
Abstract
Background:
Virological failure in second-line antiretroviral therapy (ART) occurs when HIV patients have a viral load exceeding 1000 copies/ml, presenting significant public health challenges, including increased risk of transmission of HIV, heightened morbidity and mortality rates, and the risk of developing drug resistance. The extent of virological failure among second-line ART patients in the Harari region and Dire Dawa city of Eastern Ethiopia has not been thoroughly investigated. This study aimed to determine the prevalence of virological failure and its influencing factors from January 1 to December 31, 2023.
Design and methods:
A cross-sectional study was conducted among 478 adult second-line antiretroviral therapy users at an institution-based setting. A census was employed to recruit the study participants. Data was collected using a semi-structured data extraction checklist entered into EpiData version 4.6 and exported to SPSS version 26 for analysis. Descriptive statistics, along with bivariable and multivariable logistic regression analyses, were performed to determine the associations between virological failure and independent variables, using adjusted odds ratios with 95% confidence intervals. A p-value less than 0.05 was used to declare the statistical significance.
Results:
The overall prevalence of virological failure among adult second-line ART users was 12.76% (95% CI = 10.05–16.07). Smoking (AOR = 2.81), BMI status (AOR = 6.97), TB-HIV co-infection (AOR = 0.20), history of INH prophylaxis (AOR = 4.25), and enhanced ART adherence counseling (AOR = 7.02) were found to be significantly associated with virological failure among second-line ART users.
Conclusion:
Nearly 1 in 10 adults on second-line ART experienced virological failure. Factors such as smoking, nutritional status, TB-HIV co-infection, and adherence counseling significantly influenced outcomes. Continuous monitoring and clinical interventions are crucial to reduce virological failures in this population.
Keywords
Introduction
The World Health Organization (WHO) defines HIV/AIDS treatment failure (TF) as failure in clinical, immunological, or virological treatment. 1 The most reliable and relevant way to assess the efficacy of ART is to monitor the amount of HIV RNA. This is the gold standard for identifying treatment failure in ART patients and confirms an acceptable response to treatment and sustained viral suppression.2,3 A patient on second-line (SL) ART may be determined to have virological failure when (1) they’ve been on treatment for at least 6 months and (2) they received consecutive viral load tests >1000 taken 3 months apart.1,4 It is well known that virological failure first, followed by immunological failure, and then clinical failure occurs last. 5 The WHO has recommended viral load monitoring for the detection of treatment failure and to trigger improved adherence assistance. 6
Individuals taking boosted atazanavir, the second-line medication advised by the WHO, experience equivalent virologic suppression to patients taking boosted lopinavir. 7 Current WHO guidelines recommend two NRTIs and dolutegravir as the preferred second-line regimen. 8 The gold standard criteria for HIV treatment recommendations previously recommended a second-line treatment regimen consisting of two nucleoside reverse transcriptase inhibitors (NRTIs) and a boosted protease inhibitor(PI). 1 According to the global estimate in 2016 out of 38.4 million people receiving ART more than 10% of patients were on second-line ART. 9 Every year, roughly two out of every 100 HIV patients in sub-Saharan Africa move to second-line ART. 10 In Ethiopia, patients on second-line treatment accounted for 1.5% of all patients on ART in 2019. 11
Viral failure is one of the biggest public health issues in the world affecting individuals, communities, and entire populations. 12 In the US, the pooled results for viral load suppression failure were 30% among adults receiving second-line ART, and in Africa, the viral load suppression failure was 16% among adults receiving second-line ART respectively. 13 In Ethiopia, the total treatment failure rate for HIV was 15.9%, with a virological failure rate of 6.9%. 14 The rate of virological failure was 15.4% 15 and 21% in North East and Eastern Ethiopia, respectively. 16
Virological failure of second-line ART can occur for many reasons, such as patient adherence-related factors (missed clinic appointments, high pill burden, and/or dosing frequency) and regimen-related factors (suboptimal pharmacokinetics and reduced efficacy due to prior exposure to suboptimal regimens). 17 Other contributing factors include age, not disclosing HIV status, CD4 count, opportunistic infections, and type of regimen.5,18,19 Virological failure may also result from drug resistance, toxicity, poor absorption, drug interactions, and lack of adherence. A long duration of ART, low CD4+ count, and adolescent age, past low viremia, high WHO clinical stages, and TB co-infection are associated with a higher risk of failure as well.20–23
HIV/AIDS treatment failure with antiretroviral therapy (ART) can lead to immunosuppression, opportunistic infections, resistance, and increased viral transmission. Unexplained virological failure significantly contributes to severe illnesses, such as cryptococcal disease, resulting in high morbidity and mortality in sub-Saharan Africa.24–27 To prevent virological failure among those on second-line therapy, the WHO has established guidelines aligned with the HIV care continuum, emphasizing innovative interventions, testing, ARV regimens, and monitoring. Advanced viral load measurement technologies are critical for high-risk groups, including individuals with advanced disease, infants, youths, and pregnant women.28–31
Despite efforts for early viral load testing, virological failure persists.12,16,21 To achieve 95% viral suppression among people on ART by 2030, we must prevent virological failure by improving detection of viral rebound early, improving ART adherence, and preventing opportunistic infections.20,21 Even though different evidence implied that viral load management is crucial for saving the lives of HIV patients, evidence was scarce about the virological failure of 2nd line ART and contributing factors. Thus, this study aimed to determine the extent of virological failure and associated factors among second-line ART patients in Eastern Ethiopian public hospitals of the Harari regional state and the Dire Dawa city administration.
Methods and materials
Study design and setting
The study was an institution-based cross-sectional study conducted in public hospitals in Harari Region and the Dire Dawa city administration, Eastern Ethiopia, from January 10 to February 5, 2024. Harari Regional State is located 526 km east of Addis Ababa. The Harari Region has two public hospitals: Jugal General Hospital and Hiwot Fana Comprehensive Specialized Hospital (HFCSUH). There are 45 healthcare facilities in the Harari region, including 5 hospitals, 8 health centers, and 34 health posts. Only two of the five hospitals in the Harar region are operating as public hospitals. These two hospitals currently provide different services for more than 5.8 million people in the catchment area, including ART for HIV patients. There are currently 1225 patients receiving ART at Jugal General Hospital; from these, 71 patients are on second-line ART. While there are 1897 patients receiving ART at Hiwot Fana Specialized Hospital, out of these, 114 patients are on second-line ART (Harari Regional Health Bureau). Dire Dawa is located approximately 515 km from Addis Ababa. There are two public hospitals, 15 Health centers, and 36 health posts. Dilchora Referral and Sabian General Hospitals are public hospitals located within the Dire Dawa city administration, providing various health services, including the ART service. Currently, Dilchora Hospital and Sabian Hospital serve 249 and 45 s-line ART patients, respectively (Dire Dawa Health Bureau).
Population and sampling
All records of HIV/AIDS patients who were on second-line ART for at least 6 months in HFSUH, Jugal, Dilchora, and Sabian Hospitals were included in the study. Records of patients on second-line ART who were referred from other treatment centers with incomplete information (baseline CD4 count, baseline WHO clinical stage, baseline BMI, and opportunistic infection) and transferred out to other health facilities were excluded from the study.
For the first objective, the sample size was calculated using a single population proportion formula.
Sample size determination for the second objective using different factors associated with virological failure factors among second-line ART users in public hospitals in Harar town, Eastern Ethiopia, 2023.

A census method was employed to recruit the study participants from all four hospitals (Hiwot Fana, Jugol, Dichora, and Sabiyan). Therefore, all 249 and 45 from Dilchora and Sabiya Hospitals of the Dire Dawa Administration, and 114 and 70 from Hiwot Fana and Jugal hospitals of the Harari region state, respectively, were recruited.
Data collection and quality control
A data extraction checklist was developed after reviewing the available relevant literature5,15,18,34,35 and was designed to collect information on socio-demographic, behavioral, and clinical-related characteristics. The checklist was prepared in the English language. Data was collected by four BSc-qualified nurses and supervised by one BSc public health professional. Data were collected during all working hours at the selected hospitals by using a pretested and structured checklist. First, the patient’s folders are retrieved (identified) from the hospital’s ART clinic, and then data is extracted from the patients’ case files using the pre-prepared checklist.
Two days of training were given to the data collectors and supervisor on the purpose of the study, the data collection tool, data collection methods, the process of assigning and selecting the study participants, and ethical considerations during data collection. A pre-test was conducted on 5% of the sample size in Haramaya Hospital before the actual data collection. The supervisor monitors the completeness and consistency of the collected data along with the principal investigator on a daily basis at the spot during the data collection time. The possible errors were returned to the collectors for correction. Double data entry was done by two data clerks, and the consistency of the entered data was cross-checked by comparing the two separately entered data on Epidata.
Operational definitions
Second-line ART virological failure
Assessed by measuring viral load results > 1000 copies/mL after 6 months were switched to second-line ART in two subsequent measurements at least 3 months apart. 36
Adherence
Assessed by the patient’s self-report about missed doses within a month, missing more than three doses from BID doses, and missing more than one dose from daily doses was considered poor adherence. 36
Opportunistic infections
Infections that develop because of HIV-inflicted damage to the immune system (TB, PCP, gastrointestinal OI, herpes simplex, herpes zoster, fungal infection), and other national ART guidelines define opportunistic infection. 37
Substance use
It is defined as persons reporting smoking, chewing tobacco, and shisha in the last 30 days. 37
Alcohol consumption
To measure alcohol consumption, we used a question on the history and frequent using alcohol use among the respondents. 38 It was responded to with yes and no questions.
Data processing and analysis
Data was checked for completeness, coded, and entered into Epi Data 4.6 software. After cleaning for inconsistencies, it was exported to SPSS version 26 for analysis. Descriptive analysis was conducted, with results displayed in tables and graphs. A bivariate logistic regression assessed relationships between the dependent and independent variables, considering those with p-values <0.25 for multivariate logistic regression to control for confounders and identify predictors of virological failure. Multicollinearity was checked; variables with a standard error (SE) ≥ 2 were excluded. Model fitness was tested using Hosmer–Lemeshow’s goodness-of-fit. Adjusted odds ratios (AORs) with 95% confidence intervals evaluated associations, with p < 0.05 indicating statistical significance.
Results
Socio-demographic characteristics of the study participants
A total of 478 records of adults on second-line ART were retrieved (100%). About half of 247 (51.7%) second-line ART users were in the age range from 30 to 45 years old, with a mean age of 38.79 (SD ± 11.39). More than half of 278 (58.2%) study participants were females, and about 263 (55.0%) of them were Orthodox religion followers. The majority, 403 (84.3%), of second-line ART users were urban residents, and about half of the 252 (52.7%) of study participants were married. More than half, 266 (55.6%), of them were self-employed, and 286 (59.8%) of their educational status were in primary school (Table 2).
Socio-demographic characteristics of adults who are second-line ART users in public hospitals in Harar regions and Dire Dawa city administration, Eastern Ethiopia, 2024.

Behavioral, clinical, and nutrition-related characteristics
Of the 478 study participants, 392 (82.0%) disclosed their HIV status, and 426 (89.1%) were non-smokers. Most participants, 450 (94.1%), had no history of alcohol use, while 361 (75.5%) reported chewing khat. Almost all, 469 (98.1%), did not use drugs (Table 3).
Behavioral and disclosure-related characteristics among adults on second-line ART in public hospitals in the Harar region and Dire Dawa Administration, Eastern Ethiopia, 2024.

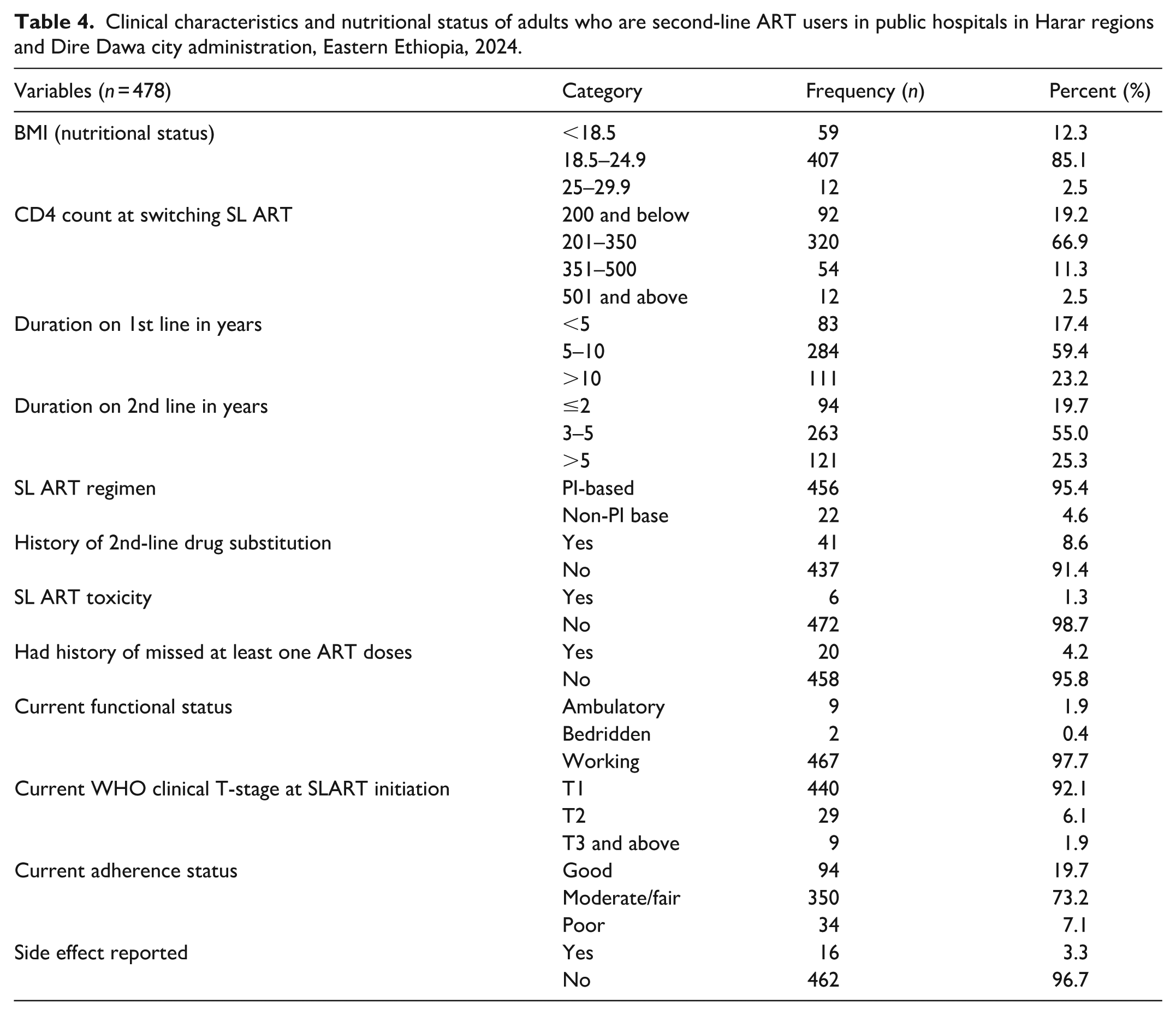
Regarding health metrics, 407 (85.1%) had a normal BMI (18.5 to 24.9), and 320 (66.9%) had a CD4 count between 201 and 350 when switching to second-line ART. More than half, 284 (58.4%), had been on first-line ART for 5–10 years, and 263 (55.0%) were on second-line therapy at the time of data extraction. Most second-line users, 456 (95.4%), were on PI-based regimens, with only 41 (8.6%) requiring drug substitution. About 20 (4.2%) missed doses of their second-line ART. Additionally, 440 (92.1%) were in T1 WHO clinical stage at ART initiation, while 73.2% had moderate drug adherence, and only 16 (3.3%) experienced side effects (Table 4).
Clinical characteristics and nutritional status of adults who are second-line ART users in public hospitals in Harar regions and Dire Dawa city administration, Eastern Ethiopia, 2024.
Health condition and service-provided-related characteristics
Almost all second-line ART users, 471 (98.1%), had negative TB screening reports, while 12 (2.5%) experienced TB/HIV co-infection during the switch. A majority, 456 (95.6%), had a history of taking isoniazid (INH) prophylaxis, and 58 (12.1%) reported opportunistic infections. Most participants, 466 (97.5%), received enhanced adherence counseling (EAC), with about half, 224 (48.0%), receiving counseling 3–4 times. More than half, 321 (67.2%), demonstrated good adherence to cotrimoxazole (Table 5). Regarding the reasons for switching to second-line ART, virological failure accounted for 65.9%, while both immunological and virological failure together accounted for 24.7% (Figure 1).
Health condition and service-provided-related factors of adults who are second-line ART users in public hospitals in Harar regions and Dire Dawa Administration, Eastern Ethiopia, 2024.


The reason for switching to the second-line ART drugs of adult people on second-line ART in public hospitals in the Harar region and Dire Dawa Administration, Eastern Ethiopia, 2024.
Overall, the study found that the rate of virological failure among adult second-line ART users was 12.76% (95% CI: 10.05–16.07).
Factors associated with virological failure among adult second-line ART users of adults
In the bivariable analysis, variables such as sex, residence, level of education, smoking, chat chewing, BMI (nutritional status), duration on second-line ART, missed second-line ART in the past 7 days, ART drug adherence status, TB-HIV co-infection, history of taking INH prophylaxis, and history of enhanced ART adherence counseling were significantly associated with virological failure at a p-value <0.25 and were a candidate for multivariable binary logistic regression analysis. However, in the final model of the multivariable logistic regression analysis, smoking, BMI (nutritional status), TB-HIV coinfection, history of taking INH prophylaxis, and history of enhanced ART adherence counseling were found to be significantly associated with virological failure at a p-value <0.05 among second-line ART users of adults.
Accordingly, the study revealed that second-line ART users who had smoked cigarettes were 2.81 times more likely to have virological failure compared to those who had not smoked cigarettes (AOR = 2.81, 95% CI = 1.06–7.42). Similarly, second-line ART users whose BMI status was 25.0 to 29.9 (overweight) were 6.97 times more likely to have virological failure compared to those whose BMI was 18.5 to 24.5 (normal; AOR = 6.97, 95% CI = 1.96–24.86). In addition, adults who were second-line ART users and who had no history of taking INH prophylaxis were 4.25 times more likely to have virological failure compared to their counterparts (AOR = 4.25, 95% CI = 1.36–13.33). Further, adults who were second-line ART users and who had no history of enhanced ART adherence counseling were 7.02 times more likely to have virological failure compared to those who had a history of enhanced ART adherence counseling (AOR = 7.02, 95% CI = 1.70–29.00). Likewise, second-line ART users with no TB/HIV coinfection were 80% less likely to have virological failure than those with a TB/HIV coinfection (AOR = 0.20, 95% CI = 0.05–0.83; Table 6).
Factors associated with virological failure among second-line ART users in public hospitals in Harari regional state town and Dire Dawa Administration, Eastern Ethiopia, 2024.

Significant at p < 0.05.
Discussion
According to this study, the overall magnitude of virological failure among adult second-line ART users was 12.76% with a 95% CI: (10.05–16.07). This result was comparable with study findings that showed that the magnitude of virological failure was 11.0% in Jimma, Ethiopia, 39 in Debre Markos, northwest Ethiopia, was 10.5%, 37 in northwestern Tanzania showed that virological failure was 12.18% 40 and a study conducted in Nepal showed that the virological failure was 11.34%. 41 On the other hand, our study was lower than the study conducted in Cameroon, which showed that the second-line virological failure was 20.6%, 42 but lower than the study conducted in Pune, India showed that 15.0%. 19 This difference may be due to sociodemographic differences and the time of study when some treatment strategies were modified, which directly resulted in lower virological failure in our study area.
Accordingly, the study revealed that second-line ART users who had smoked cigarettes were more likely to have virological failure compared to those who had not smoked cigarettes. This finding is in line with similar studies conducted indicating the significant impact of smoking on the effectiveness of HIV treatment in which the second-line antiretroviral therapy (ART) users who smoked cigarettes were indeed more likely to experience virological failure compared to non-smokers 43 and another finding indicated that smoking had a direct impact on increasing virological failure among ART users. 44 This is explicitly related to the fact that smoking is a serious health threat for everyone, but it’s especially dangerous for people living with HIV. 45 People with HIV who smoke are more likely to develop infections, which also lead to a poorer response to antiretroviral therapy and increase the risk of cardiovascular diseases, which increases the probability of virological failure among ART users. 46
The study also revealed that second-line ART users whose BMI status was overweight were more likely to have virological failure compared to those whose BMI was normal. Our finding is supported by different findings indicating overweight has a significant effect on the virological load among people who are using ART.47,48 One possible explanation may be that overweight individuals may experience altered drug absorption and metabolism, which can affect the efficacy of ART, which directly results in virological failure. Overweight individuals might face additional health challenges such as diabetes, cardiovascular disease, and cancer that can complicate adherence to ART; then when adherence is poor, the probability of virological failure is expected. 49 In addition, excess weight can lead individuals to chronic inflammation, which might impact the immune response, and as the immune response of ART users is impacted, the reproduction of various would be increased; then, the effectiveness of ART would be low, directly resulting in virological failure. 50
In addition, adults who were second-line ART users and who had no history of taking INH prophylaxis were more likely to have virological failure. This finding is in line with studies that found taking INH prophylaxis has been associated with reducing virological failure.5,51 This finding is also supported by other findings indicating that taking isoniazid (INH) prophylaxis has been shown to have a positive impact on reducing virological failure among individuals on antiretroviral therapy (ART). 52 This may be explained by the fact that INH prophylaxis is primarily used to prevent tuberculosis (TB) in people living with HIV, but it also appears to support better virological outcomes by reducing the incidence of opportunistic infections like TB, which can complicate HIV treatment.
Further, adults who were second-line ART users and who had no history of enhanced ART adherence counseling were more likely to have virological failure compared to those who had a history of enhanced ART adherence counseling. This finding is in line with similar studies conducted in different settings that showed that counseling on enhanced ART adherence has a significant effect on reducing virological failure.53–55 The possible explanation is that having strategies of providing tailored advice can help individuals to overcome specific barriers to adherence, such as forgetfulness, side effects, or stigma; also, it educates patients about the importance of strict adherence to ART, helping them understand how missing doses can lead to drug resistance and virological failure. 56
Finally, second-line ART users with no TBHIV coinfection were less likely to have virological failure than those with a TBHIV coinfection. This finding is in line with similar studies conducted in various places that showed that TB/HIV coinfection can significantly contribute to virological failure among individuals on antiretroviral therapy (ART).5,33,53,54 This is explicitly related to the fact that TB/HIV coinfection causes weakening of the immune system, making it harder for the body to fight off TB. This dual burden can lead to a higher viral load and reduced effectiveness of ART. 5 The medications used to treat TB can interact with ART drugs, reducing their effectiveness. Managing both TB and HIV requires taking multiple medications, which can be overwhelming and lead to poor adherence, and the combination of TB and HIV medications can cause significant side effects, which may lead patients to skip doses or stop treatment altogether; those are all major factors in virological failure.22,57
This study is not without limitations. Limitations such as the secondary nature of the data, which may lack detailed patient-level information, and the cross-sectional nature, which limits the ability to establish causal relationships between factors and virological failure, should be considered. Future research should focus on longitudinal studies to better understand the relationships between these factors and virological failure, as well as explore the generalizability of the findings across different healthcare settings.
Conclusion
The findings from this study indicated that nearly 1 out of 10 virological failures happened among adult second-line ART users in the study area. Factors such as smoking, BMI (nutritional status), TB-HIV co-infection, history of taking INH prophylaxis, and history of enhanced ART adherence counseling were found to be significantly associated with virological failure among second-line ART users of adults. Based on the findings of this study, targeted interventions to address modifiable risk factors, such as smoking cessation, regular physical exercises, regular screening for TB-HIV co-infection, and focusing on adherence to completion of INH among ART users to improve treatment outcomes, are recommended.
Footnotes
Acknowledgements
We would like to extend our heartfelt gratitude to Haramaya University, College of Health and Medical Sciences, for providing us the opportunity to conduct this research. We deeply appreciate the cooperation and support of all stakeholders in facilitating data collection.
Ethical Considerations
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences, Haramaya University, with reference number of IHRERC/017/2024. Official letters were written to respective health facilities. The hospital unit was informed about the purpose of the study and the risks and benefits of the study. Informed, voluntary, written, and signed consent was obtained from the hospital administrators before the data collection. The hospital administrators were also informed that information obtained from patients’ medical records and registration books was treated with complete confidentiality.
Author Contributions
LM conceived the idea, analyzed the data, and drafted the manuscript. LM, KM, AD, DF, and SL contributed to data analysis, writing, and editing the manuscript. Finally, all the authors read and approved the final version and agreed on all aspects of this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Haramaya University as part of a master’s thesis project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.