
Abstract
Background:
Exploring the problems with the current supply chain management of health commodities and vital medicine procurement systems at the local level of government in federal Nepal remained the study’s main objective. More precisely, to investigate the theories surrounding the current health commodities supply chain management and the programmatic management elements of the federal government of Nepal’s local level medicine procurement systems.
Methodology:
In two randomly chosen districts of Nepal’s Bagmati and Koshi province namely Kavrepalanchowk and Sankhuwasabha districts, respectively, and at their selected six municipalities and four rural municipalities, 25 semi-structured in-depth interviews were carried out with central, provincial, district, and local health managers and service providers.
Results:
The results of verbatim transcriptions and audio video recordings of interviews were examined inductively and subsequently mapped into the four domains of “supply chain management of health commodities and essential drug procurement.”
Delays in the procurement procedure, mostly at the local level, were the main obstacles to the efficient management of essential drugs. Storage issues can provide difficulties, mostly because of a lack of available storage capacity and the requirement to manage extra emergency related comorbidities.
Conclusion:
In Nepal, ensuring access to necessary medications continues to be a difficult task. According to this study, the main reason for the difficulties in supply chain management of health commodities and essential drug procurement at district of Nepal’s is procurement delays. Challenges with supply chain management of health commodities and essential drug procurement inventory management systems at various municipalities’ levels.
Introduction
A “poly crisis” of aid cuts, fiscal restraint, and supply chain fragility revealed by the COVID-19 pandemic are some of the causes that are currently posing serious problems to the global supply chain for health commodities and key medications. As a result, procurement systems are under additional strain, underscoring the need for more robust, effective, and fair supply chains to guarantee access to high-quality, safe medications, particularly in low- and middle-income nations. Resource limitations, natural disaster-related disruptions, shortages of raw materials, and the necessity of bolstering procurement and logistics to avert drug shortages and counterfeits are important concerns.1,2
The essential drugs procurement mechanism has been criticized as inadequate in Nepal. There has also been a debate on the need for a proper system for the procurement and distribution of quality essential drugs at various levels.3–5 With this rationale, this study was conducted to analyze the present essential drugs procurement and supply chain management system in the federal governmental health system at the municipal, district, and provincial of Nepal and identify some options for its improvement. The provision of high-quality healthcare services depends on the efficient management of essential drugs procurement and it’s supply chains. Obstacles such essential drugs shortages, essential drugs stockouts, procurement procedures, and inventory management systems (IMS) continue to hinder the provision of high-quality healthcare services worldwide, primarily in low- and middle-income countries (LMIC) like Nepal.3,6
The extent of essential medicine stock-outs among municipalities and rural municipalities in Nepal (LMICs) is examined in this research, along with the causes and effects of such shortages. The causes and effects of such shortages. Medicine stockouts are not unique to Nepal as studies have documented similar problems in other LMICs.7,8 Stockouts, however, negatively affect population health outcomes. Everyday 800 women pass away because of pregnancy and child-related health problems. This can be avoided with proper administration of necessary essential medications to help prevent complications and eclampsia. Whilst existing literature point to common obstacles (challenges) across LMICs in assuring uninterrupted supply and availability of essential medications,9–13 this study aims to draw attention to the particular challenges that Nepal’s healthcare system faces. Even though there is a wealth of study in this field conducted globally, little of it focuses on Nepal, leaving a knowledge vacuum about the unique difficulties it faces. Health managers, service providers, distributors, pharmaceutical manufacturers, information service providers, regulatory bodies, and service consumers are just a few of the many stakeholders that must coordinate in the complicated healthcare supply chain. 14 Any interruptions to medical institutions’ IMS and medication supplies have a significant and immediate effect on patient care and healthcare delivery, particularly in the wake of some man-made or natural calamities. Numerous investigations on essential drugs and IMS supplies have been carried out by researchers and practitioners over the past few decades, examining their susceptibilities to systemic issues in medical facilities and crises.15–18
Nepal, which the World Bank has categorized as a lower–middle-income nation, has experienced significant political upheaval in recent years, moving toward a federal form of government.
Since provincial and municipal governments now have more responsibility to deliver high-quality healthcare as a result of this decentralization, efficient logistics management is crucial. 19 However, ensuring year-round access to essential drugs and health commodities is a constant difficulty for Nepal’s health system, especially at subnational level. This problem is made worse during public health emergencies. Despite government expenditures on distribution and procurement, persistent worries regarding the availability of the 70 critical medications and 15 medical and surgical devices provided by local health facilities are still present. These issues are regularly raised by the public and media during program evaluations. 20 The government’s objective of guaranteeing universal access to necessary medications is impacted by the multifaceted disruption in the regular supply of pharmaceutical items, including essential drugs in the public sector.21–23 Few studies have looked into what causes important product stock-outs at the service delivery point.24–27 This study offers important insights for improving pharmaceutical supply chain management in LMICs by offering a nuanced understanding of the problems unique to Nepal.
Methods
Study design and study sites
Using a qualitative research approach, this survey’s focus is on the public-sector logistics system in Nepal. The study participants are actors (or stakeholders) from all levels of the public-sector logistics system and not just those at the Ministry of Social Development (MoSD) Health Logistics Management Centre (HLMC). The HLMC is in charge of managing the distribution of medications, medical supplies and equipment.
Sampling procedure and sample size
Out of the 13 municipalities of Kavrebalanchowk district of the Bagmati province, we chose five at random: Dhulikhel municipality, Banepa municipality, Panauti municipality, Roshi rural municipality and Temal rural municipality similarly, Khandbari municipality, Chainpur municipality, Dharmadevi municipality, Silichong rural municipality, and Makalu rural municipality were selected from Sankhuwasabha district of Koshi province. The purposeful inclusion of districts having both municipality and rural municipality setups was emphasized by applying inclusion criteria to districts with rural municipality. Our goal of fully comprehending the elements under investigation is supported by this strategic approach, which guarantees a wider representation of varied situations in our study sites. Each area was chosen to have a health office.
The chief or store in charge of health offices and the store in charge of the province health logistics management center as well as the health sections at each municipality were interviewed by the researchers. Then, from each of the two districts, 10 local governments (four rural municipality and six municipalities) were chosen at random. Depending on the administrative rules of the nation, these local governments were either municipalities or rural municipalities, which mostly indicated their level of development. The chiefs of the health sections and assistant health section chiefs from each local government took part in the interviews.
To make sure the questionnaire were valid, clear, and suitable for the study, a pilot test was carried out prior to the final version. It was done at Dhadhing and Kathmandu districts of Bagamati province, Nepal.
“Twenty-five in-depth interviews were conducted to the point of thematic saturation. This sample of 25 participants also fits well with recommendations in Hennink and Kaiser, 28 and Wutich et al. 29 The list of municipal and district governments chosen for the study is displayed in Table 1.”
List of the district and local governments selected for the study.

PHLMC: Provincial Health Logistics Management Centre; MD: Management Division.
Data collection methods
Conducted in-depth interviews with staff members involved at logistics management centers at the organization’s/municipalities’ health sections, respectively. To conduct the interviews, a structured set of interview questions was developed, which covered topics such as product selection, demand-supply chain, essential drug procurement and quantification, storage and distribution, IMS, and essential drug availability. Open-ended questions were also incorporated into the interview guide to get a better understanding of participants’ perspectives on areas that needed improvement. Two public health graduates research were appointed as research assistants including two supervisors to collect data from July 20, 2022 A.D. to January 20, 2023 A.D. Some participants were interviewed over the phone and via the Zoom virtual/Google Meet platform due to their busy time schedule and unavailability at their respective duty stations.
The interviewers received training from the reach managers and stakeholders from Bagmati province’s HLMC. Over the course of the 2 days training, topics included the fundamentals of provincial-level logistic management, an introduction to data collection instruments and permission procedures, communication techniques, coordination techniques, and methods for recording and transcribing audio and video transcripts.
Data management and analysis
Initially, the audio recordings were translated into English and transcribed. In order to use the inductive analytical approach to interpret the domain, themes, and patterns, thematic analysis was conducted. After becoming acquainted with the transcripts and emphasizing the noteworthy remarks made by the research participants, codes were first determined. Prior to being organized under domains, these codes were sorted into themes. Authors R.K.S. and M.K. verified the audio recordings and the transcripts to determine the quality of the transcripts. Likewise, confirmed the codes and themes produced.
In order to guarantee the depth of the data collected, data saturation was a crucial factor in this investigation. When more data stops producing fresh insights or themes related to the study questions, it is said to be saturated. Saturation was achieved in this study using structured interviews and data was collected until recurring patterns started to appear consistently among participants. It became clear after 25 interviews and observations that no new codes or themes were emerging and that the data was supporting rather than challenging the categories that already existed.
We conducted in-depth interviews to verify saturation. The comparison of emergent themes was made possible by this iterative procedure, which also made sure that the sample size was adequate to fully address the study objectives.
Ethical approval
The Nepal Health Research Council’s Ethical Review Board provided ethical approval (reference number: 215/2022 P). The HLMC at province of Koshi and Bagamati granted administrative authority for the data collection. Prior to the interviews, the participants’ verbal and written informed consent was signed. Throughout the study, the respondents’ privacy and confidentiality were protected. The transcripts of the interviews were only available to the research team.
Results
Characteristics of study population
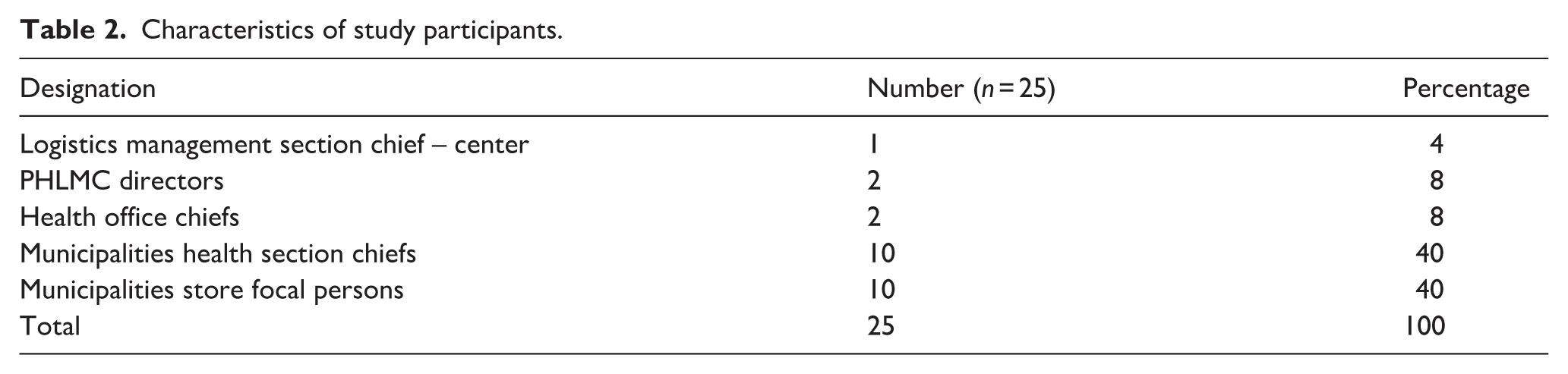
The study involved 20–50 participants, including one from logistics management section at Management Division, Kathmandu, two provincial health director, two health office chiefs, 10 health section chiefs and store focal persons from municipalities and rural municipalities. Table 2 lists the designations of involved professionals taking part in the study.
Characteristics of study participants.
Overarching domain
The four key domains identified by data analysis were:
i. Essential drugs procurement
ii. Supply chain management of health commodities
iii. Essential drugs demand and supply
iv. Management of essential drugs and health commodities during shortage
Domain 1: Essential drugs procurement
Theme 1: Procurement-related delays
All the participants thought that the procurement procedure took a long time and caused supply chain delays. Essential drugs and health commodities only arrive at municipalities in the third quarter, with the procurement administrative process beginning in the first quarter. Procurement involves many stakeholders, such as municipal governments, province hospitals, and HLMC. The process does not, however, involve health offices or health section chiefs. Although a quotation is requested for the purchase of essential drugs totaling, a tender is opened to acquire essential drugs totaling. The logistic officer and store in-charge’s quotes emphasize the difficulties in the procurement procedure.
The procurement process takes a lot of time. Therefore, we want to start the purchase process in the first quarter and start the distribution in the second. (PHLMC director, Bagmati Province) It’s a lengthy and challenging process that requires us to organize several lists. Since we are unable to contact every supplier for a quote and fee, we must call the suppliers on our roster for the medications. The supply of medications could run out at any time. (PHLMC director, Koshi Province) We are unable to regularly deliver essential drugs and health commodities for up to two or three months out of the year due to the lengthy process of obtaining medications and the delay in receiving the supply. (Health office chief, HO Sankhuwasabha)
According to the majority of health section chiefs, the local level procurement procedure was drawn out and frequently delayed. As a result, essential drugs and health commodities were in low supply at municipalities.
The municipality’s tender procedure begins very late. The municipality responded that the tender is being completed after we recently reported a shortage of essential drugs and health commodities. We ought to abide by the municipality’s decision. (Health Section Chief, Silichong rural municipality, Sankhuwasabha, Koshi Province)
Theme 2: Quality control of purchased essential drugs and health commodities
Inadequate monitoring procedures throughout the procurement process have drawn criticism, resulting in problems like the provision of low-quality or near-to-expire drugs. Findings from participant quotes shed light on the challenges of quality monitoring.
During the tender process, we frequently encounter lowered criteria for essential drugs. Medicine inventories that are almost out of date, defective goods, and even what appear to be subpar goods are provided. (Health section chief, Makalu Rural Municipality, Sankhuwasabha)
Inadequate budgetary allocations and unclear responsibilities between the provincial and local levels increase the likelihood of obtaining secondary drugs.
The shelf-life criterion is not specified in the local government level tender document. As a result, some essential drugs and health commodities may have a 12- to 14-month shelf life. (Logistic management section chief, Management division, Kathmandu)
Theme 3: Inadequate funding
Participants stated that the funds allotted were not enough to guarantee a year-round supply of essential drugs and even with the province, district, and local governments having dedicated budgets. Participants’ quotes emphasize the financial limitations.
Our budget is insufficient, and the hospital management committee is similarly short on funds. We are unable to carry out certain initiatives, like medical camps, because of a shortage of drugs. Additionally, the health office must have procurement authority. The responsibility of health offices to guarantee that essential drugs and health commodities are always available at municipalities should be reinforced. (Health office chief, Kavrepalanchowk, Bagamati Province)
Some of participants at the municipality level underlined the necessity of allocating funds to alleviate the current shortage.
For the past three months, we have been short on family planning. If sufficient funds had been timely allocated at the municipality, the shortage would have been managed. (Health section chief, Panauti Municipality, Kavrepalanchowk).
Domain 2: Supply chain management of health commodities
Theme 1: Training on supply chain management of health commodities and inventory management
e-LMIS training was found to be insufficient, and the gap was exacerbated by changes in authority and responsibility as well as resource limitations.
“We have not received e-LMIS training.” To enable local governments to buy medications independently, e-LMIS and procurement-related training are necessary in municipalities areas. (Store focal person, Health section, Dharmadevi municipality, Sankhuwasabha). We use the online system instead of doing entry in the registers. However, there is an issue with our internet and electricity back up. (Store focal person, Health section Makalu rural municipality, Sankhuwasabha)
Theme 2: Not enough room for storing
According to the majority of participants, handling necessary medications is severely hampered due to lack of enough storage space. Space in the corridor was rented or managed to solve storage issues. One major issue that compromised adherence to the first expired first out (FEFO) was a lack of storage space. This is an inventory management technique that prioritizes the sale or use of products with the earliest expiration dates. In order to minimize waste and guarantee that clients receive the freshest products. The additional supply of logistics and medications in response to health emergencies, such as the COVID-19 pandemic, landslides, earthquakes result in inadequate storage during a public health emergency.
Our storage space is inadequate. Because of this, essential drugs and health commodities are not kept according to the usual storekeeping guidelines. Newly acquired medications are displayed in front, while outdated drugs and health commodities are kept in the rear of the storage area. Therefore, the FEFO regulation is challenging to apply. Consequently, the storage is filled with piled-high expired medications. (Store focal person, Silichong rural municipality, Sankhuwasabha) We have a serious issue with the store. We are renting a room one KM away from this municipality office to keep essential drugs and health commodities safely because we don’t have enough room here at rural municipality office. It’s difficult to go and bring logistics during rainy season. (Store focal person, Temal rural municipality, Kavrepalanchowk)
Theme 3: Unskilled human resources
Due to a lack of logistic management training, most participants’ store management was subpar. An additional difficulty in handling essential drugs and health commodities and the supply chain system is the constant turnover of qualified healthcare professionals.
We lack qualified human resources for store management because of a lack of logistic management training. (Store focal person, Chainpur municipality, Sankhuwasabha)
Concerns over being overworked with several duties, such as recording and reporting and cold chain management, were voiced by the participants.
It is challenging to manage a single storeroom because it is covered in discarded rubbish. I have to operate the store, oversee the cold chain, and also serve as the recording and reporting focal point in this rular municipality; our health section lacks personnel for store management. (Store focal person, Roshi rural municipality, Kavrepalanchowk)
Domain 3: Essential drugs demand and supply
Theme 1: Demand and supply
Essential drugs and health commodities are normally requested by municipalities every month, with adjustments made in response to usage trends and supply levels.
We demand medicine if the stock lasts for only one month. The supply of medications is made monthly. (Health section chief, Dhulikhel municipality) In the event of an emergency, we request for essential drugs at any time with the reference of the threshold of emergency, though monthly demand is sent. (Health section chief, Khandbari municipality)
Theme 2: Impractical demand forecasting
The participants acknowledged that forecasting the needs for essential drugs and health commodities are based on patient flow and consumption data from prior months presented. Municipalities/rural municipalities health sections calculates essential drugs and health commodities to be purchased on the basis of morbidity data and ongoing health programs at their municipalities.
The Authorized Stock Level (ASL) and Emergency Order Point (EOP) statistics from the prior year are the primary sources of demand generation. Due to a limited supply of essential drugs, we occasionally cannot meet health facilities demands for more medication than they did the year before. Consequently, ASL and EOP meet less. (Health section chief, Dharmadevi municipality, Sankhuwasabha) Although we lack precise population statistics, we estimate the necessary quantity of essential drugs and health commodities based on program, morbidity, and population. Estimating morbidity data which is really challenging. (Health section chief, Banepa municipality, Kavrepalanchowk)
Theme 3: Carriage and transportation
Participants from hilly regions highlighted the obstacles of transporting necessary medications in inclement weather, highlighting transportation-related issues.
The areas of Kavrepalanchok district are prone to disasters, one of them is Temal rural municipality. We deal with the issue of landslides the rainy season each year. We had to carry the essential drugs and health commodities to the municipality level after traveling half of the way in the bus further carry on the backs of porters, land rover jeeps and tractors are occasionally used for carriage and transportation. During the rainy season, transporting essential drugs and health commodities are considerably more difficult. (Health section chief, Temal rural municipality, Kavrepalanchowk)
Domain 4: Management of essential drugs and health commodities during shortage
Theme 1: Shortage of essential drugs and health commodities
Municipalities close to urban areas typically avoid shortages more than those in rural areas, according to participants who reported encountering shortages to varied degrees. A shortage of necessary medications was typically not an issue for many participants who worked at municipality offices close to urban regions. Essential drugs and health commodities were, however, in low supply for rural areas or distant from the district headquarters. Most of the municipalities had a scarcity of family planning supplies last year such as amoxicillin, ciprofloxacin, and albendazole. Additionally, some individuals brought out the lack of essential drugs including metformin, ranitidine, vitamin B complex, chlorpheniramine and amlodipine at their municipalities and rural municipalities.
Our municipality is close to the city and has access to transportation; the Chainpur municipality is fully equipped to provide essential drugs and health commodities and start the procurement process when necessary. Throughout the past six months, our section has never experienced a lack of essential drugs and health commodities. (Health Section Chief, Chainpur municipality, Sankhusasabha) Due to lack of transportation and rising water levels in the river, we experience a shortage of essential drugs and health commodities throughout the rainy season. Additionally, we experience shortages at the beginning and end of the fiscal year. (Health section chief, Roshi rural municipality, Kavrepalanchowk)
Theme 2: Delay in health logistics supply delivery and financial burden to patients
Local service providers reported stock-outs of essential drugs and health commodities at the municipality levels, as well as delays and shortages in supplies from health offices.
Health office do not provide necessary medications in accordance with demand. By completing the LMIS form, we request essential drugs for three months throughout the rainy season, but they only provide a small amount that is insufficient. The primary cause of the shortage is the tardiness with which municipal offices acquire medications. Additionally, there is not enough money set up for the purchase of essential drugs. (Store focal person, Dhulikhel municipality, Kavrepalanchowk) In our municipality, people with low income, comes for the medical treatment at health facilities. When free essential drugs are not available at the health facility level, they prefer private hospitals or clinics although they cannot afford. But people cannot pay for private health services when they are impoverished. (Store focal person, Banepa municipality, Kavrepalanchowk)
Theme 3: Actions to manage shortages
Several approaches to dealing with shortages were discussed by the participants, such as working with the municipalities team (karyapalika) decision makers, borrowing medications from health office as per availability, and maintaining at least 1-month supply.
We ask the municipality office, karya palika and health office team to provide those essential drugs and health commodities, if we are short on them. (Store focal person, Panauti municipality, Kavrepalanchowk) We do maintain a month’s supply of essential drugs and health commodities before making a demand. (Store focal person, Khandbari municipality, Sankhuwasabha)
Discussion
The root causes of the shortages of essential drugs and health commodities at selected municipalities of Kavrepalanchowk and Sankhuwasabha districts in Nepal’s Bagmati and Koshi provinces were investigated in this study. Although there are several issues included in these hurdles, procurement delays stand out as the main one causing shortages of necessary medications. The use of a manual inventory management system, unrealistic demand estimation, a lack of IT resources and power backup, inadequate training on eLMIS, and lack of storage space are further obstacles. Resolving procurement delays alone will not achieve much without an efficient, simplified distribution networks that has an adequate fleet of delivery trucks running the breadth and length of Nepal. At the moment, in Nepal, the current three-tier system is still the most suitable. It strikes a balance between local accessibility, provincial supervision and central authority. Nonetheless, without lowering the number of tiers, efficiency enhancements such as enhanced eLMIS, better transport routes, and better tier-to-tier coordination could greatly boost its performance. According to the study, one of the main causes of the shortages of essential drugs and health commodities at municipalities is delays in the procurement process. We advise the provincial government to create thorough procurement guidelines and provide pertinent training for the staff members engaged to address this problem. Additionally, we support prompt demand submissions to the procurement units from service delivery locations, encouraging cooperation between PHLMC, health office, and municipalities health sections (Supplemental Material). The type of medical shortages identified in this study aligned with findings from earlier research projects in Pakistan, 30 China, 31 and Europe. 32
This alignment highlights the universality of issues in the distribution and purchase of essential drugs and health commodities, highlighting the significance of a thorough and coordinated strategy. There have been many complaints concerning subpar medications in LMICs,33–35 which frequently lead to calls for the national medicine regulators to be strengthened.
Unexpectedly, this study discovered that province-level quality control of purchased vital medications is strictly implemented, guaranteeing a minimum 18-month shelf life. Local issues, however, present difficulties since there are no explicit procurement regulations, which increases the possibility of obtaining medications that are about to expire and creating duplicate orders. These problems can be resolved by the existing governance system through efficient cooperation and communication. Participants in the study also pointed out financial limitations, citing insufficient funding for essential drugs and health commodities. To lessen this and guarantee constant availability and accessibility, we advise municipalities to set aside a specific budget for the purchase of essential drugs and health commodities. This tactic encourages better health outcomes and lessens the financial strain on people who need to buy essential drugs and health commodities from private pharmacy. The issues with inventory management, a lack of funding, and insufficient e-LMIS training, highlight the necessity of a knowledgeable workforce and technologically advanced workspaces. The lack of enough storage space and qualified human personnel was another obstacle to inventory management. Healthcare service delivery can be optimized, and efficiency increased by providing basic logistics training or training health workers in logistics management. Recognizing possible resistance, it is essential to prioritize technology-friendly environments with enough IT resources and frequent e-LMIS refresher training.30,36
Furthermore, our study results are consistent with international issues in the acquisition of essential drugs and health commodities, as demonstrated by research from Ethiopia, 37 Kenya, 38 South Africa, 39 and Uganda.40,41 Drug ineffectiveness, excessive costs, inaccessibility, and non-availability were among the obstacles noted by a study in 2013. 37 In 2016, a study highlighted how the provision of vital medicines is impacted by disorganized supply chains management, a lack of information and communication technology manipulation, and insufficient staff qualifications. 38 Procurement process delays, pharmaceutical supply chain management, staffing shortages, and insufficient finance were among the issues mentioned in studies conducted in Kenya, 11 Malawi, 42 South Africa, 39 and Uganda. 40
These findings support the obstacles found in our study, including inadequate funds, inadequate storage space, and procurement of essential drugs and health commodities delays. It is advised to prioritize a technologically friendly atmosphere at health sections in each and every municipality by offering adequate IT resources and conducting frequent e-LMIS training. According to a study done at government hospitals in Malaysia, installing electronic inventory management systems may encounter opposition because of unfavorable attitudes and ideas, which makes change challenging. 43 In order to guarantee a seamless transition to new technologies, it is imperative that appropriate change management techniques be put into place going forward. 43 The implementation of FEFO in our study environment and the efficient use of the e-LMIS system were impeded by the restricted storage space, underscoring the necessity of sufficient storage space in healthcare facilities.
Inadequate storage space could be resolved with the help of local governments’ space allocation and an evaluation of currently available space. Essential drugs should have their physical integrity preserved by properly designating and maintaining temporary storage spaces. 44 Essential drugs and health commodities management can be strengthened even more by addressing storage space shortages and putting emergency plans and other problems into account.45,46
To satisfy the needs of service users, it is imperative that vital medications and commodities be managed effectively. 47 Nonetheless, this study discovered that accurate monitoring of necessary medication supplies is hampered by local governments’ tardy reporting. Inconsistencies in the supply of important medications and commodities are a result of certain healthcare facilities’ dependence on manual records and their mistrust of computerized reporting. Strong monitoring and management systems that enable local governments to make knowledgeable decisions on distribution and procurement should be given top priority by the provincial government to address these issues.
Strengths and limitations
To sum up, our study conducted at selected municipalities and rural municipalities of Kavrepalanchowk and Sankhuwasabha districts in Nepal’s Bagmati and Koshi provinces, respectively, highlights procurement delays as a major contributing reason to shortages of essential drugs and health commodities.
This study, advances knowledge of essential drugs management during Nepal’s shifting to a federal health care delivery system. The results offer important insights for policymakers and health authorities looking to improve access to necessary supply chain management and essential drugs procurement systems at local level and varied representation of participants. It is necessary to exercise caution when extrapolating the results of this study to the national level. This study has been conducted at selected geographical locations of Nepal which are hard to reach areas but also mirror National data of supply chain management of health commodities and essential drug procurement systems at different levels of federal Nepal.
Apart from this, the study could have been conducted at additional municipalities and districts but due to limited availability of fund and resources, it was conducted at selected municipalities/rural municipalities and districts. When interpreting the study’s conclusions, these limitations should be considered.
This all-encompassing strategy is required to guarantee the efficiency of essential drugs and health commodities management in municipalities and rural municipalities of Bagmati and Koshi provinces and can act as a template for dealing with comparable issues throughout the Nation.
Conclusion
Delays in the procurement procedure, mostly at the local level, were the main obstacles to the efficient management of essential drugs. This resulted in regular shortages of these drugs, especially at the municipality level. Storage issues can provide difficulties, mostly because of a lack of available storage capacity and the requirement to manage extra emergency related comorbidities. Other issues that have been noted include a lack of information technology resources in municipalities, a lack of training on logistics management information systems, a shortage of skilled personnel to run logistics management information systems, and a lack of power backup. The intricate web of difficulties was further exacerbated by manual inventory management systems, insufficient transportation expenses, and wildly inaccurate demand estimates from the service stations.
According to this study, the main reason for the difficulties in supply chain management of health commodities and essential drug procurement at Kavrepalanchowk and Sankhuwasabha district of Nepal’s Bagamati and Koshi province is procurement delays. To solve this issue, we advise putting in place thorough procurement standards, group training, and allocated funds. This study offers profound, situational, and policy-relevant insights into the workings of health commodity supply chains in Nepal’s federal system.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261418439 – Supplemental material for Supply chain management of health commodities and essential drug procurement systems at Sankhuwasabha and Kavrepalanchowk districts of federal Nepal
Supplemental material, sj-docx-1-phj-10.1177_22799036261418439 for Supply chain management of health commodities and essential drug procurement systems at Sankhuwasabha and Kavrepalanchowk districts of federal Nepal by Rajiv Kumar Sharma, Manisha Kumari and Rajendra Baxi in Journal of Public Health Research
Footnotes
Acknowledgements
I would like to thank the Logistics Management Information System (LMIS) at Management Division (MD) Kathmandu, Provincial Health Logistics Management Centers, Health offices, and municipalities/rural municipalities for their support and taking part in this study.
Author contributions
Conceptualization: Rajiv Kumar Sharma and Dr. Rajendra Baxi. Data curation: Rajiv Kumar Sharma and Dr. Manisha Kumari. Formal analysis: Rajiv Kumar Sharma and Dr. Rajendra Baxi. Methodology: Rajiv Kumar Sharma. Project administration: Dr. Rajendra Baxi. Writing – original draft: Rajiv Kumar Sharma and Dr. Rajendra Baxi. Writing – review and editing: Rajiv Kumar Sharma, Dr. Rajendra Baxi, and Dr. Manisha Kumari.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.