
Abstract
Background:
Risky sexual behavior (RSB) among youth can lead to serious socio-economic and health problems, such as unwanted pregnancy and acquired immune deficiency syndrome (AIDS). Little is known about RSB among secondary school students in the South Omo zone, South Ethiopia. Therefore, this study aimed to assess the magnitude of RSB and its determinants among secondary school students in the study area.
Design and methods:
An institution-based cross-sectional study was conducted in January 2023. A multistage sampling method was used to select 538 students. A structured self-administered questionnaire was used to collect data. Binary logistic regression analysis was used to determine associated factors. The level of statistical significance was declared to have a p-value less than 0.05 in multivariate analysis.
Results:
The prevalence of RSB among study participants was 25.9% (95% CI = 22.3, 29.9%). It was significantly associated with having close sexually active close friends (adjusted odds ratio (AOR) = 3.09; 95% CI: 1.90–5.02), attending night clubs (AOR = 2.56; 95% CI: 1.35–4.86), drinking alcohol (AOR = 1.90; 95% CI: 1.10–3.29), experiencing parental neglect (AOR = 2.10; 95% CI: 1.35–3.29) and poor HIV/AIDS knowledge (AOR = 1.76; 95% CI: 1.12–2.77).
Conclusions:
RSB among secondary school students in the South Omo zone was high. It was associated with the presence of sexually active friends, attendance at night clubs, alcohol consumption, parental neglect experience, and poor HIV/AIDS knowledge. Subsequently, it is necessary to strengthen HIV/AIDS education in schools, promote parental engagement in adolescent health, and raising community awareness on the risks of alcohol use and nightclub attendance.
Introduction
Young people aged 10–24 years, including most secondary school students, undergo rapid physical and psychosocial changes that make them vulnerable to risky sexual behavior (RSB).1,2
RSB includes early sexual initiation, multiple sexual partners, inconsistent condom use, and engagement with high-risk partners such as commercial sex workers or individuals with known HIV risk factors.3,4 These behaviors are linked to serious health and social consequences, including unwanted pregnancies, infertility and sexually transmitted infections, especially HIV/AIDS.5–7
Despite global progress in adolescent sexual health, RSB remains a significant challenge.8,9 In 2020, youths contributed 44% of new HIV infections in sub-Saharan Africa despite comprising only 20% of the population. 9 In Ethiopia, 0.2% of youths aged 15–24 are HIV-positive. 10 In 2019, 38.4% of U.S. high school students reported sexual experience; 8.6% had four or more lifetime partners. 11 Similar patterns are seen globally: 25% of Swedish youth had multiple partners in the past year, 12 36.1% of Colombian students engaged in RSB, 13 and 87.3% of Malaysian adolescents reported not using condoms. 14 In sub-Saharan Africa, high levels of multiple partnerships and low condom use are common, especially among male and female adolescents, respectively.15,16
Ethiopia has developed strategies to meet the sexual and reproductive health needs of young people in the country and to end AIDS as a public health threat in 2030.10,17 Strategies include improving sexual, reproductive and maternal health and reducing the burden of sexually transmitted infections. 17 Nevertheless, Ethiopia still faces many young people’s challenges with RSB. 18 Previous studies have reported various aspects of RSB. For example, research at Mizan Aman found that 30.5% of adolescents engaged in dangerous sexual activities, particularly in multiple partnerships and inconsistencies in the use of condoms. 19 Similarly, research at Aksum and Addis Ababa reported significant levels of initial sexual introduction and unsafe sexual practices.20,21
In contrast to earlier studies,22–24 this study evaluates RSB by considering it as a composite of all four dangerous behaviors, including participation in multiple partnerships, early sexual activity, inconsistency in the Little is known about the scope of RSB and its determinants among secondary school students in the South Omo zone. This zone, facing increasing urbanization, a growing influx of migrants, and expanding liquor outlets, may pose heightened risks for HIV transmission among youth. 25 This study aims to assess the prevalence and determinants of RSB among secondary school students in the South Omo zone, providing evidence to inform targeted public health interventions.
Methods
Study design and period
An institution-based cross-sectional study was conducted from 1 January to 31 January, 2023.
Study setting
The study was conducted in the South Omo zone, 767 kilometers southwest of Addis Ababa, Ethiopia’s capital. The South Omo zone is part of the Ethiopian region of the southern nations, nationalities and people’s region and is located as its administrative city of Jinka. 26 It is one of Ethiopia’s socially most diverse zones, containing a minimum of 12 different ethnic groups and possibly as many as 21. There are 820,480 people in nine districts of the South Omo zone who live as pastoralists and/or agrarians. In the South Omo zone, there are 21,848 students in 35 secondary schools comprising 11,651 male students and 10,197 female students.
Study participants
The source population for this study was all secondary school students in the South Omo zone, whereas the study population was all selected students in the selected secondary schools found in South Omo zone. All regular students aged 15–24 years who were registered in a selected secondary school were included in the study. On the other hand, all secondary school students who were unable to respond due to sickness orthose students who were attending night classes were excluded from the study.
Sample size determination
Considering 95% confidence level (z = 1.96), 5% marginal error (w) and 30.5% prevalence (p) of RSB from a study in Mizan Aman, 19 the following single population proportion formula yielded a sample size of 326:

The study in Mizan Aman used a similar operational definition of RSB, which included early sexual debut, multiple partners and inconsistent condom use. 19 However, our study, just like a study in Jiga, North Ethiopia, expands on the study done in Mizan Aman by including engagement with commercial sex workers as an additional component of RSB. 27
Subsequently, by multiplying the initially computed sample size by a design effect of 1.5 to account for multistage sampling and incorporating a 10% adjustment for potential nonresponse, the ultimate sample size reached 538.
Sampling procedure
The selection of study participants utilized a two-step multistage sampling method. Initially, three districts (Dasenech, Jinka and South Ari) were chosen randomly from all districts in the South Omo zone. Before proceeding to the second sampling stage, the final sample size was distributed proportionally among the selected districts based on the number of secondary school students in each.
In the second stage of sampling, students were selected using a simple random sampling technique from the school register. A computer-generated randomization process was employed to ensure fairness. All secondary schools in the chosen districts were included in the study. Accordingly, the study was carried out in Omorate Secondary School of Dasenech, Jinka Secondary School, Meles Zenawi Secondary School, Bruh Tesfa Secondary School of Jinka, Goh Secondary School, Gorker Secondary School, and Metser Secondary School of South Ari.
Data collection
The data were collected using a structured self-administration questionnaire adapted from the Youth Risk Behavior Survey Questionnaire. 28 The questionnaire was prepared in English, translated into Amharic, and returned to English by speakers to check the consistency of the meaning. Before using the questionnaire independently, students received a short orientation to explain key terms and ensure understanding. Research assistants were available to answer non-leading clarifications. By placing completed questionnaires in sealed boxes in a designated private area, students can maintain the anonymity of the answer. Subsequently, research assistants collected the questionnaires daily.
Study variables and their measurement
The study designates RSB as a dependent variable. On the contrary, independent variables include socio-demographic factors such as gender, age, level of education, religion, residence, living conditions, parental education, parental occupation, pocket money, and conversations about sexual and reproductive issues. In addition, poor HIV/AIDS knowledge, parental neglect, social support, drinking alcohol, chewing hats, pornography, and participation in night clubs are also considered independent variables in the study.
The definition of RSB in this study refers to students who engage in at least one of the following acts: having multiple sexual partners (approval of more than one sexual partner until the date of the survey), starting sexual activity at an early age (experimenting the first sexual activity before the age of 18), unauthorized use of condoms (discontinuation of at least one sexual encounter until the survey), or having sexual activities with commercial sex workers at least once during sexual encounters until the survey. 29
Parental neglect was assessed using a questionnaire on adverse childhood experiences, which inquired about instances of childhood abuse (emotional, physical and sexual), neglect during childhood (emotional and physical) and dysfunction within the household (such as violence against mothers, parental separation or divorce, mental illness in the household, substance abuse within the household and the presence of an incarcerated household member). 30 Hence, if the student experienced as a child a particular type of aforementioned childhood neglects/abuses, he/she will score 1, otherwise score 0. As a result, students whose summed scores on adverse childhood experiences exceeded the average score of all students were identified as individuals who had experienced parental neglect.
Social support was assessed by the Oslo Social Support Scale, which has three items. The sum of the scores was categorized into three social support levels: poor (3–8), moderate (9–11) and strong (12–14). 31
HIV/AIDS knowledge was classified as “good” or “poor” according to the answers to the 10 standardized knowledge questions, with an average score as a threshold. 32
Data quality control
To ensure validity, the structured questionnaire was adapted from the Youth Risk Behavior Survey (YRBS), a well-valid tool used around the world to assess risk behaviors of adolescents. 28 To ensure the validity of the content, experts in public health and adolescents reviewed the questionnaire before collecting data. In addition, a pretest was conducted within 5% of the total sample size of a secondary school outside the selected study areas to assess the clarity, coherence and understanding of the items. The necessary modifications were made on the basis of feedback.
All research assistants were fully trained to meet the objectives of the study, ethical considerations and procedures for facilitating the collection of data. The questionnaire was tested two weeks before the actual data collection period, involving 5% of the final sample size, and targeted students from normal government secondary schools in unelected districts. The research assistants ensured the completeness of each questionnaire. After the data cleaning process, two data officials input the data and cross-check the data consistency. To control confounding factors, multivariable logistic regression analysis was carried out.
Data processing and analysis
Data were initially checked for completeness and coherence during collection and subsequently cleaned and encoded. Clean data were entered into SPSS version 26 for statistical analysis. Descriptive statistics (frequency, percentages, averages, and standard deviations) were used to summarize participants’ socio-demographic and behavioral characteristics.
In order to assess the factors associated with RSB, binary logistic regression analysis was carried out in two phases. Firstly, bivariate logistic regression was used to evaluate the overall relationship between each independent variable and the outcome. Variables with a p-value of 0.20 are considered eligible for multivariate logistic regression. This threshold is chosen to reduce the risk of excluding potentially confounding or suppressing variables.
Before building the multivariable model, the multicollinearity between independent variables was assessed using variance inflation factors (VIFs). Variables with VIF values greater than 5 were excluded from further analysis in order to minimize redundancy and instability in coefficient estimates, in accordance with established epidemiological guidelines. 33
The final multivariable logistic regression model was used to identify independent predictors of RSB while adjusting for covariates. The adjusted odds ratio (AOR)with 95% confidence intervals (CIs) was reported and the statistical significance was set at p-value of 0.05. Model diagnosis was carried out to validate the multivariate logistic regression model.
Hosmer-Lemeshow’s goodness-of-fit test was used to assess the model calibration, with a p-value> 0.05 indicating good fit. In addition, two-way interaction terms were constructed and tested between the selected independent variables on the basis of theoretical plausibility (e.g. alcohol consumption, participation in night clubs; parental neglect, knowledge of HIV/AIDS). In the final model, interaction terms with of p < 0.05 would be retained.
Ethics approval and consent to participate
The study was approved by the Jinka University Ethics Review Committee with reference number JKU/RCE/ERC/041/15. Confidentiality was ensured by omitting personal identifiers and the respondents provided written informed consent. For students under the age of 18, written informed consent was obtained from their legal guardians via distributed forms, which were collected by homeroom teachers. Written assent was also sought from the students themselves. Participants had the option to decline participation or withdraw from the study at any point upon their request.
Results
Sociodemographic characteristics
Of the 538 students selected for the study, 522 completed and returned valid questionnaires, resulting in a response rate of 97%. The 16 nonresponses were due to absenteeism (n = 9), incomplete responses (n = 5) and voluntary withdrawal (n = 2). Although these cases were distributed proportionally among the selected schools, no detailed data were collected from them due to the anonymous nature of the survey. The median age of the students was 17.44 years, with a range of 9 years. Approximately 58.4% and 81% of the mothers and fathers of the students were able to read and write, respectively. Monthly family income was less than 5000 Ethiopian Birr for most (58%) students. Almost half (48.5%) of the participants discussed sexual and reproductive health issues with their parents, while one third (32.2%) of them felt peer pressure on sexual and reproductive health issues (Table 1).
Sociodemographic characteristics (n = 522).

Sexual behavior
The prevalence of RSB among secondary school students in the South Omo zone is 25.9% (95% CI: 22.3, 29.9%). Forty-five (8.6%), 59 (11.3%), 25 (4.8%), and 6 (1.1%) of the students have one, two, three and four of the four risky behaviors labeled RSB, respectively. One-quarter (23.2%) of the respondents had ever had sexual intercourse, while the mean age of sexual debut was 16.52 years, with a standard deviation of 2.77 years. Of all respondents who had ever had sexual intercourse, three fourths (77.9%) of them did not always use condoms. The main reasons for not using condoms were trusting sexual partners (54.7%), unavailability of condoms (13.2%), decrease in sexual pleasure (20.8%), refusal by sexual partners (7.2%) and others (4.3%) (Figure 1) (Table 2).

Reasons to start sexual intercourse among secondary school students in South Omo zone (n = 121).
Sexual behavior of participants (n = 522).

Substance and illicit drug use
Table 3 presents the pattern of substance and illicit drug use among the 522 respondents. Regarding substance use, most students reported never drinking alcohol (81.8%), never chewing khat (93.5%), never smoking cigarettes (94.3%). Meanwhile, majority (95.2%) of them never used illicit drugs such as hashish or cocaine. Occasional use (“sometimes”) was reported by 18.2% for alcohol, 5.0% for khat, 4.8% for cigarettes, and 3.1% for illicit drugs, while regular (“often”) use remained rare, not exceeding 1.7% in any category.
Substance and illicit drug use characteristics of respondents (n = 522).

Determinants of risky sexual behavior
During multivariate logistic regression, close friends’ sexual experience, attendance at night clubs, alcohol drinking habits, parental neglect, and poor knowledge about HIV / AIDS were identified as determinants of RSB (Table 4). However, some variables, such as gender, pocket money, and religious participation, were not significantly associated with RSB. The final multivariate logistic regression model demonstrated an acceptable fit to the data, as indicated by the Hosmer-Lemeshow test (p = 0.837). Furthermore, no significant two-way interactions were identified among the independent variables (p > 0.05 for all interaction terms).
Determinants of risky sexual behavior (n = 522).
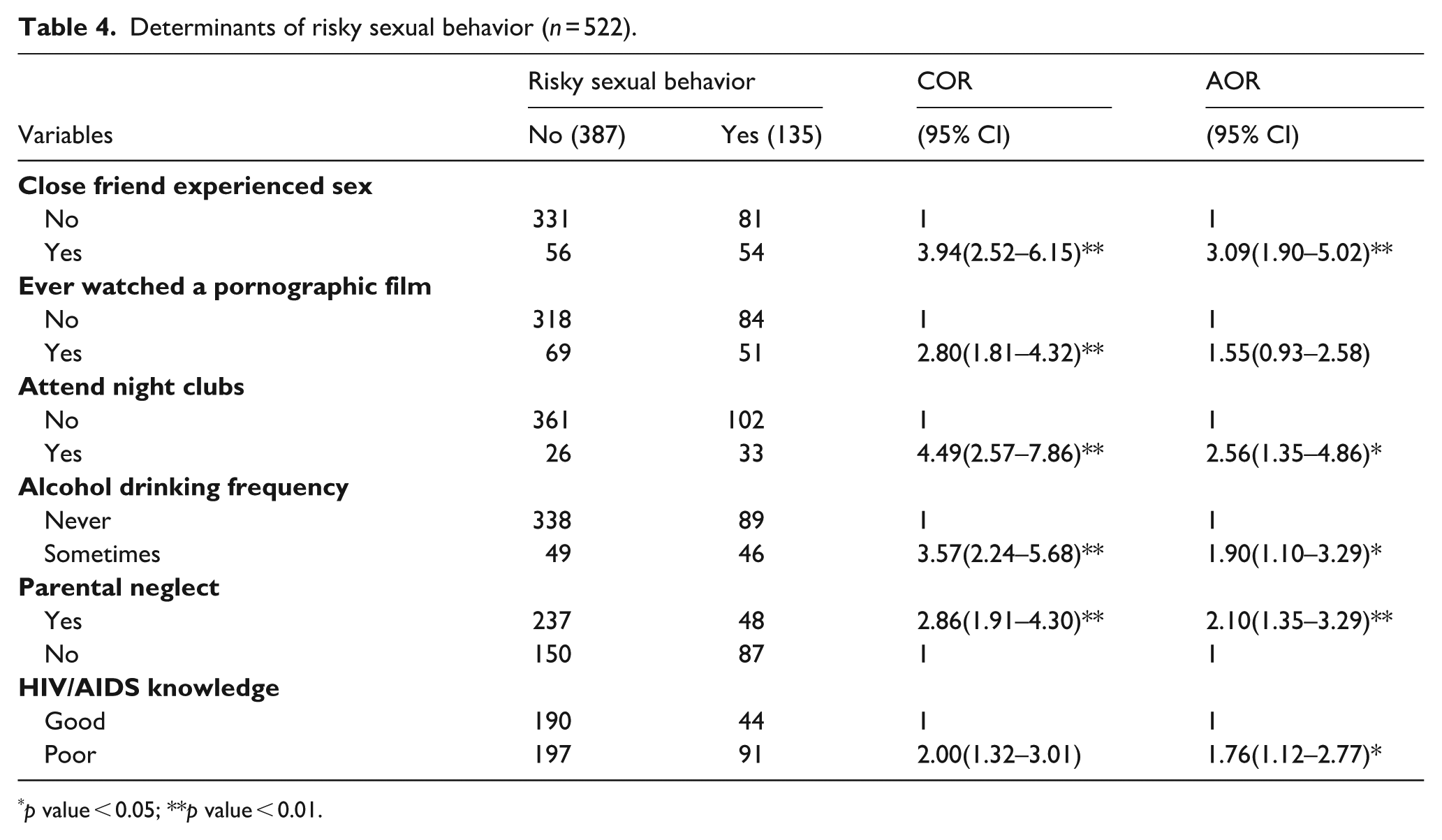
p value < 0.05; **p value < 0.01.
Respondents whose close friends experienced sex were threefold (adjusted odds ratio (AOR) = 3.09; 95% CI (confidence interval): 1.90–5.02) more likely to have RSB than respondents whose close friends did not experience sex. In contrast to students who do not attend night clubs, those students who attend night clubs are 2.56 times (AOR = 2.56; 95% CI: 1.35–4.86) more prone to RSB. A respondent who sometimes drinks alcohol 1.90 times (AOR = 1.90; 95% CI: 1.10–3.29) tends to have RSB more than a respondent who never drinks alcohol. The odds of having RSB among students with parental neglect were twice (AOR = 2.10; 95% CI: 1.35–3.29) higher than that among students with no parental neglect. Participants with poor HIV/AIDS knowledge were 1.76 times (AOR = 1.76; 95% CI: 1.12–2.77) more likely to have RSB than participants with good HIV/AIDS knowledge.
Discussion
Given the limited scientific information on the prevalence of RSB and its determinants among secondary school students in the study area, this study was deemed necessary. In this study, a respondent is said to have RSB if he/she has a practice of at least early sexual debut (before age 18), or more than one sexual partner, or not using always condom during sex, or having sexual activity with commercial sex workers. The mean age of sexual debut among respondents was 16.52 years, which means that most of the participants have started sex a very early age. This mean age of sexual debut among respondents is almost similar to a study done in India that revealed that average age at first intercourse was 15.25 years for boys and 16.66 years for girls. 34 In the current study 18.6 of participants had started sexual intercourse before the age of 18, which also shows significant number of adolescents experiencing sex at such a premature age when they don’t have that much decision making skill, exposing them to consequences of risky sexual behavior. Similarly, 18.4% of preparatory and high school students in Woldia town had early sexual initiation. 35 With a 4.4% proportion of respondents having more than one sexual partner, this study has lower magnitude of multiple sexual partnership compared to a study done in Metu town (61.7%) and Gondar city (51.6%). 22 , 36 This discrepancy might be due to socioeconomic and cultural difference. Moreover, the urban setup of the latter’s favors exposure to pornographic material and chance of having more than one sexual partner, while the strict cultural norm in the current study limits multiple sexual partnership.
This study showed that one-fourth (25.9%) of secondary school students in the South Omo zone had experienced RSB. This prevalence falls within the mid-range of estimates reported globally. For instance, a study in Sweden, a high-income country, reported that 29% of adolescents had multiple sexual partners and 17% initiated sex before age 15. 12 In contrast, a study from the United States found that 38.4% of high school students had engaged in sexual activity, with 45.7% reporting not using a condom during last sexual intercourse. 37 Studies in Latin America (e.g. Colombia: 36.1%) and Southeast Asia (e.g. Bangkok: 69.5%) show even higher rates of RSB, likely due to differences in urbanization, access to nightlife, media exposure and cultural permissiveness toward adolescent sexuality. 13 , 38
In sub-Saharan Africa, the prevalence varies widely but is often shaped by socioeconomic disparities, patriarchal norms and limited sexual health infrastructure. For example, Nigerian adolescents reported 57.4% multiple sexual partnerships, while in Rwanda, 41% of secondary school students reported some form of RSB. 16 , 39 In comparison, the prevalence in South Omo may reflect a confluence of protective factors (e.g. cultural conservatism, religious norms, limited access to mass media) and emerging risks (e.g. expansion of urban centers and local liquor stores).
The prevalence of RSB in this study is higher than that of a study conducted in Aksum town (17.2%). 20 This discrepancy may be due to differences in the operational definition of RSB. While the studies in Aksum focused primarily on early sexual debut and inconsistent condom use, our study included additional components such as engagement with commercial sex workers and multiple sexual partnerships, which may have contributed to the higher prevalence observed. The observed variation may also be explained by the difference in methodologies and socioeconomic status. Moreover, a possible explanation for the discrepancy may be the difference in the time of study. Students in this study may be increasingly exposed to pornography and nightclubs due to expanding internet access, mobile phone penetration, and urbanization in Southern Ethiopia, which have changed adolescents’ leisure activities and social interactions.
On the other hand, the magnitude of RSB in our study is less than the findings from studies in Addis Ababa (26.7%), 21 Kigali (41%), 39 and Bangkok (69.5%). 38 The lower prevalence in our study may be attributed to the rural setting of the South Omo zone, where access to technology and social media—factors that often facilitate risky behaviors—is limited. Studies have shown that adolescents’ exposure to sexually explicit content via mobile devices and social networking sites is associated with earlier initiation of sexual activity and multiple sexual partnerships. 40 , 41 Additionally, cultural norms and religious practices in the South Omo zone may discourage early sexual activity and multiple partnerships, contributing to the lower prevalence of RSB compared to urban areas like Addis Ababa and Bangkok. The region is home to multiple indigenous communities (e.g. Hamar, Ari, Dassenech), where traditional practices often include early arranged marriages and taboos against premarital sexual activity. These factors may create social environments where adolescents experience stronger behavioral regulation and less exposure to liberal sexual norms, especially in comparison to urban youth in Addis Ababa or Bangkok. Such cultural embeddedness may therefore serve as a protective mechanism against RSB.
Students whose close friends had engaged in sexual intercourse were significantly more likely to report. This is in line with past studies conducted in Wolaita Sodo town. 42 This association may be explained by peer influence, where adolescents model behaviors of their social group to gain acceptance or avoid exclusion, as shown by the study in Kigali. 39 Social learning theory suggests that perceived norms within peer networks can strongly shape attitudes toward sex, often overriding formal education or parental guidance. In settings with limited access to accurate sexual health information, peers may become the primary source of knowledge and behavioral cues. These findings underscore the potential of peer-led interventions within schools to reshape social norms and promote safer sexual behaviors among adolescents.
Students who attended nightclubs were more than twice as likely to engage in RSB compared to non-attendees, aligning with previous Ethiopian findings. 43 Nightclubs often provide unsupervised environments where adolescents are exposed to alcohol, peer pressure, and opportunities for impulsive sexual encounters, all of which contribute to increased risk-taking. The combination of disinhibition from alcohol and social expectations in such settings may undermine adolescents’ ability to make informed decisions. These findings suggest that environmental and structural factors such as alcohol availability and access to nightclubs in the community, play a critical role in adolescent sexual behavior.
In harmony with prior studies in Nigeria, 44 and in Ethiopia, 45 this study discovered that a higher frequency of alcohol consumption increases the chance of having RSB. Alcohol impairs cognitive control and lowers inhibition, increasing the likelihood of unprotected sex or multiple partnerships. Behavioral economics explains this through present-biased preferences, where immediate gratification overrides long-term health concerns like STIs. This effect is amplified in social environments such as nightclubs, where peer approval reinforces risk-taking. Additionally, alcohol use before sex may serve as a justification for avoiding condom use, perceived as socially acceptable in some youth contexts. These findings highlight the interplay between substance use, cognitive bias, and social norms in shaping adolescent sexual risk-taking.
Consistent with a study carried out in Aksum town, 20 this study showed that parental neglect significantly increased the likelihood of engaging in RSB among secondary students. Adolescents who lack consistent parental monitoring, emotional support, or communication about sexual health are more likely to rely on peers or media for guidance, which may reinforce risky norms. Studies show that neglect disrupts adolescent decision-making and self-regulation, increasing vulnerability to external influences.39, 42 , 46 Moreover, the absence of parental supervision can reduce accountability and weaken protective family structures. These dynamics suggest that beyond individual behavior, family context plays a critical role in shaping adolescent sexual choices. Strengthening parent-child communication and household stability could serve as key preventive strategies in reducing RSB.
Having good HIV/AIDS-related knowledge among secondary students was associated with a lower RSB experience in the current study area. This association is in agreement with a study performed in Arsi Negele. 32 This could be attributed to likely enhanced HIV risk perception and high protective behaviors among students who have comprehensive understanding of HIV transmission, particularly through unprotected sex and multiple partnerships. Knowledge serves as a cognitive tool that enables informed decision-making, fostering self-efficacy in avoiding unsafe sexual practices. In contrast, misinformation or knowledge gaps may reduce perceived susceptibility, leading to higher risk-taking. These results highlight the importance of integrating accurate, age-appropriate HIV education into school curricula, not only to increase awareness but also to promote behavioral change essential for reducing RSB among adolescents.
The study relied on self-reported data, which may be subject to recall bias. Although the response rate was high (97%), the exclusion of 16 students may introduce a small degree of non-response bias. Since non-respondents’ characteristics were not recorded due to confidentiality measures, the impact of their exclusion on representativeness remains unknown. The exclusion of students attending night classes may introduce selection bias, potentially excluding certain groups with distinct characteristics related to RSB. In this study, RSB is operationally defined as engaging in at least one of the following behaviors: early sexual initiation (before age 18), multiple sexual partnerships, inconsistent condom use, or engaging in sexual activity with commercial sex workers. However, some other risky behaviors, such as unprotected sex with partners of unknown HIV status, or substance use during sexual encounters were not included in this definition. Unlike the study in Mizan Aman, whose prevalence used for sample size calculation of this study, our study used a similar operational definition of RSB, but by including engagement with commercial sex workers as an additional component of RSB, which could potentially result in measurement bias. 19 Despite efforts to maintain confidentiality, respondents may provide answers they perceive as socially acceptable, leading to a bias in the reporting of sensitive behaviors. Hence, future studies should include all students and should employ longitudinal study designs to explore the temporal relationship between various factors and RSB.
The study’s focus on RSB among secondary school students is highly relevant to public health, considering the potential social, economic, and health consequences associated with such behaviors. The use of a two-step multistage sampling method enhances the representativeness of the study. The study comprehensively assesses RSB by considering it as a composite of four specific behaviors, providing a more nuanced understanding of the prevalence and determinants of these behaviors among secondary school students.
Conclusions
The prevalence of risky sexual behavior (RSB) among secondary school students in South Omo zone is concerning. Key factors associated with RSB include frequent alcohol use, nightclub attendance, peer influence, parental neglect, and poor HIV/AIDS knowledge. Interventions should focus on strengthening HIV/AIDS education in schools, promoting parental engagement in adolescent health, and raising community awareness on the risks of alcohol use and nightclub attendance. Future research should explore underlying mechanisms using longitudinal and qualitative approaches.
Significance for public health
As young people transition from childhood to adulthood, they undergo rapid physical and psychosocial changes facing many new challenges including RSB. Among adolescents, RSB can lead to serious social, economic and health harms such as unwanted pregnancy and sexually transmitted diseases. Contrary to earlier research, this study will evaluate RSB by considering it as a composite of all four risky behaviors. Little is known about the magnitude of RSB and its determinants among secondary school students in the South Omo zone. Hence, this study was designed to determine the prevalence of RSB and its determinants among secondary school students in the South Omo zone. The study has substantial implications for decision-makers, urging a multifaceted approach to address the high prevalence of RSB among secondary school students in the South Omo zone. It recommends interventions that incorporate educational, social, and environmental components to create a holistic framework for reducing RSBs.
Footnotes
Acknowledgements
The authors are grateful to Jinka University for financial support and ethical clearance to conduct this work. Our acknowledgment also goes to thank the South Omo zonal health department for giving us permission to carry out the research and providing some relevant information. We extend our heartfelt appreciation to the data collectors, supervisors and study participants without whom this work has been accomplished.
Abbreviations
AIDS: Acquired Immunodeficiency Disease; AOR: Adjusted Odds Ratio; CI: Confidence Interval; HIV: Human Immunodeficiency Virus; RSB: Risky Sexual Behavior.
Author contributions
GAT wrote the study proposal, including its methods and work plan, in addition to analyzing the data and writing the results. GAT, EWW, MDA and BAA supervised the data collection and wrote the discussion and conclusion. EAT interpreted the data and wrote the discussion and conclusion. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jinka University sponsored the data collection of this study through the grant reference number JKU/RCE/13091. The funder has no specific role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.