayed treatment, or changes in health-seeking behavior.
These challenges have prompted researchers to adopt an approach centered on excess death estimation, comparing pandemic to pre-pandemic mortality, rather than focusing solely on COVID-19 mortality. 23 In our analysis, we take a similar approach, focusing on the entire population, not just hospitalized individuals. We aim to provide a more comprehensive assessment of the pandemic’s mortality burden among people affected by comorbidities. Our goal is to investigate how the number of comorbidities present prior to the pandemic interacted with COVID-19 and whether the all-cause mortality risk for individuals with comorbidities changed during the pandemic in Denmark. We will examine the first two pandemic years 2020 and 2021, including COVID-19-specific and non-COVID-19-related mortality, to assess the direct and indirect effects of the pandemic on the mortality risk of individuals with and without comorbidities. By doing so we investigate how the number of comorbidities relates to all-cause mortality at the population level, providing a comprehensive assessment of both direct and indirect effects of the pandemic. Quantifying the mortality impact on individuals with multiple comorbidities during periods of widespread mortality shocks is essential for effective public health planning and risk stratification. Mortality shocks often amplify underlying vulnerabilities, and people with high comorbidity burdens may experience disproportionately elevated risks that are not captured when focusing solely on cause-specific mortality. By measuring how all-cause mortality varies across levels of comorbidity during such events, health authorities can better identify the populations most in need of protection, allocate resources more efficiently, and refine preparedness strategies. This evidence also supports the development of more accurate risk-prediction tools and helps ensure that interventions are targeted equitably toward those who are most susceptible. This is particularly relevant in aging societies, where a growing proportion of older adults live with multiple comorbidities.
Methods
Study design
This is a retrospective cohort study comparing mortality risks between individuals with and without comorbidities among Danish residents ages 45 and older during the pre-pandemic period (2017–2019) and the pandemic period (2020–2021), independently of whether they have been hospitalized or not after contracting COVID-19.
Data sources
We utilize comprehensive, nationwide individual Danish registry data, provided by Statistics Denmark. We can link records from different registries for the same individual by using personal identifiers. Specifically, we retrieve information from the Danish Population Register, which contains demographic information including age, sex, and residence for all individuals legally residing in Denmark; the Cause of Death Register, which records the date and underlying and contributing causes of death for all deaths occurring in Denmark, coded according to ICD-10; the National Patient Register, which captures all inpatient hospital admissions in Denmark since 1977, recording diagnoses coded according to ICD-10, dates of admission and discharge; and the Education Register, which records highest achieved educational attainment for all Danish residents.
Study population
Our study population includes individuals aged 45 and older, as chronic conditions of concern are infrequently observed in younger age groups. We include all individuals in this age range regardless of their hospitalization status for COVID-19 or other conditions.
The mortality follow-up started at age 45 and ended up either by death or censoring at the end of the observation period: 2017–2019 for the pre-pandemic period and 2020–2021 for the pandemic period. Our study population includes about 2.6 million individuals overall.
Exposure
The exposure in our analysis is the number of comorbidities. We determine the presence of comorbidity based on diagnosed chronic conditions during hospitalization in the 5 years leading up to the pandemic (2015–2019), ensuring the associations are relevant to our study. We focused on specific severe chronic conditions derived from a review of the scientific literature: Neoplasms, Diabetes (type I and II), Chronic Rheumatic Heart Diseases, Angina Pectoris, Acute and Old Myocardial Infraction, Stroke, Parkinson’s Disease, Alzheimer’s Diseases, Chronic Respiratory Diseases, Cirrhosis, and Chronic Kidney Diseases. The list of chronic diseases and their respective ICD-10 codes is available in Table A1 of Supplemental Materials (SI). Based on the presence of those conditions, each individual is then classified depending on the number of comorbidities they had: none, one, two or more.
Covariates
We also included information on the highest achieved educational attainment categorized – according to the International Standard Classification of Education (ISCED) – as low (less than high school diploma), middle (high school diploma) and high (university diploma).
Outcomes
During the pre-pandemic period, we observe over 105,000 deaths. During the pandemic period, we separated the covid-related-deaths from the all the other deaths, and we observed respectively circa 2500 and 108,000 deaths.
Statistical analysis
First, we examined mortality risks for individuals with and without comorbidities using Kaplan-Meier curves and performed log-rank tests to assess whether the pandemic had varying effects on different comorbidity profiles. Afterward, we derived Nelson-Aalen estimates for the non-parametric cumulative hazard functions of men and women by level of comorbidity. Finally, we analyzed relative risks with Cox regression models, driven by our focus on understanding risk disparities rather than the exact shape of the hazard functions.
All analyses were performed using STATA version 19.5.
The reporting of this observational study conforms to the STROBE guidelines 24 (see Supplemental File).
Results
Kaplan-Meier survival curves
In Figure 1, Panel A, we observe a clear and anticipated gradient in the risk of death, ranging from a lower risk for individuals without comorbidities to a higher risk for those with a greater burden of comorbidities. Notably, women exhibit a more pronounced separation among the curves representing varying comorbidity levels.
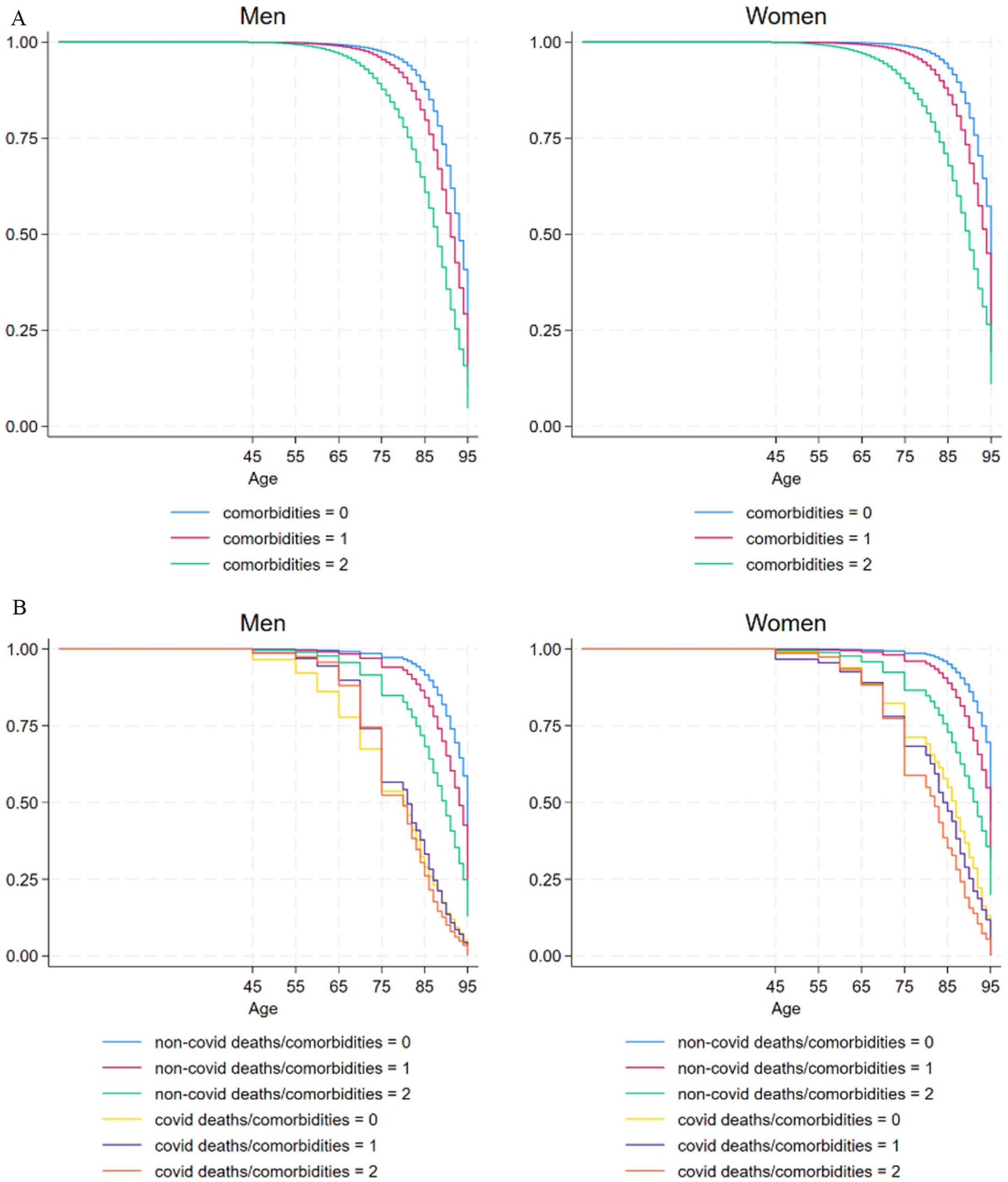
Panel A – Kaplan-Meier survival curves, all deaths from age 45 in Denmark by comorbidity level (from 0 = low to 2 = high), in pre-pandemic period (2017–2019). Panel B – Kaplan-Meier survival curves, deaths related to COVID and all other deaths, from age 45 in Denmark by comorbidity level (from 0 = low to 2 = high), in pandemic period (2020–2021).
Turning our attention to Panel B, we can see that during the pandemic, deaths unrelated to COVID-19 maintain a consistent gradient corresponding to the pre-existing level of comorbidity. However, the relationship between comorbidity and COVID-related deaths appears less pronounced, particularly among men. In fact, the Kaplan-Meier survival curves for men almost completely overlap, and the gap between curves for non-COVID-related deaths is notably narrower compared to women.
Log-rank tests for the equality of the Kaplan-Meier survival curves, shown in Table A2 of SI, confirm this. In pre-pandemic times, the survival curves of the different comorbidity levels are significantly different for both men and women; during the pandemic, different comorbidity levels, in both sexes, still show significantly different survival for non-covid deaths, while for covid-related deaths, comorbidity survival rates are significantly different for women but not for men. This means that the risk of covid related death for women during the pandemic was significantly lower for individuals with no comorbidities compared to those with one or more comorbidities, but this was not the case for men.
Nelson-Aalen cumulative hazard
Figure 2 shows the Nelson-Aalen estimate for the non-parametric cumulative hazard functions of men and women by level of comorbidity for all deaths in pre-pandemic period (Panel A) and for covid-related and non-covid related deaths during the pandemic (Panel B). Note that the y-axis scale differs between Panels A and B to reflect the higher cumulative hazard observed during the pandemic period compared to the pre-pandemic period. As expected, the cumulative hazards of death for all combinations of comorbidities and type of deaths are higher form men than for women. When it comes to covid deaths, from age 70 the cumulative risk of death from covid clearly accelerates, for both sexes and for all the levels of comorbidities, indicating a strong impact of covid on the risk of death among the elderly. However, while for men, the risk of covid-death for individuals with no comorbidities (yellow line) is clearly higher than for all the other groups until age 70, it is not the case for women, whose hazard curves for the different groups practically overlap until age 65. After age 70, the risk of covid death becomes clearly higher than the risk of non-covid related death, but for men, the three levels of comorbidities don’t have statistically different risks, while for women, those with two or more comorbidities are exposed to a significantly higher risk of death compared to those with one or no comorbidities, especially after age 80.
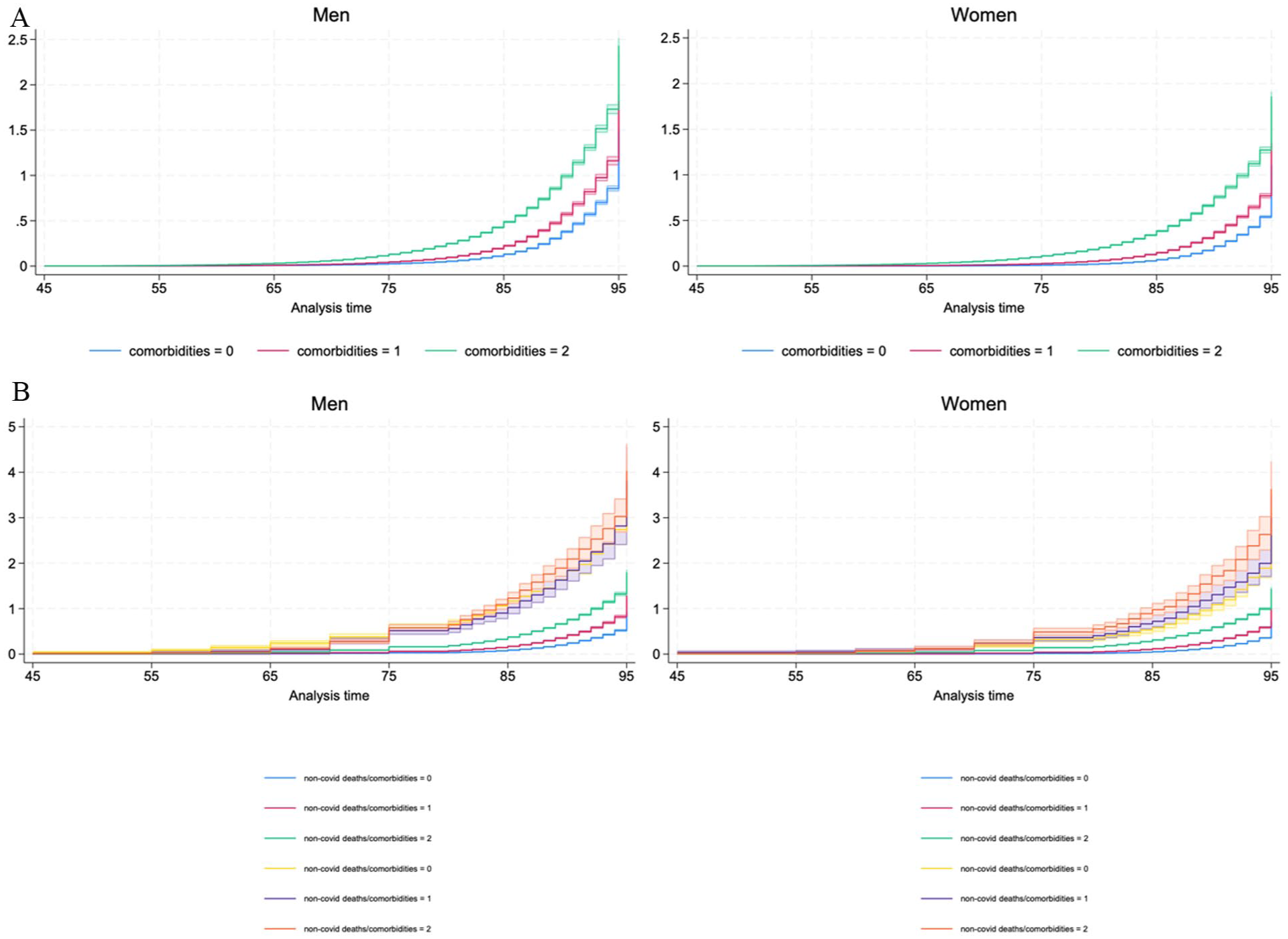
(a) Nelson-Aalen estimator for the hazard function, all deaths from age 45 in Denmark by comorbidity level (from 0 = low to 2 = high), in pre-pandemic period (2017–2019) and (b) Nelson-Aalen estimator for the hazard function, deaths related to COVID and all other deaths, from age 45 in Denmark by comorbidity level (from 0 = low to 2 = high), in pandemic period (2020–2021).
Cox regression
We performed multiple regressions, progressively including additional variables and interaction terms in a stepwise approach. The model which offered the best fit of the data was selected based on the AIC criterion. The dependent variable is risk of death over age; independent variables are sex (male vs female), comorbidity level (having 1 or 2+ comorbidities vs zero comorbidities), education level (medium and high education level vs low education level). In the next sections we describe the results for these models, for the pre-pandemic and the pandemic periods; for the pandemic period we included an additional covariate for type of death (covid-related vs non covid-related).
Pre-pandemic period
Table A3 in SI shows the results of the Cox regression model applied to the pre-pandemic period; this model, which included interaction terms between all the included covariates, significantly improved the fit of the model compared to more the restricted models (those including fewer covariates and interaction terms), as indicated by the AIC statistic.
Not surprisingly, being a woman, having higher education and lower levels of comorbidity, in the pre-covid era significantly lowered the risk of death compared to men, lower education and higher comorbidity groups. The interpretation of the interaction effects, instead, is notoriously not straightforward from the regression coefficients. To ease the interpretation, we then used the command margins, available in Stata, to estimate and graph the interaction effects (results in Table A3b in SI) which are shown in Figure 3.

Predictive margins of level of comorbidities, at different combinations of sex and education level, based on Cox regression model of risk of death in the pre-pandemic period (2017–2019).
Among the individuals with no comorbidities, the category at the highest risk of death is less educated men, compared to which all the other combinations of sex and education levels, have significantly lower risk. Remarkably, lowly educated men with zero comorbidities display a higher risk than women with worse health condition (one comorbidity) at all levels of education and the same risk as highly educated men with one comorbidity. At comorbidity level 1, only men with middle and low education have higher risk of death with lowly educated men with no comorbidities. Only the individuals with two or more comorbidities (of both sexes and all levels of education) display a higher risk of death than men with low education and no comorbidity.
Pandemic period
We ran three separate analyses for the pandemic period: one with all the deaths pooled together and an additional covariate for the type of death (covid-related death vs non-covid-related), whose results are reported in Table A4 and A4b and Figure A1 in SI; one only on the non-covid-related deaths (results in Table A5 and A5b in SI and Figure 4); and one only on covid-related deaths (results in Figure A6 and A6b in SI and Figure 5).

Predictive margins of level of comorbidities, at different combinations of sex and education level for non-covid deaths, based on Cox regression model of risk of death in the pandemic period (2020–2021), non-covid deaths.

Predictive margins of level of comorbidities, at different combinations of sex and education level for covid-deaths, based Cox regression model of risk of death in the pandemic period (2020–2021), covid deaths.
In the analysis with all the deaths pooled together, adding interaction terms between type of death (covid-related vs non covid-related) and the other covariates did not improve the fit of the model. The results of the best fitting model and the estimated interaction effects from margins are reported in Table A4 and A4b in SI.
The results of the best fitting model and the predictive margins of the interaction terms for the analysis on non-covid-deaths during the pandemic are reported in Table A5 and A5b in SI. Figure 4 offers a visual representation of the interaction between comorbidity and the other covariates in the analysis, which, even though with small differences, clearly resembles the patterns and the gradients observed during the pre-pandemic period.
Finally, Figure 5 depicts the interaction between comorbidity, education and sex for covid-related deaths during the pandemic, based on the results of the best fitting Cox model (whose results are reported in Table A6 and A6b in SI). Even though the point estimates have high uncertainty, due to the small numbers of deaths from covid occurred in Denmark, an important change in the comorbidity-mortality pattern emerges. The pattern is strikingly different: the pre-existing comorbidity matters less, and all groups are more equally affected by covid-deaths. It is also important to notice how gender matters as, compared to the reference category (male, low education, healthy), women at all levels of education with 0 or 1 comorbidity had a significantly lower risk of death.
Discussion
This study provides a comprehensive population-level analysis of mortality patterns in Denmark before and during the COVID-19 pandemic, with a particular focus on how pre-existing comorbidities interacted with sociodemographic factors to shape mortality risk. Using nationwide registry data and comparing pre-pandemic (2017–2019) and pandemic (2020–2021) periods within the same population, our analysis extends beyond the hospital-centered perspective that has dominated much of the COVID-19 literature. By considering both COVID-19-related and non-COVID-19-related deaths and including the entire adult population aged 45 and older, we capture both the direct and indirect mortality impacts of the pandemic at the population level.
A first important finding is that mortality patterns for non-COVID-related deaths during the pandemic closely resembled those observed in the pre-pandemic period. As in earlier years, individuals with a greater burden of comorbidities consistently experienced higher mortality risks, and well-established gradients by sex and education largely persisted. This suggests that, overall, in Denmark, the indirect effects of the pandemic such as healthcare system strain, delayed diagnoses or treatments, and broader social disruptions, did not fundamentally alter the relationship between chronic disease burden and mortality risk from causes other than COVID-19. This finding aligns with evidence from Belgium, another high-income country with a well-developed healthcare system, where pre-existing mortality gradients associated with chronic disease burden or socioeconomic disadvantage persisted during the pandemic, and excess non-COVID deaths did not substantially alter these underlying patterns. 25 Nevertheless, we observed noteworthy shifts among specific subgroups. In particular, women with one comorbidity experienced an increase in non-COVID mortality risk during the pandemic, reaching levels comparable to those of low-educated men without comorbidities. This pattern may reflect heightened vulnerability to indirect pandemic effects among women with moderate health conditions, potentially related to disruptions in healthcare access, caregiving responsibilities, or increased psychosocial stress.
In contrast, COVID-19-related mortality displayed a markedly different pattern, representing the most novel finding of this study. At the population level, pre-existing comorbidities appeared to play a less decisive role in differentiating COVID-19 mortality risk than would be expected based on pre-pandemic mortality gradients or clinical studies focusing on hospitalized patients. Instead, COVID-19 deaths were relatively more evenly distributed across comorbidity groups, particularly among men. This suggests that, in Denmark, when the entire population is considered, including individuals who were never hospitalized, the virulence of SARS-CoV-2, combined with widespread exposure and rapid disease progression, may have attenuated the protective advantage typically associated with better baseline health, especially during the early stages of the pandemic before widespread vaccination. The absence of a clear comorbidity gradient in COVID-19 mortality at the general population level in our study contrasts with recent population-based evidence showing elevated mortality risk among individuals with chronic conditions.11,26,27 Several mechanisms may plausibly explain this discrepancy. First, during the first and second pandemic waves, mortality risk was likely driven primarily by widespread exposure to a highly virulent virus in the absence of population immunity or vaccination. Under such conditions, infection risk may dominate baseline vulnerability, thereby attenuating pre-existing mortality gradients linked to chronic disease. Second, the Danish context is characterized by a strong healthcare system and early, targeted protection of clinically vulnerable groups, which may have mitigated relative differences in COVID-19 mortality by comorbidity at the population level. Third, our observation window focuses on acute pandemic months and therefore captures direct COVID-19 lethality rather than longer-term or indirect mortality effects, which may disproportionately affect individuals with chronic conditions and emerge only over extended follow-up. Together, these factors suggest that while comorbidity increases individual-level risk, its impact on population-level mortality distributions may be context- and time-specific, particularly in the early phases of the pandemic. This interpretation warrants further investigation.
Regarding the discrepancy with findings mostly based on hospitalized populations, this is likely explained by differences in study design and population coverage. Hospital-based studies necessarily focus on patients who have already developed severe disease, where comorbidities strongly influence clinical trajectories and survival. In contrast, our population-wide approach captures mortality across all settings and stages of infection, including deaths occurring outside hospitals or shortly after infection. In this broader context, factors such as exposure risk, timing of infection relative to treatment availability, and limited immunity prior to vaccination may have reduced the relative importance of pre-existing health conditions in shaping COVID-19 mortality outcomes. Our findings therefore complement hospital-based evidence by illustrating how population-level mortality dynamics can differ from patterns observed in selected clinical samples.
Gender emerged as a robust and consistent determinant of COVID-19 mortality, with women experiencing significantly lower mortality risk than men across all educational and comorbidity groups. This finding aligns with a growing body of international evidence documenting higher COVID-19 mortality among men and supports hypotheses related to biological sex differences in immune response, hormonal influences, and inflammatory processes. Behavioral and occupational factors may also contribute to these disparities. Importantly, these gender differences persisted even when comorbidity burden was similar, indicating that comorbidities alone cannot fully explain sex-based differences in COVID-19 outcomes.
Educational differences in mortality risk also persisted during the pandemic, highlighting the continued importance of social determinants of health. Even in Denmark, where overall COVID-19 mortality was relatively low and healthcare access is universal, socioeconomic gradients were not eliminated. This underscores the relevance of factors such as occupational exposure, living conditions, and health literacy in shaping pandemic outcomes alongside medical risk factors. From a public health perspective, the relative equalization of COVID-19 mortality risk across comorbidity groups suggests that focusing exclusively on medically high-risk individuals may be insufficient during pandemics caused by highly virulent pathogens. Instead, broad population-level interventions, combined with targeted efforts to address persistent social and gender inequalities, appear essential.28,29
Study limitations
Several limitations should be considered when interpreting these findings. First, comorbidities were identified using hospital discharge registries, which may fail to capture chronic conditions managed exclusively in primary care, potentially leading to misclassification, particularly among individuals with milder disease. However, because the same data sources and definitions were applied consistently across pre-pandemic and pandemic periods, this limitation is unlikely to bias comparisons over time. Second, comorbidity burden was measured by number rather than by severity or specific disease combinations, which may obscure heterogeneous effects associated with particular conditions. Third, the relatively small number of COVID-19 deaths in Denmark limits statistical precision, especially in subgroup analyses, and warrants cautious interpretation of estimates with wide confidence intervals. Fourth, our analysis does not explicitly account for vaccination status or changes in treatment protocols over time, which may have influenced mortality patterns, particularly in later phases of the pandemic. Finally, Denmark’s comparatively low COVID-19 mortality, early uptake of strong measures and robust healthcare system may limit the generalizability of our findings to countries with different healthcare systems or pandemic trajectories.30,31
Conclusions
Using comprehensive nationwide registry data, this study provides a population-level assessment of how comorbidities, gender, and education shaped mortality risk before and during the COVID-19 pandemic in Denmark. While traditional comorbidity gradients persisted for non-COVID mortality, COVID-19 deaths exhibited a relative equalization across comorbidity groups, alongside persistent gender, and educational disparities. These findings highlight the need for pandemic preparedness and response strategies that combine protection of medically vulnerable individuals with broad population-level interventions and sustained attention to social inequalities in health. More generally, our results demonstrate the value of population-wide approaches in understanding the full mortality impact of pandemics and informing equitable public health policies.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261423654 – Supplemental material for Association between the number of comorbidities and all-cause mortality during the COVID-19 pandemic: A Danish nationwide, retrospective cohort study
Supplemental material, sj-docx-1-phj-10.1177_22799036261423654 for Association between the number of comorbidities and all-cause mortality during the COVID-19 pandemic: A Danish nationwide, retrospective cohort study by Virginia Zarulli, Cosmo Strozza and Silvia Rizzi in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036261423654 – Supplemental material for Association between the number of comorbidities and all-cause mortality during the COVID-19 pandemic: A Danish nationwide, retrospective cohort study
Supplemental material, sj-docx-2-phj-10.1177_22799036261423654 for Association between the number of comorbidities and all-cause mortality during the COVID-19 pandemic: A Danish nationwide, retrospective cohort study by Virginia Zarulli, Cosmo Strozza and Silvia Rizzi in Journal of Public Health Research
Footnotes
Acknowledgements
NA.
Ethical considerations
This study was based on fully anonymized secondary data. Therefore, ethics approval was not required.
Consent to participate
This study was based on fully anonymized secondary data. Therefore, informed consent to participate was not required.
Author contributions
VZ: Conceptualization, formal analysis, methodology, resources, software, supervision, validation, visualization, writing original draft, writing review and editing. CS: Conceptualization, data curation, resources, writing review and editing. SR: Conceptualization, funding acquisition, resources, supervision, writing review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ROCKWOOL Foundation’s Excess Death Grant (V.Z, C.S. and S.R.), and the SCOR Foundation for science through the SCOR Chair on Mortality Research 2023-2026 (C.S. and S.R.).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data of the Danish National Registries that support the findings of this study are available from Statistic Denmark but restrictions apply to the availability of these data, in accordance with the General Data Protection Regulation (GDPR), and so are not publicly available. However, programming code is available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.