
Abstract
Background:
The ear plays a vital role in hearing and maintaining balance, which means proper care is crucial. This study examines the knowledge, attitude, and practice of ear care and hearing health in the community.
Design and Methods:
A cross-sectional study was conducted between 17 February and 16 March 2024 in three municipalities each from Surkhet and Salyan districts of Karnali Province, selected using probability-proportional-to-size sampling. Structured interviews were conducted with 1532 individuals aged 15 years and above, following informed consent. A 20-item questionnaire was used for data collection.
Results:
Among the 1532 participants, 55.1% were aged 15–44 years, and 64.6% were female. The mean knowledge score was 3.04 ± 0.93, the attitude score was 3.35 ± 0.98, and the practice score was 2.39 ± 0.81 (out of 5). Good knowledge was found in 34.7% of participants, a positive attitude in 47.7%, and appropriate practices in only 7.2%. Age was significantly associated with knowledge, attitude, and practice, with younger individuals exhibiting higher scores. Education level was significantly associated with knowledge and attitude but not with practice. Significant positive correlations were observed between knowledge and attitude, and between attitude and practice, but not between knowledge and practice.
Conclusion:
Less than half of the population demonstrated good knowledge and attitude towards ear and hearing health. Healthy practices were notably low. Younger participants had better KAP levels than older individuals. While higher education was linked to improved knowledge and attitude, it did not influence healthy practices.
Introduction
By 2050, an estimated 2.5 billion people will have some degree of hearing loss, with 700 million requiring rehabilitation services. Currently, 1.5 billion people experience some level of hearing impairment. 1 The vast majority of this number live in low- and middle-income countries, where access to ear and hearing care is limited. 2 The prevalence of hearing loss is higher in these regions due to the higher incidence of infectious diseases, many of which are preventable through public health programmes such as vaccinations and counselling. 3
The ear is essential for hearing and balance, which means proper care is crucial. 4 Cleaning the external ear with cotton buds and other objects is a common practice, as cerumen (earwax) is often mistaken for dirt. 5 However, cerumen is a natural secretion of the ceruminous and sebaceous glands in the external auditory canal. 6 An adequate amount of cerumen is necessary for preventing bacterial and fungal infections, repelling insects, and blocking water. 7 In fact, the ear canal has a self-cleansing mechanism and does not require manual cleaning. 8 While excessive care is unnecessary, proper and adequate care remains essential. 9 Using objects to remove earwax can push it deeper, making it difficult to extract, and may lead to tympanic membrane perforation, inflammation, and other complications. 10
Exposure to loud noise, including construction work and prolonged use of listening devices at high volumes, can contribute to hearing loss. 11 Other factors, such as ear infections, diabetes, and hypertension, can also impair hearing. 4 Many individuals are unaware of the risks associated with unhygienic ear care due to a lack of knowledge and awareness. 9 A 2015 study in Nigeria found that most participants cleaned their ears with cotton buds, despite their potential harm. 5
In Nepal, hearing impairment is a significant public health concern, yet limited national-level studies exist. A survey of over 79,000 schoolchildren found that nearly 6% had hearing impairment. A baseline survey on ear care practices conducted in 2021 across multiple districts revealed that 76% of respondents cleaned their ears, predominantly using potentially harmful methods such as ear buds (75.5%), metal earpicks (44.7%), and quills (12.4%). 12 Other studies have also highlighted that poor knowledge, attitude, and practice (KAP) regarding ear care are not limited to the general population, with deficiencies observed even among healthcare trainees. 9 Similarly, several intervention-focused studies from Nepal and the South Asian region have highlighted efforts to improve ear care and hearing health. For example, a recent study in Nepal evaluated hearing health awareness among Female Community Health Volunteers, underscoring the potential for community health workers to enhance ear care knowledge and early referral practices. 13 Early detection and intervention services for paediatric hearing loss remain limited in Nepal, but pilot programmes integrating infant hearing screening within immunisation clinics show promise for scaling early identification and rehabilitation, which is critical for improved developmental outcomes. Furthermore, research from South Asia indicates that comprehensive community-based ear care programmes, including training of primary care workers and school-based screenings, significantly increase timely diagnosis and management of common ear conditions. 14
Existing research highlights a gap in knowledge and practices related to ear and hearing care. 4 Karnali Province, one of Nepal’s most underprivileged regions, has low literacy rates, and ear health remains a neglected issue. Hence, this study aimed to assess the knowledge, attitude, and practices regarding ear and hearing care in Karnali Province.
Methodology
Study design and setting
This descriptive cross-sectional survey on knowledge, attitude, and practice regarding ear care and hearing health complements a prevalence study on hearing impairment conducted in Karnali Province. 15 The prevalence study, carried out by Nepal Netra Jyoti Sangh, assessed ear and hearing health in three municipalities each from Surkhet and Salyan districts. To ensure representative sampling, six municipalities were selected using the probability-proportional-to-size method. The study was conducted between 17 February and 16 March 2024.
Sampling and participants
Following the World Health Organization’s Ear and Hearing Survey Handbook 2020, the prevalence study included 2148 participants of all ages and genders. From this group, 1532 individuals aged 15 years and above were selected for the knowledge, attitude, and practice survey. The sample represented people from diverse sociocultural, ethnic, and religious backgrounds, as well as various places of birth, all of whom had resided in the area for at least 6 months. This age group was chosen as they were capable of forming opinions and making decisions. Interviews were conducted on the day of the hearing camp.
Study instrument and scoring
Data were collected using a structured interview with a 20-item questionnaire divided into four sections. The full 20-item questionnaire (English and Nepali) is provided in Supplemental Material 1. In addition to demographic data, five questions assessed knowledge of ear and hearing health, five examined attitude, and five explored practices. Participants responded to multiple-choice questions with “Yes,” “No” and “Don’t know” options. The questionnaire was adapted from a similar study conducted in Saudi Arabia, 16 translated into Nepali, and contextualised for the study sites.
Reliability and scoring
Internal consistency was evaluated using Cronbach’s alpha (ɑ = 0.7), which was within an acceptable range. Knowledge, attitude, and practice were assessed using a common grading method, assigning 1 point for correct responses and 0 for incorrect ones. Participants scoring above the For each KAP domain (0–5 scale), we classified participants scoring at or above the 75th percentile (upper quartile) within the sample as “good” and below this threshold as “poor,” consistent with prior KAP studies that use internal distribution cut-offs when externally validated cut-points are unavailable.
Statistical analysis
Data management and analysis were conducted using the Statistical Package for the Social Sciences (Version 23.0) software. Descriptive statistics were used to summarise demographic characteristics. Chi-square tests assessed associations between categorical independent and dependent variables, while Pearson correlation examined relationships between knowledge, attitude, and practice. A p-value <0.05 was considered statistically significant for all analyses.
Ethical approval
Ethical approval was obtained from the Nepal Health Research Council’s Ethical Review Board (Ref. No.: 689-2023). Written informed consent was collected from all participants, with assent and parental consent requested for those below 18 years of age. Confidentiality and anonymity were strictly maintained, and participants had the right to withdraw from the study at any time.
Results
Table 1 depicts the sociodemographic characteristics of the participants. The survey included 1532 participants, with most (64.6%) being female. Of these, 1101 were from Surkhet district and 431 from Salyan district. The largest (30.1%) age group was 15–29 years, followed by 30–44 (25.0%). In terms of education, 21.3% were illiterate, 34.5% had completed primary education, and 21.0% had attained higher education. Regarding occupation, 39% were homemakers, while 16.3% were engaged in agriculture. More than half (52.7%) had a monthly family income of NPR 21,000–50,000, while one-third had an income of NPR 20,000 or less.
Sociodemographic characteristics of the participants (district-wise).

Table 2 summarises participants’ knowledge of ear care and hearing health. While 97.2% recognised the importance of seeking medical consultation for hearing problems, only 8.2% were aware that earwax should not be removed frequently by themselves. Additionally, 82.3% agreed that sudden exposure to loud noise or music can cause hearing damage, but only 43% knew that altitude changes could lead to ear pain.
Knowledge, attitude, and practice related to ear care and hearing health.

Regarding attitudes towards ear care and hearing health, 94.3% believed that exposure to loud noise could lead to hearing loss. About 92% stated that swimming in rivers or ponds could cause ear infections, and 19% believed ear piercings should not be performed soon after birth. Nearly half (49.2%) felt that regular visits to an ear, nose, and throat (ENT) specialist were necessary even without symptoms, while 79% considered it important to check the hearing of newborns and young children.
In terms of ear care practices, 92.2% reported cleaning their ears. Only 10.1% avoided blowing their nose forcefully when suffering from a cold. Most participants (90.6%) did not use eardrops without medical advice, and 86.2% avoided prolonged exposure to loud music through headsets. Additionally, 65.9% did not use oil in their ears. Notably, self-cleaning was common (92.2%), and only 10.1% avoided forceful nose blowing during colds, two behaviours with potential to worsen middle ear problems.
The mean knowledge score (±standard deviation) out of a total score of 5 was 3.04 ± 0.93. The mean attitude score was 3.35 ± 0.98, while the mean practice score was 2.39 ± 0.81.
Figure 1 shows the proportion of participants classified as “good” (≥75th percentile) versus “poor” for each KAP domain. This highlight notable gaps in knowledge, attitude, and practice regarding ear and hearing health. Only 34.7% of participants had good knowledge, while 65.3% had poor knowledge. Attitude was more balanced, with 47.7% displaying a good attitude and 52.3% a poor attitude. However, good practices were the least common, with only 7.2% following good care practices, while 92.8% engaged in poor practices (Figure 1).
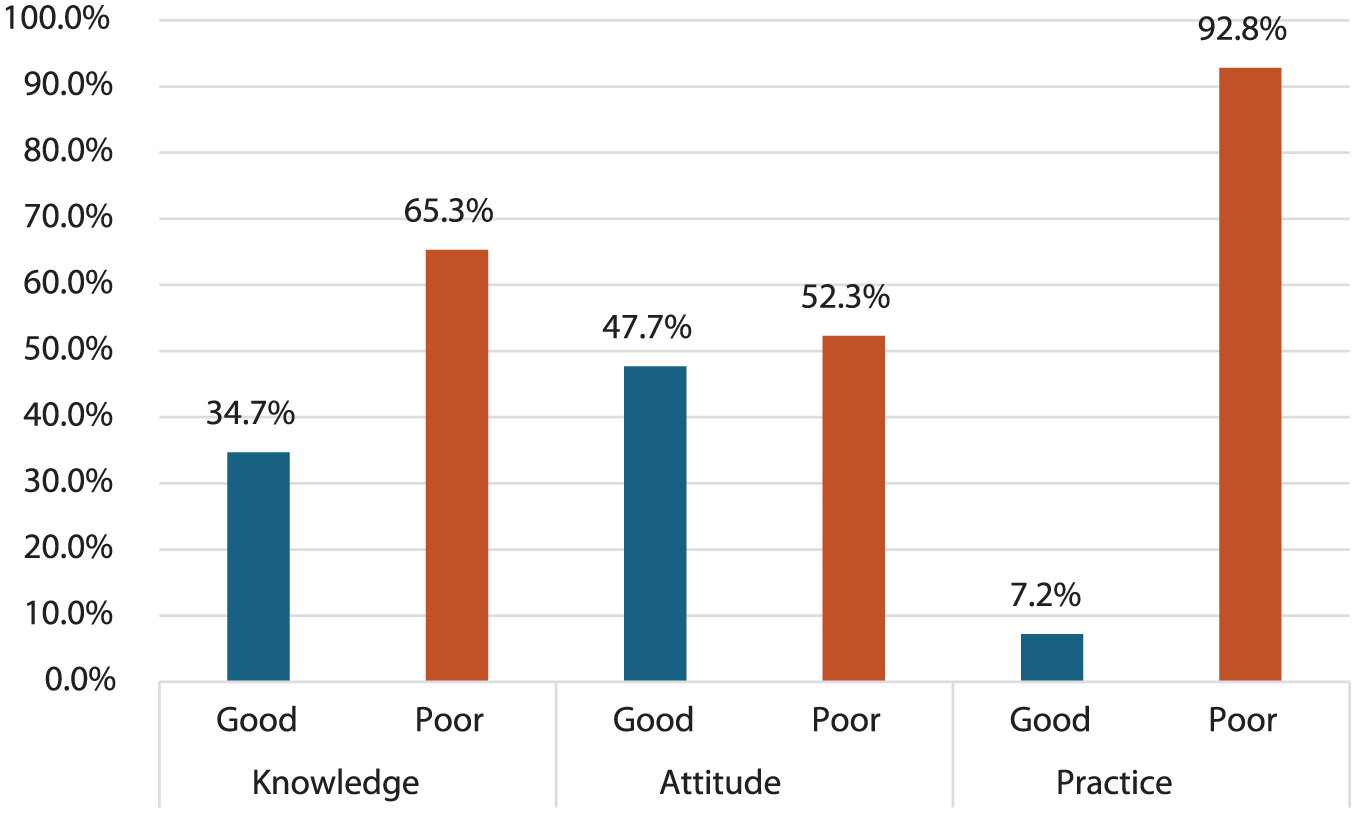
Distribution of good versus poor levels for knowledge, attitude, and practice (KAP) using ≥75th percentile threshold for “good.”
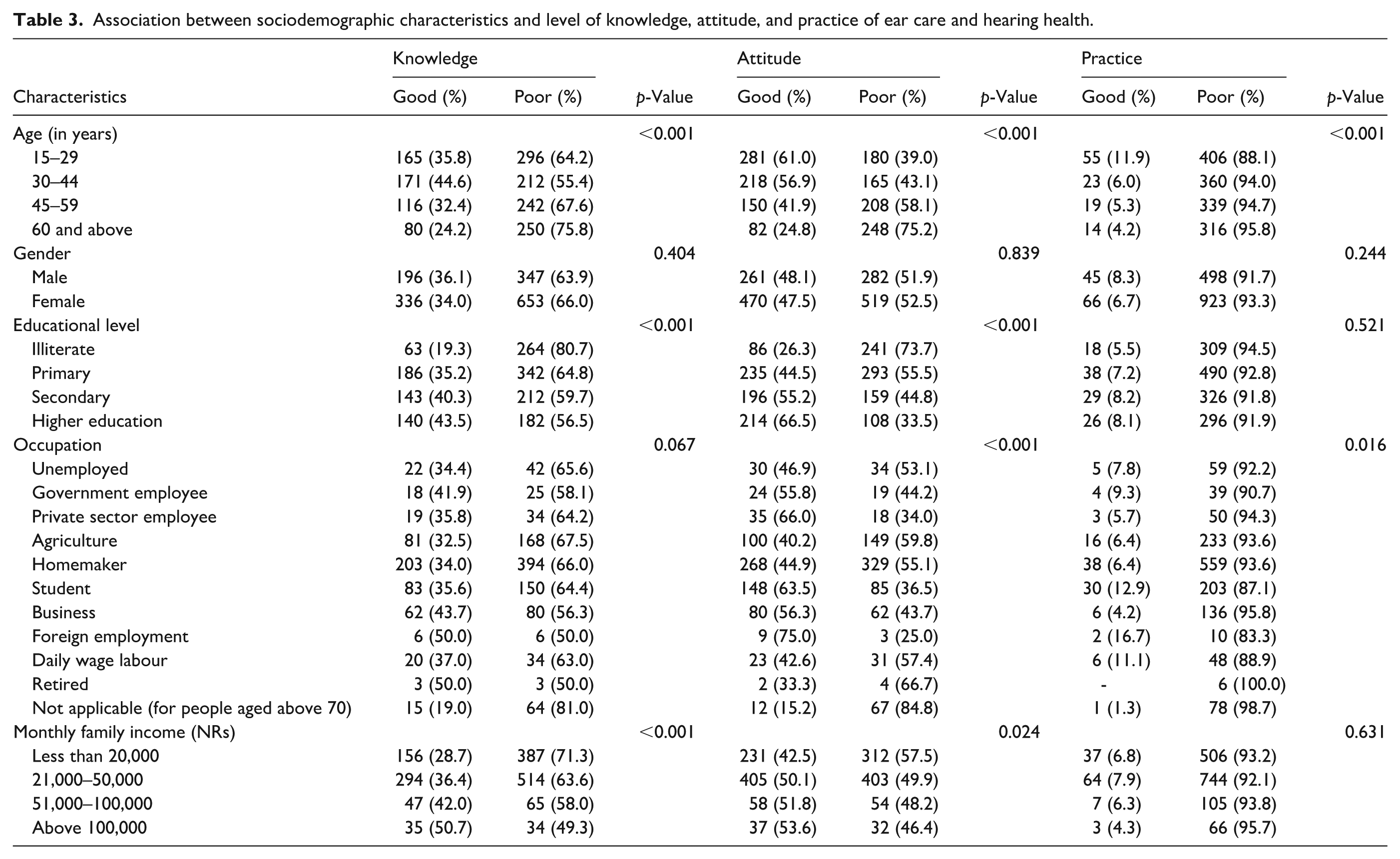
Age was significantly associated with all three dependent variables (p < 0.001). Younger individuals (15–29 years) had the highest proportion of good knowledge (35.8%), positive attitude (61.0%), and good practices (11.9%), whereas those aged 60 and above had the lowest levels (24.2%, 24.8%, and 4.2%, respectively). Education was associated with knowledge (p < 0.001) and attitude (p < 0.001), but not with practice (p = 0.521). Participants with higher education had better knowledge (43.5%) and a more positive attitude (66.5%) compared to illiterate individuals (19.3% and 26.3%, respectively).
Occupation was significantly associated with attitude (p < 0.001) and practice (p = 0.016) but not with knowledge (p = 0.067). Foreign-employed individuals had the highest positive attitude (75.0%) and good practices (16.7%), whereas homemakers (6.4%) and business owners (4.2%) had the lowest levels of poor practices. Income was significantly associated with knowledge (p < 0.001) and attitude (p = 0.024) but not with practice (p = 0.631). Those earning more than NPR 100,000 had better knowledge (50.7%) and attitude (53.6%) than those earning less than NPR 20,000 (28.7% and 42.5%, respectively). However, income did not influence practice, as poor behaviours were prevalent across all income levels.
Gender showed no significant association with knowledge (p = 0.404), attitude (p = 0.839), or practice (p = 0.244), with males and females displaying similar patterns across all variables (Table 3).
Association between sociodemographic characteristics and level of knowledge, attitude, and practice of ear care and hearing health.
Correlation analysis showed a weak but statistically significant positive relationship between knowledge and attitude (r = 0.197, p < 0.001), indicating that individuals with better knowledge tend to have a more positive attitude towards ear and hearing health. Similarly, a weak but significant correlation was found between attitude and practice (r = 0.081, p = 0.002), suggesting that a positive attitude may have a slight influence on behaviour. However, there was no significant correlation between knowledge and practice (r = −0.008, p = 0.749), signalling that knowledge alone does not necessarily lead to behavioural change (Table 4).
Correlation between knowledge, attitude, and practice scores.

Correlation is significant at the 0.01 level (two-tailed).
Discussion
This study found that 34.7% of participants had good knowledge, 47.7% had a positive attitude, and only 7.2% followed appropriate practices for ear care and hearing health. These findings align with a study by Dosemane et al. 4 in coastal Karnataka which also reported low levels of knowledge, attitude, and practice. However, these results contrasted with a study by Alharbi et al. 16 in Saudi Arabia. This disparity may be due to variations in the sociocultural backgrounds of the study populations.
Regarding knowledge, 91.8% of the participants were unaware that earwax should not be self-removed regularly. This contrasts with the findings of Alharbi et al., 16 where more than half of the participants demonstrated good knowledge. Self-cleaning of ears should be discouraged, as it may lead to conditions such as neurodermatitis, otitis media, or earwax impaction, potentially causing long-term complications. 17 In this study, 73.4% of participants were aware that a perforated eardrum requires surgery, while 82.3% recognised that exposure to loud noise or music can damage hearing. These results are similar to those reported by DelGiacco et al., 18 where 96% of participants responded correctly. The differences in findings may be linked to educational background.
Almost all participants (97.2%) correctly stated that medical consultation is necessary for hearing difficulties, consistent with a study by Mukara et al., 19 which found that most participants sought healthcare for hearing issues. However, only 43% correctly identified that changes in altitude can cause ear pain, whereas the majority in Alharbi et al.’s 16 study answered correctly. This difference may be related to variations in educational levels.
Participants generally had a positive attitude towards hearing health. In this study, 94.3% believed that loud noise could cause hearing loss, whereas Rus et al. 20 found that less than half of their participants shared this belief. This difference may be due to the participant group in the latter study, which focused on sawmill workers who may have had limited awareness of noise-related risks.
Additionally, 93% of participants believed that swimming in rivers or ponds could lead to ear infections. However, only 19.9% had a cautious attitude towards early ear piercing, whereas 44.2% of participants in Alharbi et al.’s 16 study believed ear piercing should be delayed. This contrast may stem from cultural differences, as early ear piercing is common in Nepal.
Only half of the participants in this study indicated they would visit an ENT specialist without symptoms, in contrast to Poole et al., 21 who reported that many participants had not consulted a doctor in several years. Meanwhile, 79% of participants supported newborn hearing screening, aligning with Alharbi et al.’s 16 findings, where most participants recognised its importance for early diagnosis and treatment.
In this study, 92.2% of participants reported cleaning their ears, similar to findings by Adoga and Nimkur, 22 where most participants engaged in this practice. This may be due to the common belief in Nepalese society that ear cleaning is beneficial. Despite the potential risks association with nose blowing, such as increased intranasal pressure that may force fluid from the nasal cavity into the sinuses and middle ear cavity, 23 89.9% of participants reported doing so when experiencing a cold or influenza. This contrasts with Alharbi et al.’s 16 findings where only about half of the participants engaged in this practice.
Most participants in this study did not use ear drops without consulting a doctor. This is consistent with Alsuhaibani et al., 24 where the majority sought medical advice before using ear drops. Despite awareness of noise-induced hearing impairments, 13.8% reported prolonged use of headsets to listen to loud music, a finding similar to a Swedish study by Widen et al. Additionally, 65.9% of participants reported pouring oil into their ears, corresponding with the study by Dosemane et al. 4 in Karnataka, where this practice was common. In Nepal, this may be influenced by religious customs.
Age was significantly associated with knowledge, attitude, and practice, whereas Alharbi et al. 16 and Alruwaili et al. 25 found no such connexion. Gender was not linked to any of the three variables, in contrast to studies where gender had a major association with ear care practices.16,26 Education level was notably associated with knowledge and attitude but not with practice, differing from Haji et al.’s 27 findings, which reported no link between education and knowledge.
Occupational differences were linked to variations in attitude and practice, in contrast to the findings of Alharbi et al., 16 who reported no such association. An increase in monthly family income was associated with better knowledge and attitude, but not with improved practice, again differing from Alharbi et al., 16 which reported no marked association for any variable.
The study identified a clear relationship between knowledge and attitude, as well as between attitude and practice. This suggests that individuals with more knowledge are likely to hold more positive attitudes, and those with positive attitudes are more inclined to follow appropriate practices. However, having good knowledge alone does not necessarily lead to good practice.
Findings suggest the importance of embedding ear and hearing health within primary care services. Simple measures such as counselling on safe ear care, avoidance of harmful practices like self-cleaning, and education on noise exposure can be delivered during routine visits. Community groups, schools, and municipal health units provide practical entry points for awareness-raising and early checks in children. Strengthening referral pathways to ENT services, including outreach and emerging tele-otology options, can further improve timely care.
Importantly, the findings from this KAP study on ear and hearing health in Karnali Province align with broader patterns observed across public health domains in Nepal. National-level studies on eye health, diabetes, cardiovascular health, and salt intake consistently show that while general awareness or attitude may be relatively high, actual health practices often remain poor. For instance, despite 78% of participants having basic eye health knowledge, many still relied on self-medication or informal care. 28 Similarly, only a small proportion of diabetic patients (16%) and salt consumers (18.4%) reported engaging in recommended behaviours, even though education and counselling improved knowledge and attitude.29,30 The adolescent cardiovascular health study showed a reverse gap—better practices than knowledge—indicating that behaviour change may occur through channels other than formal understanding. 31
This study has both strengths and limitations. A key strength is the large sample size, which improves the reliability of the findings. As a community-based study that included participants from various age groups, educational levels, and income brackets, the results are likely to reflect the wider population of Karnali Province. The knowledge, attitude, and practice data collected can also be used for comparison in future studies across other provinces, helping to shape more effective strategies. However, including participants from all provinces would have strengthened the evidence base for broader interventions. Also, because “good” versus “poor” was defined relative to the sample distribution, classification may understate absolute deficits when overall performance is low. To address this, we report item-level percentages (Table 2), which show low correct responses on critical behaviours (e.g. only 8.2% knew earwax should not be self-removed). Given the cross-sectional design, these associations do not imply causality; unmeasured mediators, such as access, norms, and risk perception, likely influence the translation of knowledge and attitudes into practice. Additionally, social stigma may have led some participants to withhold information, possibly affecting the accuracy of the data. Recall bias and the influence of peer discussion may also have affected some responses.
Conclusion
Participants demonstrated limited knowledge, attitude, and practice regarding ear care and hearing health, with practice scores being the lowest. No link was observed between knowledge and practice. By age group, younger individuals tended to show better knowledge, attitude, and practice. While higher education and income were associated with improved knowledge and attitude, they had no clear effect on practice.
Recommendation
To address the gaps found in the study, effective health education programmes should be developed and implemented, including community outreach, public campaigns, and the integration of ear health education into existing healthcare services. Furthermore, a nationwide study is recommended to gain a broader understanding of knowledge, attitude, and practices related to ear care and hearing health.
Supplemental Material
sj-pdf-1-phj-10.1177_22799036251397744 – Supplemental material for Knowledge, attitude, and practice of the general population towards ear care and hearing health in Karnali Province, Nepal
Supplemental material, sj-pdf-1-phj-10.1177_22799036251397744 for Knowledge, attitude, and practice of the general population towards ear care and hearing health in Karnali Province, Nepal by Ranjan Shah, Anil Paudel, Rishi Bhatta, Richa Acharya, Krishna Khadka, Manisha Budhathoki, Prakriti Maharjan, Sailesh Kumar Mishra, Roshana Kandel, Sanju Maharjan, Diego Santana-Hernández, Man Bahadur Kunwar and Manish Gautam in Journal of Public Health Research
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all six municipal offices for granting approval to conduct this research. We are also thankful to CBM international (Christoffel-Blindenmission Christian Blind Mission e.V.), for their valuable technical and financial support. We are also deeply thankful to all the participants for their time and the valuable information they shared.
Author contributions
Conceptualization: RS, MG, SKM, RK, DSH; Methodology: SM, RB, MG, AP, KK, RA; Investigation & data curation: RB, RA, MB, PM, SM, SMa, MK; Formal analysis: AP, RB, KK, RA; Visualization: KK, SM; Writing—original draft: MG, AP, RB, RA, KK, RS; Writing—review & editing: MG, MB, PM, SKM, RK, SM, SMa, DSH, MK, RB, RA, AP, KK; Supervision: MG, SKM, RK, RB; Project administration: MG, RS, MK.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data collection process is detailed in the Methods section of this article. Data can be obtained from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.