
Abstract
Background:
Musculoskeletal disorders are often given lower priority and receive little attention in developing countries especially in Ethiopia. Despite extensive research on MSDs, there is no comprehensive evidence in Ethiopia on the magnitude of musculoskeletal disorders. Thus, this study aimed to determine the prevalence and associated factors of musculoskeletal disorders among patients with DM in Ethiopia.
Methods:
The study was conducted in accordance with the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. The articles were searched using electronic databases including PubMed, Science Direct, and African Journals Online from October 1 to March 30, 2025. The authors carried out data extraction using a standardized form created in MS Excel.
Results:
Eight studies were included in this systematic review and meta-analysis study. The study showed that the pooled prevalence of musculoskeletal disorders among patients with diabetes mellitus in Ethiopia is 27.79% (95% CI: 21.90−33.68, I2 = 59.7%). Being female (OR = 1.85, 95% CI: 1.35−2.55, I2 = 0.0%), rural residence(OR = 1.89, 95% CI: 1.21−2.95, I2 = 46.1), age > 50 years (OR = 6.55, 95% CI: 1.23 −34.98, I2 = 93.9%), hypertension(OR = 4.85, 95% CI 2.59−9.08, I2 = 73.6%) and DM duration ≥ 10 years (OR = 9.41, 95% CI: 1.04−85.08, I2 = 94.9%) were associated factors of musculoskeletal disorders.
Conclusions:
Musculoskeletal disorders are highly prevalent among patients with diabetes in Ethiopia, particularly among older adults, those with long-standing diabetes, and individuals with comorbid conditions such as hypertension. These findings underscore the need for targeted screening and early intervention programs for high-risk groups.
Prospero registration number:
CRD42024580332.
Background
Diabetes mellitus (DM) is a long-term endocrine disease characterized by persistent high blood glucose level. This chronic hyperglycemia can result in significant health problems and increased risk of death due to complications affecting both small and large blood vessels. 1 The International Diabetes Federation (IDF) estimated that 24 million adults in Africa were living with diabetes in 2021. By 2045, DM cases in Africa are projected to increase by 129%, rising from 24 million to an estimated 55 million, which poses a significant public health challenge. 2 Chronic hyperglycemia can damage nerves and blood vessels throughout the body, increasing the risk of severe health problems such as heart disease, stroke, kidney failure, blindness, and musculoskeletal disorders. 3
Musculoskeletal disorders (MSDs) are common disorders that affect different parts of the musculoskeletal system. 4 DM is a metabolic disorder that increases the risk of musculoskeletal problems in joints, bones, soft tissues, and surrounding structures.5,6 Musculoskeletal disorders are the primary cause of activity limitations, functional loss, and long-term disability. They lead to fatigue, which can result in early retirement, as well as pain and joint deformities. 7
Globally, the focus of disease burden is shifting from communicable diseases to chronic non-communicable diseases (NCDs), which often encompass MSDs. 8 While the underlying pathophysiological mechanisms are not fully understood, DM can result in a range of musculoskeletal complications.9–11 It leads to chronic, irreversible damage and harmful effect in musculoskeletal and connective tissues. 11 Evidences indicates that hyperglycemia might speed up non-enzymatic glycosylation and abnormal collagen buildup in the connective tissues around joints. This can further disrupt the structural matrix and mechanical properties of the musculoskeletal system. 12 Disorders of connective tissues, neuropathy, and both micro-vascular and macro-vascular complications may collectively contribute to the onset of musculoskeletal disorders. 6 The most frequently identified and researched musculoskeletal complications affecting the shoulder and hand include frozen shoulder, restricted joint mobility, trigger finger, Dupuytren’s contracture, and carpal tunnel syndrome. 13
DM often leads to various problems affecting the skeletal and muscular systems. 6 Musculoskeletal complications of DM are often inadequately addressed compared to other complications. As the prevalence and incidence of DM rise, the proportion of patients with DM experiencing functional disability is also expected to grow, posing a significant public health challenge. 14 The 2016 Global Burden of Disease report identified MSDs as a major contributor to disability-adjusted life years, highlighting their significant economic impact, high healthcare utilization, and associated social problems.15–17
MSDs are often given lower priority and receive little attention in developing countries especially in Ethiopia. 18 Despite extensive research on MSDs, there is no comprehensive evidence in Ethiopia on the magnitude of musculoskeletal disorders. Thus, this study aimed to determine the prevalence and associated factors of MSDs among patients with DM in Ethiopia. Effective prevention of MSDs, injuries, and disabilities requires evidence-based strategies to identify and implement better measures. The results of this study will be crucial for policymakers and health program managers to design appropriate interventions for musculoskeletal disorders among diabetic patients in Ethiopia.
Material and methods
Protocol design and registration
The study was conducted in accordance with the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-2020) 19 (Supplemental File 1). The systematic review was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO) and given the reference number CRD42024580332.
Inclusion criteria
(1)
(2)
(3)
(4)
Exclusion criteria
Articles were excluded if they lacked data on the prevalence of MSDs among patients with diabetes. Additionally, articles that did not report odds ratios (OR) or binary outcome measures related to the factors associated with MSDs and/or prevalence were excluded. Furthermore, studies that were not fully accessible, qualitative studies, case series, and reports were excluded in the review.
Data sources and searching strategy
Two authors (WCT and YAF) searched electronic databases including PubMed, Science Direct, and African Journals Online to retrieve published articles from October 1 to March 30, 2025. Google Scholar was also searched to find additional relevant studies. We used both MeSH terms and free-text keywords such as ‘musculoskeletal diseases’, ‘arthritis’, ‘back pain’, ‘osteoarthritis’, ‘tendinitis’, ‘myalgia’, ‘soft tissue injuries’, ‘rheumatic diseases’, ‘diabetes mellitus’ (including Type 1 and Type 2), ‘hyperglycemia’, as well as terms like ‘determinants’, ‘associated factors’, ‘predictors’, and ‘adults’. Boolean operators ‘AND’ and ‘OR’ were applied to construct search strings across the databases. Two authors (WCT and YAF) independently screened titles, abstracts, and full texts. Search results were managed using EndNote X7, and full-text articles were thoroughly reviewed to confirm eligibility.
Study selection
All articles identified in the search were imported into EndNote X7 software (Thomson Reuters, New York, NY), where duplicates were removed. Two authors (WCT and YAF) then assessed the titles of the remaining articles and excluded articles that did not meet the inclusion criteria. Before data extraction, the full texts of the selected articles were retrieved and thoroughly reviewed to ensure they fulfilled the eligibility criteria. The analysis included only those studies that met the inclusion criteria.
Data extraction and quality assessment
Two authors (WCT and YAF) carried out data extraction using a standardized form created in MS Excel. The data extraction form included information such as the primary author’s name, publication year, region, outcome diagnostic method, response rate, sample size, and the prevalence of MSDs. Any disagreements between the two authors were resolved through discussion. Furthermore, the authors (WCT and YAF) assessed the quality of the included studies using the Johanna Briggs Institute (JBI) quality assessment checklist which is freely available at https://synthesismanual.jbi.global. The checklist consists of eight components, with each question rated as 0 (not reported or inadequate) or 1 (yes), giving a total score range of 0 to 8. Studies were then classified as low quality (0–4), medium quality (4–5), or high quality (6–8) based on their total score. 20
Measurement of outcome
The main objective of this systematic review and meta-analysis was to determine the pooled prevalence of MSDs among patients with diabetes mellitus in Ethiopia. MSDs (including carpal tunnel syndrome, Dupuytren’s contracture, limited joint mobility, stenosing tenosynovitis, adhesive capsulitis, reflex sympathetic dystrophy, diabetic amyotrophy, diffuse idiopathic skeletal hyperostosis syndrome, and Charcot joint) in the primary studies were assessed by physiotherapists using the participants’ medical history, records, and standardized physical examinations. Specific tests for each disorder, along with additional investigations, were employed for evaluation.5,21–23
Data processing and analysis
Heterogeneity test
Data were extracted using Microsoft Excel and imported into STATA version 11 software for meta-analysis. Cochran’s Q test was used to identify significant statistical heterogeneity, while the I2 statistic was applied to quantify the degree of heterogeneity. A p-value of less than 0.05 indicates that the observed heterogeneity is unlikely to have occurred by random chance. 24 Heterogeneity was categorized as low (I2 < 25%), moderate (25% ≤ I2 ≤ 75%), and high (I2 > 75%).25,26 Due to the presence of heterogeneity, a random-effects model was used. This model acknowledges that the included studies represent a sample from a larger population and adjusts for the heterogeneity among them. It is especially suitable for estimating the pooled prevalence when heterogeneity is present. 27 Subgroup analysis was performed based on the sampling methods to compare prevalence estimates across different groups. Sensitivity analysis was carried out to identify any individual studies that could affect the pooled estimate. Additionally, meta-regression analysis was utilized to statistically assess whether the characteristics of the primary studies influenced the reported prevalence.
Publication bias
A funnel plot was used to visually assess publication bias. Furthermore, a statistical test was conducted to quantify the probability of publication bias. A p-value of less than 0.05 in Egger’s test indicates a potential presence of publication bias.
Result
Study selection
A total of 15,348 records were identified through electronic searches, including 34 from PubMed, 557 from Science Direct, 14,500 from Google Scholar, and 257 from the African Journal Online. About 8963 duplicate articles were removed, and another 4457 were excluded for not being relevant to the research topic. The full texts of the remaining 45 articles were assessed for eligibility, after which 35 were excluded due to unclear outcome reporting and difference in the study populations. Eight studies were included in this systematic review and meta-analysis study (Figure 1).

PRISMA flow diagram for a systematic review and meta-analysis on the prevalence of MSDs and associated factors in patients with DM in Ethiopia (N=8).
Overview of included studies
The current study included 8 primary articles published up to 2023, with a total of 6076 study participants. Four of these articles were found from Amhara region28–31, two from Addis Ababa,32,33 and the remainder from South and Tigray region.34,35 All studies were published in journals that undergo a peer-review process. The included studies had sample sizes ranging from 301 to 1168 participants. Seven studies used an Institutional Based Cross-sectional study (CBCS) and one was conducted in Community Based Cross-sectional study (CBCS) design. The highest prevalence of MSDs (43.92%) was reported in Addis Ababa, 32 while the lowest prevalence (5.6%) was observed in Amhara region 31 (Table 1).
Summary of the studies included in the systematic review and meta-analysis on the prevalence of MSDs and associated factors in patients with DM in Ethiopia (N = 8).

Quality appraisal
The Joanna Briggs Institute’s critical appraisal checklist for analytical cross-sectional studies was applied to evaluate study quality, and the articles that met the inclusion criteria have high methodological quality (Supplemental File 2).
Meta-analysis
Pooled prevalence and associated factors of MSDs
The pooled prevalence of musculoskeletal disorders among patients with diabetes in Ethiopia was 27.79% (95% CI: 21.90–33.68), with moderate heterogeneity across studies (I2 = 59.7%; Figure 2). Higher prevalence was observed among participants older than 50 years, those with hypertension, and those with diabetes duration of 10 or more years. Rural residents also reported a higher prevalence of musculoskeletal disorders compared to urban residents (Figure 3).

Forest plot for the prevalence of MSDs among patients with DM in Ethiopia (N=8).

Factors associated to MSDs among patients with DM in Ethiopia (N=8).
Subgroup analysis
The subgroup analysis based on region indicates that the highest pooled prevalence of MSDs among patients with DM (42.74%) was reported in studies conducted in Addis Ababa (Figure 4).

A subgroup analysis presented in the forest plot illustrates the pooled prevalence of MSDs in patients with DM in Ethiopia, categorized by region (N=8).
Publication bias
The funnel plot (Figure 4) appeared asymmetric, indicating potential publication bias among the included studies. This observation was supported by Egger’s test (p = 0.000), suggesting that smaller studies with non-significant findings may be underrepresented. These findings highlight the need for cautious interpretation of the pooled prevalence estimates (Figure 5).
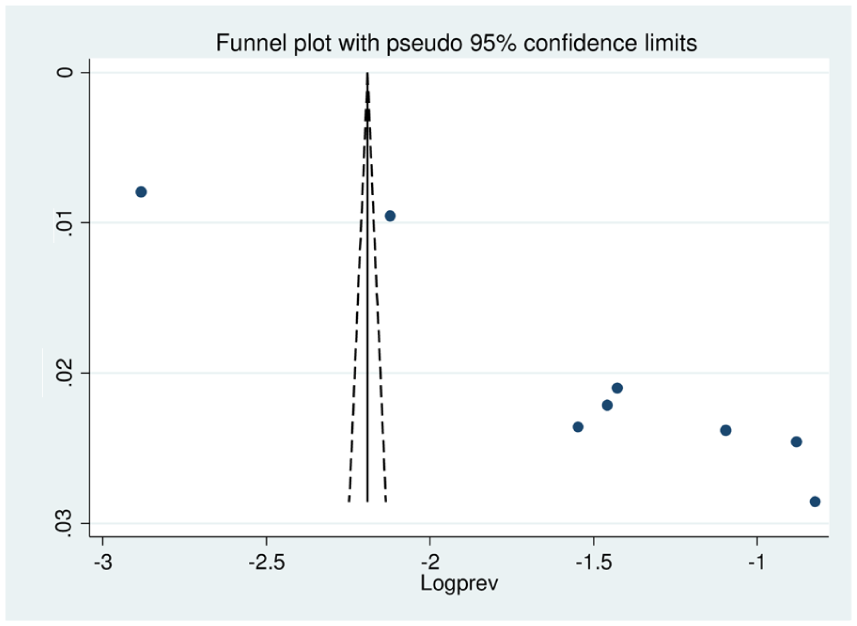
Funnel plot showing publication bias.
Sensitivity analysis
The subgroup analysis revealed a moderate level of heterogeneity between studies. We also conducted a sensitivity analysis to assess the influence of each study on the overall estimate. None of the individual primary studies had a significant impact on the pooled prevalence of MSDs among patients with DM in Ethiopia.
Discussion
This study aimed to assess the prevalence and associated factors of MSDs in patients with DM in Ethiopia. The finding of this study indicated that 27.79% of patients with DM had MSDs. The finding of this study is similar to a result of study conducted in France which reported a prevalence rate of 28.6%. 36 However, the finding of this study is higher compared to those reported in previous studies conducted in Netherland (16.3%), 37 India (19.8%), 38 and Saudi Arabia (17.9%). 14 This high prevalence of MSDs may be due to factors such as delayed diagnosis of DM, lack of patients awareness toward early screening, poor glycemic control, and inadequate management of musculoskeletal complications in our setting. 39 Additionally, better healthcare access, adherence to management practice, lifestyle modification, regular physical activity, and strict adherence to dietary guidelines could contribute to the prevalence to be low in these studies. Furthermore, this result is lower than those reported in previous studies done in Morocco (34.4%), 40 India (42.58%), 21 Turkey (45.9%), 41 Pakistan (46.7%), 42 Jordan (69.5%), 5 Canada (66%), 43 Sweden (65%), 44 and Iran (83.5%). 45 This variation may be attributed to differences in the methods used to assess musculoskeletal disorders and the types of DM studied (type I, type II, or both). Additionally, some studies focused on specific body parts, like the shoulder or hand, while others assessed the entire body. Furthermore, when comparing our findings with studies from high-income countries such as France and Canada, it is important to interpret the differences cautiously. Variations in prevalence and associated factors may be influenced by contextual and methodological factors rather than true differences in disease burden. For example, access to healthcare services, availability of diagnostic tools, healthcare-seeking behavior, lifestyle, and socioeconomic status differ significantly between Ethiopia and high-income countries. Additionally, diagnostic criteria and study designs may vary, which can affect reported prevalence estimates. Therefore, while comparisons provide useful context, these potential confounding factors should be considered when interpreting the findings.
Participants from rural areas were more likely to be associated with musculoskeletal disorders compared to those from urban settings. This disparity could be due to limited healthcare access, low awareness, delayed diagnosis, manual labor occupations, and poor diabetic follow-up systems in rural areas.46,47 In this study, MSDs were found to be more prevalent among female participants than males. This result is consistent with finding from a study conducted in Jordan. Furthermore, different studies support that females tend to have significantly higher occurrence of different MSDs compared to their counterparts. 10 The observed difference in results may be explained by the fact that due to cultural roles, household workload, and less access to health services in women.30,48
In this study, a significant association was found between the duration of DM and MSDs. The findings in our study were consistent with those of studies conducted in Jordan, 5 Turkey, 41 and India. 21 A possible explanation is that patients with DM who endure prolonged periods of hyperglycemia may experience cumulative damage in multiple areas of the body, such as the skin and feet. Persistent hyperglycemia contribute to the formation of Advanced Glycation End Products (AGEs), which result from the interaction between glucose and collagen. The buildup of AGEs leads to stiffening and reduced elasticity of collagen in the Achilles tendon, foot capsules, and ligaments, ultimately making the foot less flexible and more rigid. 49
Additionally, advanced age is associated with MSDs. This finding is consistent with the studies conducted in Iran 45 and Jordan. 5 One possible explanation is that as people age increase, there is a decline in skeletal muscle mass and strength, attributed to a decrease in muscle fibers and various cellular and molecular changes. 50 Key features of aging include bone loss, deterioration of articular cartilage, degeneration, and narrowing of intervertebral disks. These changes lead to significant biomechanical alterations that impair their function, contributing to the development of MSDs, which in turn can cause pain and disability. 51
The presence of hypertension was associated with a higher prevalence of musculoskeletal disorders compared to participants without hypertension. The association may be attributed to the micro vascular and macro vascular complications of DM, which are associated with the development of MSDs.11,52
Limitations of the study
The study has the following limitations.
Our meta-analysis showed moderate to high heterogeneity (I2 = 59.7%–94.9%) among the included studies, which is a notable limitation. This variability may be attributed to differences in study settings, regional variations across Ethiopia, diagnostic criteria for musculoskeletal disorders, sample sizes, and study designs. While a random-effects model and sensitivity analyses were employed to account for this heterogeneity, readers should interpret the pooled estimates with caution.
Furthermore, the funnel plot and Egger’s test indicated the presence of publication bias. Potential reasons for this bias include selective reporting of significant results, language restrictions (studies published only in English were included), and the underrepresentation of unpublished studies. As a result, the pooled prevalence estimates may be influenced by these factors, and the true prevalence of musculoskeletal disorders among patients with diabetes in Ethiopia could differ from the reported values.
Geographic coverage of the included studies was uneven, with certain regions of Ethiopia not represented. Ethiopia is a diverse country, with variations in ethnicity, socioeconomic status, lifestyle, and healthcare access, all of which may influence the prevalence and risk factors of MSDs. Therefore, caution is advised when generalizing these findings to the entire country. Future research should aim to include underrepresented regions to provide a more comprehensive understanding of the burden of MSDs across Ethiopia.
Additionally, all included studies were cross-sectional, which limits the ability to infer causality. While these studies can identify factors that are associated with musculoskeletal disorders among patients with diabetes, they cannot determine whether these factors directly cause MSDs. Future longitudinal or interventional studies are needed to establish causal relationships.
Despite these limitations, the findings provide useful insights into the burden of MSDs among patients with diabetes and highlight the need for more comprehensive, regionally representative studies.
Conclusion and recommendations
Musculoskeletal disorders are highly prevalent among patients with diabetes in Ethiopia, particularly among older adults, those with long-standing diabetes, and individuals with comorbid conditions such as hypertension. Screening programs and targeted interventions are urgently needed to reduce the burden and improve quality of life. Healthcare providers should consider implementing routine musculoskeletal assessments in diabetes care, and policymakers should support strategies that address regional disparities in access to care. Future research should aim to include underrepresented regions and longitudinal studies to better understand causal relationships.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251399261 – Supplemental material for Magnitude of musculoskeletal disorder and associated factors among patients with diabetes mellitus in Ethiopia: Systematic review and meta-analyses
Supplemental material, sj-docx-1-phj-10.1177_22799036251399261 for Magnitude of musculoskeletal disorder and associated factors among patients with diabetes mellitus in Ethiopia: Systematic review and meta-analyses by Worku Chekol Tassew and Yeshiwas Ayale Ferede in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251399261 – Supplemental material for Magnitude of musculoskeletal disorder and associated factors among patients with diabetes mellitus in Ethiopia: Systematic review and meta-analyses
Supplemental material, sj-docx-2-phj-10.1177_22799036251399261 for Magnitude of musculoskeletal disorder and associated factors among patients with diabetes mellitus in Ethiopia: Systematic review and meta-analyses by Worku Chekol Tassew and Yeshiwas Ayale Ferede in Journal of Public Health Research
Footnotes
Acknowledgements
The authors would like to thank the authors of the included primary studies, which were used as sources of information to conduct this systematic review and meta-analysis.
Abbreviations
CI: Confidence Interval
DM: Diabetes mellitus
JBI: Joanna Briggs Institute
MSDs: Musculoskeletal Disorders
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
POR: Pooled Odds Ratio
Ethical considerations
Not applicable since the studies used were systematic reviews and meta-analyses
Consent to participate
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data supporting the findings of this study are available within the paper and its Supplementary Information.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.