
Abstract
Objective:
To investigate the different contributions made by nurses in the management of patients with post covid-19 condition (PCC) within the French healthcare context.
Methods:
We conducted a qualitative study among healthcare professionals in France and enrolled 17 nurses from different care sectors, including private practice, hospitals, schools, and research settings. Semi-structured interviews were conducted between October 2022 and June 2023. The inclusion criteria were: “be a nursing professional” and “having taken care of a patient with PCC.” A content thematic analysis was carried out using NVIVO software with advanced pattern recognition analysis, applying the French nursing competency framework to categorize findings.
Results:
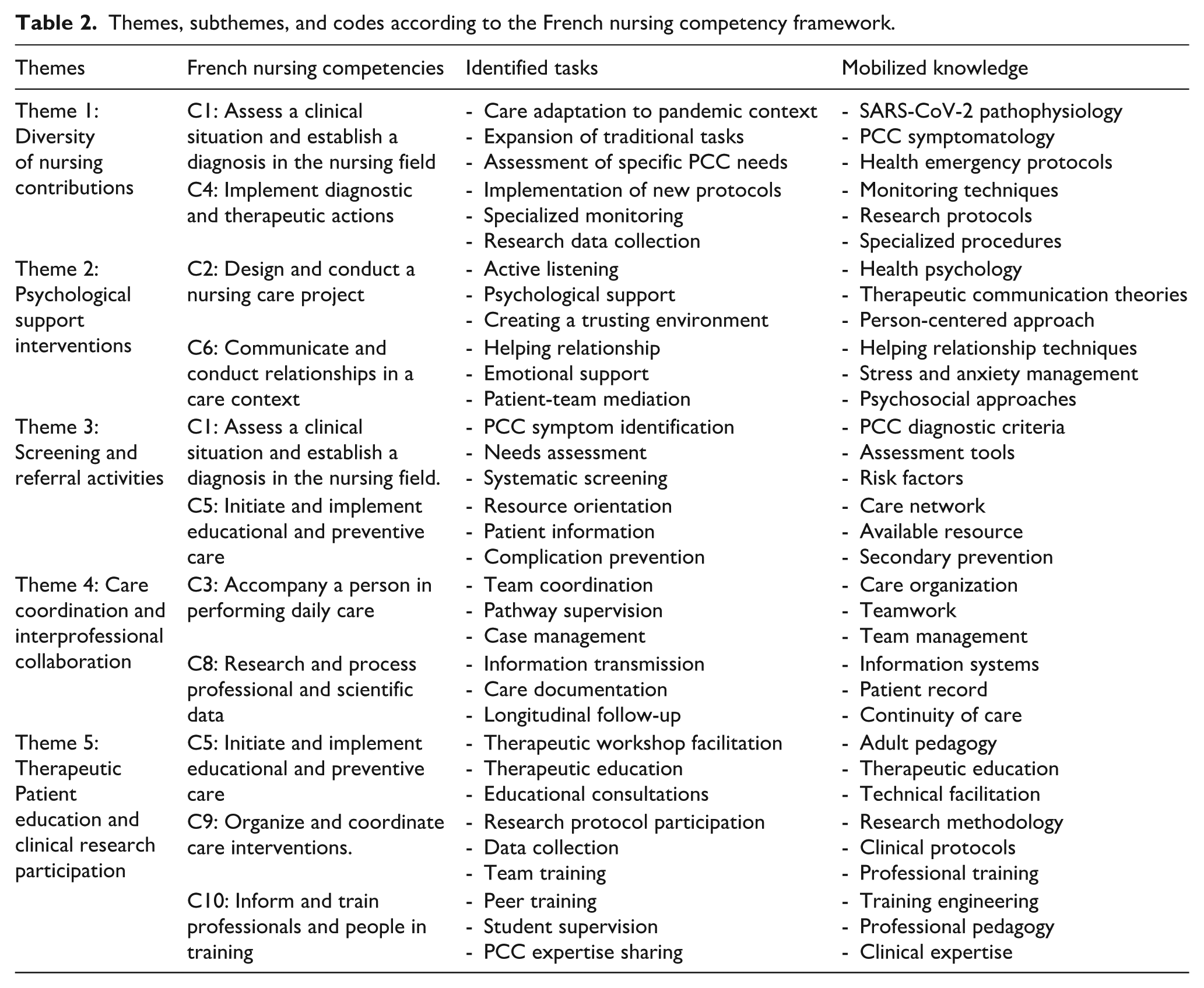
Five main themes emerged: (i) the diversity of nurses’ contributions and responsibilities, (ii) psychological support: an essential nursing contribution, (iii) screening and referral activities for PCC patients, (iv) care coordination and inter-professional collaboration responsibilities, and (v) therapeutic patient education and clinical research participation. Nurses demonstrated expanded competencies in PCC symptom recognition, adapted traditional tasks to meet novel patient needs, and integrated evolving Long Covid knowledge with existing chronic disease management expertise.
Conclusion:
The results offer important perspectives for the organization of the healthcare system and for the nursing profession in the management of chronic diseases. An important aspect of our findings concerns the coordination of care pathways, which raises the issue of task delegation to nurses, particularly in a context of healthcare professional shortages.
Keywords
Introduction
Covid-19 is no longer front-page news, however it remains a major public health problem. Covid-19 is a disease resulting from SARS-CoV-2 viral infection, characterized by a variety of systemic symptom. The cardinal symptoms of post covid-19 condition (PCC) include fatigue, cognitive impairment, and shortness of breath, 1 through other manifestations such as heart palpitations and muscle pain may also occur. 2 The emergence of PCC symptoms was observed as early as spring 2020. According to WHO criteria, 10%–20% of patients infected with Covid-19 develop PCC. 3 The WHO defines PCC as the continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation.4,5 It should be noted that “Long Covid” is a British term with specific definitions outlined in NICE guidelines, referring to symptoms persisting beyond the acute phase of infection. 5
Current management guidelines exist for PCC. The WHO has published specific guidelines for PCC, and various national health authorities, including the French Higher health Authority 6 have developed their own protocols. These guidelines generally recommend a holistic, multidisciplinary approach involving multiple healthcare professionals.7,8
The management of patients with PCC shares similarities with that of people suffering from chronic illnesses. 9 Indeed, the symptoms of PCC overlap with those of other chronic conditions such as myalgic encephalomyelitis/ Chronic fatigue syndrome (ME/CFS) 10 as well as persistent diseases that can result from a wide variety of other infectious agents such as Ebola, Epstein-Barr, hepatitis C virus and human immunodeficiency virus. 11
A multidisciplinary approach is essential to meet the diverse and varied needs of patients with chronic diseases. Thus, as for other chronic conditions, Fugazzaro et a. 12 suggested an integrated and interdisciplinary approach for better management of patients with PCC. This integrative approach requires a care pathway involving several healthcare professionals, including nurses.
Nursing plays a crucial role in chronic disease management. The nursing profession involves a variety of essential responsibilities, including the analysis, organization, evaluation, and delivery of nursing care. Lee et al. 13 described five critical roles that nurses assumed during the pandemic: reorganizing care systems, improving team communication, coordinating essential equipment, improving the effectiveness of healthcare as frontline carers, and supporting other nurses. A systematic review by Poitras et al. 14 identifies four areas of nursing practice: comprehensive assessment of people with chronic conditions, care management, promotion of health and well-being, and promotion of collaborative relationships between nurses and physicians.
In the French healthcare context, nurses frequently serve as the first point of contact for patients in private practice settings. They act as knowledge resources, offering advice on recovery, serving as role models in rehabilitation, facilitating positive psychological well-being, orchestrating social support for patients and their families, and providing holistic care that addresses the physical, psychological, social, and spiritual aspects of the chronic condition, including both management and prevention.
While existing guidelines mention the importance of nursing contributions in Long Covid management, there is a notable gap in detailed exploration of specific nursing contributions and responsibilities in this context. The WHO guidelines reference nurses without elaborating on their detailed contributions and responsibilities in PCC care pathways. This study addresses this evidence gap by providing a qualitative exploration of nurses’ experiences and contributions to PCC management in France, which is essential for informing future practice and policy development.
PCC is a recent medical syndrome and, as such, management strategies are constantly evolving. In France, with approximately 500,300 nurses employed and 98,600 nurses in private practice 15 the nursing workforce represents a significant resource for managing the growing number of PCC patients. The key role of nurses in the management of other chronic diseases has already been demonstrated. 16 Despite this, there are a limited number of publications exploring the nurses’ contributions in the management of PCC.
The main aim of this study is to investigate the different contributions made by nurses in the management of patients with PCC within the French healthcare system, using a competency-based framework to categorize findings. Understanding the contributions of nurses in the care of patients with PCC would help to improve the management of these patients, who often experience medical wandering due the complexity and variability of their symptoms.
Materials and methods
Study design
From a methodological point of view, we used a qualitative method to understand whether, in the context of the appearance of a new syndrome, the experiences reported by the nurses make it possible to identify roles that are different from those usually exercised in the management of other pathologies. We adopted an inductive approach involving semi-structured interviews to understand their experiences and express the vison they have of their work. 17 This study was conducted in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 18 A completed COREQ checklist has been provided as Supplemental Material.
Conceptual framework
To analyze nursing contributions, we applied the French nursing competency framework established by the nursing diploma reference framework. 19 This framework distinguishes 10 core competencies that define nursing practice in France: competencies (integrated knowledge, skills, judgment, and attributes), tasks (specific activities performed), roles (defined professional functions), and responsibilities (accountabilities within scope of practice). This established framework helped categorize our findings according to recognized French professional standards and ensured consistent analysis across interviews. The framework also considers the continuum from novice to expert practice and contextual factors influencing nursing practice in the French healthcare system. The competency framework was applied during analysis to systematically categorize nursing contributions. Their application to PCC represents novel practice development acknowledging the emergency context. The results were then subjected to a thematic analysis to identify and structure all the emerging themes.
Recruitment, participants, and setting
Participants were recruited through healthcare professional organizations using study information leaflets. The inclusion criteria were: “be a nursing professional” and “having taken care of a patient with PCC.” A total of 17 nurses participated in this study with no refusals. No prior professional relationships existed between the interviewer and participants, who were informed that the interviewer was a nurse-researcher conducting doctoral research. All participants provided written informed consent after receiving comprehensive study information. Interviews were carried out between October 2022 and June 2023.
Data collection
To identify the nurses’ contributions to care pathways for patients with PCC, we collected nurses’ representations and perceptions of their contributions in the care of these patients using an interview guideline developed and then tested with two nurses from the research team. The interview guideline was validated by the members of the research team.
The interviews were conducted by the first author (O.L.K.), a female PhD student in public health who is also nurse working in private practice (her experience includes participation in previous qualitative research projects). The interviews were formalized in the form of semi-structured interviews to allow participants to speak freely about the aspects of them experiences they considered important. 20
As the interviews progressed, the interview guideline was adapted using an inductive approach to allow the participants to express freely. No interview needed to be repeated. The interview guideline was structured around several themes: (i) knowledge of the disease; (ii) diagnostic understanding; (iii) disease management and nursing contributions; (iv) professional organization; (v) improvement suggestions.
As it was sometimes difficult to conduct interviews in the nurses’ different places of practice, and to obtain as many participants as possible, some interviews were conducted face-to-face, while others were conducted remotely by phone. No other individuals were present during the interviews except the participant and interviewer. With participants’ agreement, interviews were audio-recorded and field notes were taken. Transcriptions were anonymized and audio files destroyed according to institutional data protection protocols. After 17 interviews, no new elements emerged, so we decided to stop collecting data. 21 The interviews lasted between 25 and 45 min on average. All interviews were conducted in French. The original transcriptions were then translated into English by the principal author who is bilingual (O.L.K.). To ensure accuracy and fidelity of the statements, each translation was systematically reviewed and compared to the original French recordings and transcriptions and validated by a second bilingual member of the research team (Pr. C.N.N.).
Data analysis
Descriptive analyses characterized study participants. Interview transcripts were coded (P1-P17) and thematic analysis was conducted using NVIVO software (version 12), employing advanced pattern recognition features to identify recurring themes and relationships. Following Braun and Clarke’s framework, data were coded independently by two researchers (O.L.K. and J.G.) with continuous debriefing sessions held to ensure reliability and consistency. 22 To improve the reliability of the coding process, the authors carried out continuous debriefing throughout the data analysis. The competency framework was applied during analysis to systematically categorize nursing contributions. Potential themes were examined and refined to determine whether a theme presented a coherent thematic pattern. We have collected a lot of information’s: Information regarding nurses’ personal and professional experience with Covid-19, symptoms and impact of Long Covid, supportive and rehabilitative approaches; training and knowledge regarding Long Covid; challenges and gaps in the management of PCC, professional and organizational adaptations and roles of nurses in the management of patients with PCC. However, the guiding ideas of our findings are defined by the purpose of our study. As ethically minded researchers, we were rigorous in identifying the themes that emerged from our data.
Research rigor
Multiple strategies ensured scientific rigor throughout the study: diverse participant recruitment across sectors and experience levels; dual coding by researchers with qualitative expertise (J.G., PhD); use of NVIVO’s advanced analytical capabilities; member checking with participants for validation; and data saturation achieved after 17 interviews following Guest et al.’s recommendations. 21
Results
Descriptive analysis
The nurses interviewed came from different sectors. There was one man for every 16 women. This gender difference reflects the general trend toward feminization of the nursing profession. Their years of experience varied, ranging from 3 to 31 years. Participants worked across various settings: hospitals (specialized PCC units, cardiology, follow-up and rehabilitation care, intensive care, palliative care), private practice, schools and research settings. The professional profile of the participants is presented in Table 1 (professional characteristics of participants).
Professional characteristics of participants.

Thematic analysis
To analyze nursing contributions, we applied the French nursing competency framework. Results are showed in Table 2. The nurses interviewed acknowledged that the Covid-19 pandemic posed new challenges for them and the healthcare system. They were on the front line. Their roles had diversified and evolved to adapt to clinical and organizational challenges.
Themes, subthemes, and codes according to the French nursing competency framework.
Theme 1: The diversity of nurses’ contributions and responsibilities
1.1 Adapting contributions to pandemic context and PCC emergence.
With Covid-19 pandemic onset, nurses continually adapted their working environment to cope with health emergency demands in the French healthcare system. Several nurses’ testimonials illustrate this flexibility.
At the beginning, it was a blow of anxiety and fear for me, then also a great professional questioning and with adaptability, to find quickly to take care of these patients. (P14; H)
They also spoke of the need to modify their traditional functions to respond to the urgency of care research and the needs of PCC patients. They contributed to research by appointing and employing a nurse for data collection.
We’ve even doubled the posts of clinical research officers and clinical protocol nurses with a normal consultation nurse so that we have total control over vaccination research. (P15; H)
In this context, nurses have been given greater responsibilities, particularly in the management of persistent Long Covid symptoms, where collaboration has become essential.
1.2 Variety of clinical and administrative tasks
Nurses describe the complexity of treating Long Covid, both physically and psychologically. Hospital services have adapted to the needs of patients with Long Covid. The nurses emphasized the need for multidisciplinary care and recognized certain gaps in resources.
We are working on the physical aspect. It’s clear that they’re improving their skills [. . .] they’re better, but their neurological problems haven’t been resolved. (P16, H)
Some healthcare professionals have highlighted the confusing nature of the various clinical cases. The symptoms of Long Covid are diverse and include ageusia, severe and chronic fatigue, chronic pain, neurological disorders, cardiac complications and impact on mood, as described by participants. Long Covid patients often find it difficult to return to normal work activities due to debilitating fatigue that interferes with their daily lives and work responsibilities.
Symptoms include agueusia, severe and chronic fatigue, chronic pain, neurological disorders, cardiac complications and effects on mood and morale. (P4, H)
In this context of complex care, the nurses have taken on a range of functions, from resuscitation (during Covid 19) to managing follow-up consultations for patients with Long Covid. They play a proactive role in interdisciplinary collaboration and suggest several actions to improve Long Covid care, including enabling patients to be active partners in their own care.
We should be able to refer patients to the appropriate organisations and resources, including families, not just patients. (P13, H)
This diversity of tasks facilitated the continuity of patient care.
Theme 2: Psychological support: An essential nursing contribution
All the nurses interviewed recognized their role in caring for patients with Long Covid. All 17 professionals interviewed agreed that they had a role to play in listening to and supporting patients with Long Covid. In this distressing situation, the healthcare professionals stressed the vital importance of listening as the first therapeutic intervention for patients. Indeed, participants noted the profound relief felt by patients when they find themselves in an environment where they are “finally heard” and “without judgement.”
Because of their close relationship with patients, nurses are often the first to identify signs of emotional or psychological distress. Some stress the importance of active listening and empathy in the nurse-patient relationship, It’s true that I would have liked to wear a different hat, a bit of a psychologist, because it’s not unusual for patients to collapse [. . .] So it’s not easy. [I think it’s really a time for listening and sharing. (P16; H)
This need for psychological support can also be explained by the presence of fluctuating symptoms, which are often misunderstood by certain healthcare professionals and by those around patients who complain.
Afterwards, I say that covid has a good back, there are some who blame everything on covid. You must be careful. There have been some since I’ve had covid, I’ve got this, I’ve got that, but hey. There’s nothing proven. Is it really linked to covid? (P2; H)
The nurses, in their role as mediators, offer patients a space where they can express their concerns and frustrations, thereby strengthening the relationship of trust.
Patients often come to see me to talk about their illness and their fears, and we try to reassure them. I think our role goes beyond physical care, it’s also about listening to them and giving them a space where they can express themselves. (P7; PP)
Theme 3: Screening and referral activities for PCC patients
To identify these symptoms, nurses regularly enquire about patients’ current complaints, medical history, and potential exposure to Covid-19. This will enable them to direct patients to the appropriate care channels.
It’s really necessary to distinguish between people with Long Covid and those with other conditions. (P3, S)
Once these patients have been identified, the nurses provide them with essential information and refer them to available resources.
Our responsibility includes referring people to specialist centres. (P12, H)
Nurses have had to adapt to a wide range of symptoms and have identified the need for specific training in this area in order to better guide and monitor patients.
I think there should be more information and training so that carers can better understand long Covid and its after-effects. (P1; PP)
Theme 4: Care coordination and interprofessional collaboration responsabilities
The nurses interviewed stressed the need for a holistic approach and multidisciplinary care for patients with long-term conditions, You need a network of different professionals to monitor these patients properly. (P15; H)
This monitoring will enable patients’ needs to be readjusted.
We have a monitoring role to check whether the rehabilitation and treatments we have advised them have been successful and whether any adjustments need to be made. (P1; PP)
Wherever they work, whether in a practice or a hospital, nurses work closely with the entire medical team to formulate personalized care plans for patients and constantly monitor their progress over time.
It’s an integral part of our role to provide feedback to the GP: how is the patient this week? How are they feeling? What feedback has he given? (P10, PP).
Interdisciplinary collaboration requires coordination. This need was expressed by some nurses: There’s a real need for collaboration with different professionals, [. . .] We have to ensure that patients have access to all the care they need, which means good communication with the multidisciplinary team. (P15; H)
The coordinator’s role is essential to ensure ongoing monitoring. He or she ensures that there is good communication between all the professionals involved in the patient’s care and supports the patient throughout the entire care process.
In my hospital, I’m responsible for overseeing the patient’s journey: from arrival to referral to other professionals depending on their needs (P4; H)
Thanks to their position, nurse coordinators provide accurate information to other professionals, optimizing the quality of care.
Theme 5: Therapeutic Patient education and clinical research participation
Long Covid is a chronic disease, and patients often must live with disabling symptoms such as chronic fatigue and respiratory problems. Therapeutic patient education is a tool that enables patients to take charge of their own health. Some nurses run therapeutic education workshops specific to Long Covid to teach patients how to live with this syndrome.
We have an educational role, especially in explaining to them how to manage their chronic fatigue and breathlessness. These are things that can help them improve their daily lives. (P2; H) We need to offer them educational consultations to teach them how to manage persistent symptoms, flare-ups and fatigue. (P15, H)
The nurses stressed the need to listen. Patients want to meet other patients with the same problems and want their illness to be recognized.
Really on this long covid group I leave a lot of room for discussion and exchange. I try to guide things and bounce off what everyone says. (P17, H)
Long Covid is a little-known pathology, and several studies are being set up. Nurses are involved in these studies at several levels.
Our protocol, basically, [. . .] IT is there to do a bit of observational data, a bit of forecasting, even a bit if there are signs that are common to patients, in our department, we have several studies underway. (P14, H)
Discussion
This study explored the different contributions made by nurses in the management of patients with PCC. Contributions vary depending on the practice setting. Using the French nursing competency framework 19 recently modified, 19 we identified that nursing contributions to PCC span multiple competency domains: psychological support, screening, referral, clinical follow-up, coordination and organization of activities and care, and even contribution to clinical research. Application of the competency framework revealed:
Competency expansion: Nurses developed new competencies in Long Covid symptom recognition and management
Task diversification: Traditional nursing tasks were adapted to meet novel patient needs
Knowledge integration: Nurses integrated evolving Long Covid knowledge with existing chronic disease management expertise.
Contributions identified align with nursing competencies described in the French professional framework, though their application to Long Covid represents novel practice development. Most of them are in line with the activities described in the French professional framework. 19 Our results show that for nurses, psychological support is the most frequent contribution in the care of PCC patients. The lack of recognition of the PCC pathology, and the multiplicity and fluctuation of symptoms, generate feelings of frustration and distress in patients. This often translates into a need for nurses to listen empathetically and sympathetically. Indeed, the proximity of nurses to patients helps to create an environment of trust and listening, where patients feel understood and supported in their care. These results are in line with those of Babaii et al., 23 who show that the quality of communication between nurse and patient is an influential factor in improving patient care.
PCC is an illness that is not yet recognized by some healthcare professionals. 24 In the field, this situation sometimes leads to patients wandering in search of solutions. The second contribution described by the nurses in our study provides a response to this wandering. It involves screening and referring PCC patients. Nurses are often the first to identify patients with symptoms of PCC and refer them to appropriate care. 25 This seems essential in order to avoid medical wandering, a phenomenon which, as Mwangi and Siegelman point out 26 affects many patients who suffer in silence from PCC. In the French healthcare context, particularly in private practice, nurses often serve as the initial point of contact for patients seeking care. They conduct preliminary assessments and guide patients to family physicians or other healthcare professionals based on the clinical situation.
Among other identified contributions, care coordination and organization particularly interested us. Long-term care strategies are like those put in place for patients with complex needs. For this type of patient, coordination between different professionals is essential. According to the Agency for Healthcare Research and Quality, care coordination can be defined as “the deliberate organisation of care activities between two or more participants (including the patient) involved in the care of a patient in order to facilitate the appropriate delivery of healthcare services.” 27 Our results show that in several care pathways for patients suffering from Long Covid, the coordinating role of care pathways was given to nurses. Our results are similar to those of Karam et al. 28 who showed that nurses play an important role in coordinating the care.
The approach to caring for patients with post-COVID conditions demonstrates integrated and effective care delivery. While quotes from professionals may initially give the impression of professional aspirations, they reflect evidence-based practices supported by the cases managed. Our findings demonstrate that for PCC patients, it is imperative to deploy a comprehensive and continuous care pathway – and our participants have successfully operationalized this integration.
However, coordination presents a number of problems, particularly those linked to the delegation of tasks. 29 These include human resources (the professionals to whom the task is delegated must be available), skills, acceptance of new tasks, and regulations. While the French healthcare context is marked by a shortage of healthcare professionals in general, this is accentuated among physicians. According to recent statistics, France faces significant healthcare workforce shortages, with rural and underserved areas particularly affected. 30 Task shifting to nurses, as demonstrated in our study through their expanded coordinating roles in PCC care, represents a strategic response to these shortages. This delegation aligns with WHO recommendations on task shifting in healthcare 31 and mirrors successful models in other European countries such as the Netherlands and UK, where nurse practitioners assume expanded responsibilities in chronic disease management. 32
While this study focused on the French context, international interest in the role of nursing in post-COVID care is evident. In the United Kingdom, the NHS England report, Long COVID: A framework for nursing, midwifery, and care staff (2022), highlights the roles of specialist nurses in symptom assessment, patient monitoring, and care coordination within post-COVID services. Also in Australia, a multidisciplinary post-COVID recovery clinic (Long COVID Recovery Clinic) was deemed acceptable by its users, highlighting the importance of coordinated care involving different healthcare professionals. 33 The care coordination role identified in our findings aligns with international trends toward nursing leadership in chronic disease management but may be particularly pronounced in the French context due to physician workforce shortages and the tradition of autonomous nursing practice in private settings.
Post-pandemic implications
As we enter the post-pandemic phase, the nursing roles and care coordination mechanisms developed for PCC management may serve as a model for future health system responses to emerging chronic conditions. With an estimated 65 million people worldwide experiencing Long Covid, 34 PCC has transitioned from an acute pandemic response issue to a chronic disease management challenge. The nursing competencies identified in our study: screening, coordination, therapeutic education align with broader trends toward nurse-led chronic disease management models. The adaptability demonstrated by nurses during the pandemic represents valuable organizational learning for future health emergencies. The care pathways and coordination mechanisms developed for PCC could serve as templates for managing other complex, multi-symptom conditions or future pandemic-related chronic conditions. This evolution is already being operationalized through innovative programs such as SPACO+ (Monitoring and Adapted Pathways for People Suffering from Persistent Symptoms of Covid-19), 35 a program we have developed which combines therapeutic education methods with personalized multifactorial interventions. Such programs demonstrate how nursing-led initiatives can provide comprehensive, multidisciplinary care that addresses the complex needs of patients with chronic post-viral conditions, potentially serving as templates for future pandemic preparedness and chronic disease management strategies.
Significance for public health
Nursing work is difficult to specify, as it includes many recognized and unrecognized aspects. The results of this study offer important perspectives for the organization of the French healthcare system and for the nursing profession in chronic disease management. The results highlight the expansion of nursing contributions, particularly in the areas of screening, psychological support, and inter-professional collaboration. By strengthening tasks that are still underdeveloped, such as contributing to clinical research or coordinating care pathways, our work highlights the central contribution made by nurses in prevention and the organization of the healthcare system in France.
Strengths and limitations of the study
To date, few research studies have examined nurses’ contributions in supporting patients with PCC. As with any research, certain limitations must be considered. Firstly, all the nurses voluntarily agreed to take part, which may introduce a selection bias. Nurses with positive and motivating opinions or experiences might be more inclined to participate, which could influence the results in the direction of a more positive view of their role. We opted for a qualitative study to explore nurses’ perceptions; this study is therefore not intended to reflect the diversity of practice in the nursing profession across all French healthcare settings. Our study could be supplemented by a questionnaire distributed to a larger sample, to confirm or refute the prevalence of these contributions. While we applied the French nursing competency framework to guide our analysis, the retrospective application of this framework to data originally collected without this specific theoretical lens may have limitations. Future studies would benefit from a priori framework application from the data collection stage. The results indicate that nurses had difficulty distinguishing between patients with COVID-19 and patients with post-COVID-19 syndrome when answering questions, which could lead to potential diagnostic bias. The study was conducted in France with specific healthcare system characteristics, which may limit result generalizability to other healthcare contexts.
Conclusion
Multidisciplinary collaboration appears essential to meet the complex needs of patients with Post Covid-19 condition. This qualitative study allowed for the description of the various and essential contributions that nurses make to patients Post Covid-19 Condition care pathways. An important aspect of our findings concerns the coordination of care pathways, which raises task delegation questions to nurses, particularly in the French context of healthcare professional shortages. This delegation, although essential for the effective organization of care, raises significant questions regarding human resources, the required competencies, and the recognition of these new responsibilities. Looking ahead to the post-pandemic era, it would be relevant to explore innovative approaches, such as collaborative and proactive city-hospital pathways, where nurses would play a central role. The evolution of nursing contributions and responsibilities, highlighted by this study, opens important perspectives for the continuous improvement chronic disease management and healthcare system organization.
Supplemental Material
sj-pdf-1-phj-10.1177_22799036251390963 – Supplemental material for Management of patients with post Covid-19 condition in France: A qualitative study exploring nurses’ contributions to care pathways
Supplemental material, sj-pdf-1-phj-10.1177_22799036251390963 for Management of patients with post Covid-19 condition in France: A qualitative study exploring nurses’ contributions to care pathways by Odette Linda Kamdem, Jessica Guyot, Caroline Dupre, Pauline Gouttefarde, Marie Pierre Vericel, Marie Fanget, Céline Nguefeu Nkenfou, David Hupin, Frederic Roche, Elisabeth Botelho-Nevers and Bienvenu Bongue in Journal of Public Health Research
Footnotes
Acknowledgements
The authors would like to thank all the researchers in the SPACO+ team. The members of the PRESAGE institute: Franck Chauvin, Véronique REGNIER, Nathalie BARTH, Yves MBAMA, Elie SHIKITELE, Fanny COLLANGE, Amandine BAUDOT.
Ethical considerations
Our study was approved by the ethics committee of the Saint-Etienne University Hospital Centre under the reference IRBN1282023/CHUSTE.
Consent to participate
All participants sign an informed before entering the study.
Consent to publication
Not applicable.
Author contributions
Study design: JG, FR, EBN, and BB.
Data collection: OLK, PG, MPV, and MF.
Data analysis: OLK, JG, and CD.
Drafting of the manuscript: OLK.
Critical review of important intellectual content: DH, EBN, CNN, FR, and BB.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the SPACO+ project, which has received funding from ANRS – Agence Nationale de la Recherche/Emerging Infectious Diseases (Grant number: ANRS283). The funders were not involved in the design of the study, the collection and analysis of the data, the decision to publish or the preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Full interview data is not publicly available due to privacy or ethical restrictions. However, the data is available on reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.