
Abstract
Artificial intelligence (AI)-enhanced ultraportable X-ray machines have been recently introduced in our region as tools for community-based pulmonary tuberculosis (TB) screening. Compared to the previously used method of relying solely on “any symptoms of tuberculosis,” chest X-ray screening is a more efficient and practical approach. Subclinical TB cases, who often lack overt clinical symptoms, may still be infectious and can present with radiographic abnormalities detectable on chest X-rays. Therefore, a parallel screening strategy combining chest X-rays and symptom assessment, followed by confirmatory sputum testing, is effective in detecting both clinical and subclinical TB cases (with X-ray abnormalities) within the community. The integration of this algorithm, along with AI-assisted portable X-ray devices, represents a significant advancement in community TB screening, although some limitations remain.
Introduction
Chest X-ray is a highly sensitive screening tool for detecting people who require diagnostic testing for pulmonary TB and can guide the effective allocation of molecular WHO-recommended rapid diagnostic tests (GeneXpert). 1 In past years, chest radiography (CXR) has played a significant role in detecting pulmonary tuberculosis (TB) primarily in hospital settings. However, the development of ultraportable X-ray machines has enabled its use as a screening tool in community health camps. Where the World Health Organization (WHO) has set an ambitious target to end the global TB epidemic by 2030, active case finding is expected to play a major role. 2 The current WHO guidelines recommend the integration of CXR into screening and triaging algorithms. 3 Furthermore, the incorporation of artificial intelligence (AI) software as an image analyzer is reported to enhance disease predictability and reduce human error. 4 The Nepal Tuberculosis Control Center, the central body for surveillance of tuberculosis in Nepal, has recently endorsed CAD4TB (computer-aided diagnosis for TB), an artificial intelligence software integrated with an ultraportable X-ray modality for community screening of tuberculosis. CAD4TB is an AI-powered software modality that works online (CAD4TBcloud) and offline (CAD4TBbox). The setup can be made in two rooms without requiring much space or sophisticated connections and can be set up and run by a trained doctor and a radiographer (Figure 1). The X-ray tube can take high-resolution images and has been claimed to have low scattering and minimal radiation doses. 5 The X-ray tube system sends a DICOM image to the offline local CAD4TB server (CAD4TBbox). The CAD4TB box interprets the X-ray image and provides the following results in less than 5 s: an abnormality score (0–100) for the chest lesions, a heatmap of the lesion, and binary classification of “possible TB” or “no TB.” In our setting, we use parallel screening with any TB symptom (cough, fever, night sweats, or weight loss) and chest X-ray. Suspected cases are directed for spot sputum sample collection for GeneXpert. With this algorithm, we have experience performing approximately 200–250 readings per day by a doctor effectively. However, integrating this technology into remote healthcare settings comes with both opportunities and challenges. With an experience of 19 screening programs in underserved regions of Nepal, we put forward the benefits and challenges of AI-enhanced ultraportable X-ray modality in rural Nepal from a clinician’s viewpoint.
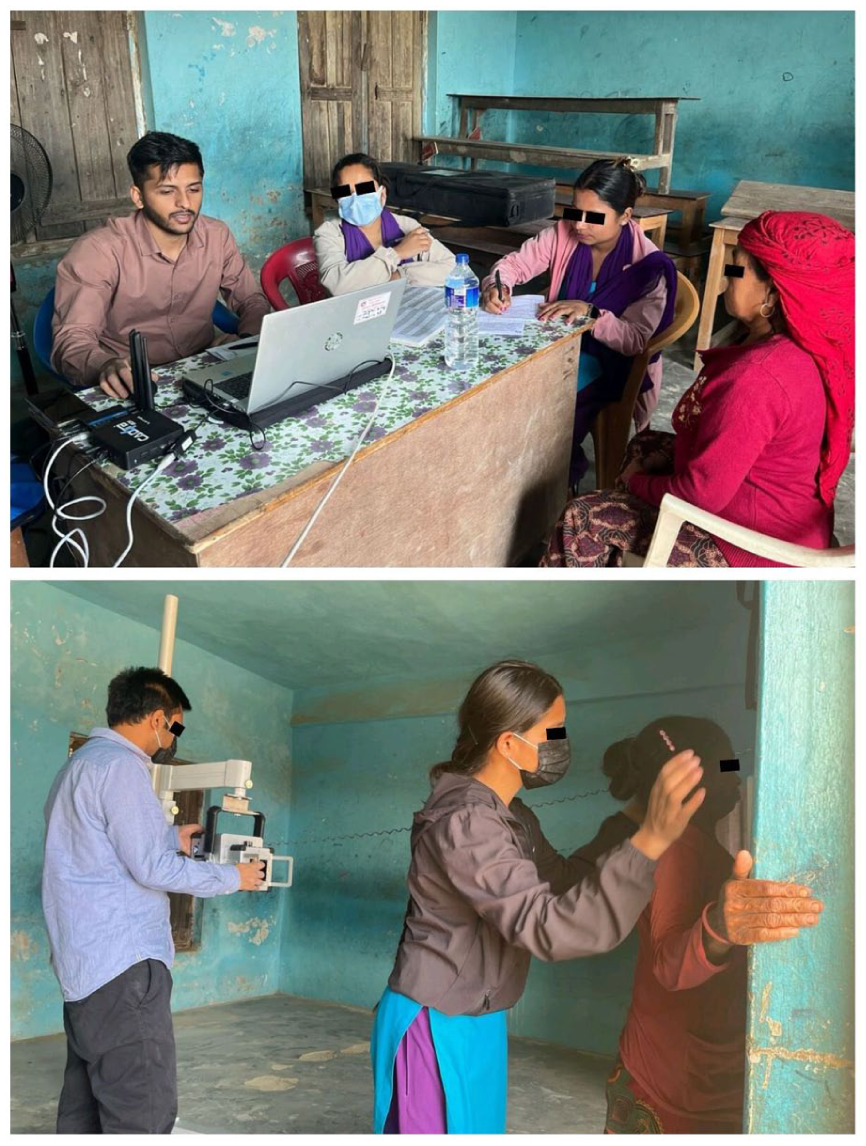
The X-ray setup made in two rooms using minimal local resources.
Benefits of the current technology
Increased efficiency of screening programs
Before community X-ray screening, the screening algorithm used in our context was the “any symptom” screen test, in which community health workers visit dwellings, ask for symptoms suggestive of pulmonary TB, and request a sputum test (microscopy and/or GeneXpert) if any symptoms are suggestive. In a context such as Nepal, where the TB prevalence is estimated to be 0.5%, its sensitivity is 60%, and its positive predictive value is 29.4%. 3 With the advent of AI-enhanced portable X-rays for community screening, the WHO suggests that the use of an algorithm incorporating CXR with TB symptom screening (parallel screening or sequential negative serial screening) is the most suitable for TB screening because of its high detection rate (sensitivity: 85%), excellent negative predictive value (99.9%), and considerable PPV (56.7%), making it effective for public health use. 3 Symptom-based referral to sputum testing leads to a greater number of GeneXpert tests, which itself is a cost burden to the government, and X-ray with symptom screening is evidence-based and rational. Triaging with chest X-ray before allocating sputum GeneXpert yield significantly lower number need to screen compared to symptoms based molecular testing. 1 In settings with high TB prevalence, triage using chest X-ray helps limit unnecessary use of GeneXpert testing, thereby easing resource strain. Use of AI-enhanced X ray triaging modality can reduce operational costs by up to 37% and is projected to avert nearly 4% of disability-adjusted life years (DALYs). 6
Detection of subclinical tuberculosis
Subclinical TB is a disease caused by viable M. tuberculosis bacteria that do not cause clinical TB-related symptoms but cause other abnormalities that can be detected by existing radiologic or microbiological assays. 7 Subclinical TB might be an important source of transmission for TB in the community.7,8 Where symptom-based screening is not applicable for active cases of this subset, chest X-rays can detect radiological abnormalities suggestive of TB in these cases.1,3 When Nepal aims to end the TB epidemic by 2035 and eliminate TB by 2050, the detection of subclinical tuberculosis and its management are important aspects to address. 9
Enhanced human productivity
Interpreting hundreds of chest X-rays and correlating them with symptoms in a day is a fatiguing task. During week-long screening programs, human errors such as “slips” can prevail. AI software, particularly heatmap technology (Figure 2), can prevent us from overlooking subtle chest lesions and missed diagnoses. CAD software has been shown to have comparable accuracy to humans in reading TB lesions on chest X-ray. The WHO has suggested that CAD software has potential to replace human readers and has now recommended it as an alternative to human reading. In a WHO estimate, TB screening using AI software has demonstrated sensitivity ranging from 85% to 94% and specificity from 42% to 80%, which is comparable to human readers who show sensitivity of 82%–93% and specificity of 14%–63%.3,10 Thus, screening algorithms with incorporated human and AI reading may further enhance productivity and reduce errors. 11 At the same time, AI rapidly flags abnormalities, allowing physicians to focus more on patient interaction and counseling. “In the future,” it may also enable task shifting like empowering junior staff to triage routine cases under AI guidance.

The software interface with a chest X-ray with and without heat map of the lesions.
Parallel workflow and reduced workload
In rural screening camps, the daily workload for a doctor can be overwhelming, often requiring the review of 200–250 (and sometimes more) chest radiographs in addition to patient counseling, documentation, and coordination of sputum collection. Such volume inevitably leads to decision fatigue. With AI assistance, the workflow shifts substantially: the radiographer acquires the image, the AI rapidly flags potential abnormalities with heatmap, and the clinician can either independently analyze the image or cautiously validate the AI’s output. This parallel approach facilitates task shifting and streamlined triage, allowing clinicians to focus on nuanced judgments and patient counseling. Importantly, it reduces the time spent on monotonous image interpretation and reallocates physician effort toward patient engagement and supervision.
Solved operational difficulties
Earlier, the use of chest X-rays for active case screening was limited by logistic challenges. The development of ultraportable and light X-ray machine setups has made the use of X-rays for camp screening possible. These instrument sets are lightweight and can be easily carried by two people. Furthermore, the development of AI-engaged diagnostic software has further aided CXR interpretation and reduced human error.
Reduced dependence on traditional infrastructure
Portable X-ray systems require less physical space and infrastructure than conventional units do. This is particularly beneficial for rural health posts and mobile health camps, where space and infrastructures are limited.
Challenges with the current technology
High initial cost and sustainability concerns
The cost of acquiring and maintaining AI-powered X-ray units is high. In our country, health camps operate on limited budgets, raising concerns about financial sustainability, maintenance, and long-term operational support.
Logistic issues
Although ultraportable X-ray systems have significantly reduced the burden of heavy logistics, transportation challenges still persist, especially in regions with poor road access, monsoon-related disruptions, or where porters are required to reach remote health posts (Figure 3). Carrying and coordinating these multiple sensitive devices requires proper planning, secure packaging, and, often, manual porters.

The damaged road due to a landslide and human porters being awaited.
Unique technology and system fragility
The setup involves a unique combination of integrated devices (X-ray generator, AI software, battery packs, tablets, and connectivity tools). Failure of even a single component can bring an entire camp or screening session to a halt. This fragility limits its reliability in high-volume or rugged field conditions.
Weak referral linkage & continuity of care and follow up
Even after a presumptive TB case is identified via X-ray, ensuring that it reaches a diagnostic center for confirmation (e.g. “repeated” GeneXpert testing, bronchoalveolar lavage, or CT scan) is a major challenge in rural settings. Geographic and financial barriers can lead to significant dropouts. Rural health systems often lack digital tools to track screened patients, especially those needing follow-up. Without proper linkage, many patients are lost to follow-up after initial screening. This challenge is not specific to chest X-ray–based screening; symptom-based sputum screening is likewise constrained by weak referral systems. Delays in accessing confirmatory tests or starting treatment can result in ongoing transmission and worsening of disease. Efficient linkage-to-care systems are crucial but currently underdeveloped.
Radiation risk
In facilities with proper radiation protection (lead shielding, operator booths), the occupational risk for health workers remains very low, even with 200–300 exposures daily. However, in community-based or mobile screening programs, such infrastructure is often lacking. This can increase closeness to the radiation source and scatter exposure, the risk profile. Strict adherence to safety measures like increasing distance from the X-ray source, shielding, and reducing time in the field is essential to reduce risks of health hazards.5,12
Shortcomings of the current technology
Extra-pulmonary TB
This newer screening tool still does not provide a clue about extra-pulmonary tuberculosis.
AI algorithm bias and validation
AI models are trained on datasets that may not fully represent the Nepali population. Currently, we do not have an established cut-off value or threshold value for determining when to suspect tuberculosis. Additionally, it cannot perfectly distinguish an active lesion from old fibrosis/calcification or the artifactual appearance of opacification (due to improper inspiration, positioning, or exposure). Similarly, AI software tends to misclassify other pulmonary diseases (pneumonia, tumor) as tuberculosis. 13 This can lead to diagnostic inaccuracies, particularly in conditions where subtle variations exist. Some clinicians express skepticism about delegating image interpretation to AI, but it can be accepted for now as a supportive tool rather than a replacement.
Conclusion
Although a chest X-ray is not a diagnostic test for tuberculosis, screening with CXR in people irrespective of TB-related symptoms is a better mass screening modality in TB-endemic regions because of its superior productivity than earlier screening tools. Thus, portable X-ray systems can transform TB detection and treatment in rural regions. They offer a practical solution to bridge the gap between underserved populations and quality diagnostics. Furthermore, artificial intelligence and heatmap technology reduce human error (“slips”) and increase productivity. AI rapidly flags abnormalities, allowing physicians to focus more on patient interaction and complex cases. However, physicians must balance reliance on AI with their own clinical judgment and ultimate diagnostic responsibility. From a doctor’s perspective, these tools are welcome innovations. However, sustainable implementation requires more than just deploying the technology; it demands investment in infrastructure and patient follow-up systems.
Footnotes
Authors contribution
Ravi Shukla: Conceptualization, methodology, resources, writing & editing.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article, as no new data were created or analyzed in this study.