
Abstract
Objective:
The COVID-19 pandemic increased the risk of interpersonal violence. We investigated the association between lifetime interpersonal violence experience and risk of post–COVID-19 condition (the persistence of symptoms of COVID-19 and severity of health problems associated with COVID-19 that last a few weeks, months, or years) among women with lifetime interpersonal violence experience.
Methods:
Women participants aged ≥18 years in Kentucky’s Wellness, Health & You—COVID-19 study completed online quantitative surveys about the impacts of the pandemic, developing COVID-19, and symptoms of post–COVID-19 condition. We conducted cross-sectional analyses estimating rate ratios of developing COVID-19 and symptoms of post–COVID-19 condition during the pandemic (October 13, 2020–February 28, 2022).
Results:
Of the analytic sample (N = 938), 342 (36.5%) disclosed a history of lifetime interpersonal violence. Compared with women with no lifetime interpersonal violence experience, women with lifetime interpersonal violence experience had significantly more distress because of the pandemic, defined as family financial challenges (P = .001), symptoms of mental health challenges (P < .001), and negative coping behaviors (P < .001). While experiencing lifetime interpersonal violence was not significantly associated with either receiving COVID-19 vaccinations (adjusted rate ratio [aRR] = 1.10; 95% CI, 0.75-1.61) or developing COVID-19 (aRR = 1.15; 95% CI, 0.92-1.44), experiencing lifetime interpersonal violence was associated with an increased rate of developing symptoms of post–COVID-19 condition (aRR = 2.09; 95% CI, 1.19-3.65).
Conclusion:
Symptoms of post–COVID-19 condition may be linked to lifetime interpersonal violence experience, possibly through stress or violence-associated trauma. Future research is needed to assess the negative effects of the pandemic, prioritizing people with lifetime interpersonal violence experience.
In early March 2020, the World Health Organization declared the COVID-19 pandemic. 1 Those at increased risk of being hospitalized or dying from COVID-19 include older adults, those who are pregnant, and those who have underlying medical conditions, severe disabilities, or mental health disorders.2-4 Females are more likely than males to be infected with SARS-CoV-2, the virus that causes COVID-19. 5 Groups that have been economically or socially marginalized, those with low income and education levels, those who are employed in essential industries, and those who require in-person contact are disproportionately affected by COVID-19.2,4-12 Pandemic-related psychological stressors (eg, isolation or loneliness, fear of infection, financial or childcare concerns) are risk factors for chronic inflammation that lead to neurocognitive deficits and mental disorders among people infected with SARS-CoV-2.4,13 Those who are hospitalized with COVID-19 are more likely to experience cognitive impairment, depression, and anxiety than those who are not hospitalized with COVID-19. 14 The COVID-19 pandemic also increased the risk of interpersonal violence experience15-17; current and lifetime interpersonal violence experience may additionally increase the distress and related life and health challenges of living through the pandemic. Social isolation exacerbates personal and collective vulnerabilities while limiting accessible and familiar support options.18,19
COVID-19 and Post–COVID-19 Condition
Post–COVID-19 condition is defined as the persistence of symptoms of COVID-19 and the severity of health problems associated with COVID-19 that last a few weeks, months, or years after a person becomes infected with SARS-CoV-2.20-22 Based on worldwide estimates, about 54% to 72% of people who are hospitalized with COVID-19 experience at least 1 symptom of post–COVID-19 condition.23,24 The major symptoms of post–COVID-19 condition are excessive fatigue, difficulty breathing or shortness of breath, headache, cough, difficulty thinking or concentrating, sleeping problems, and chest, stomach, joint, and muscle pain.20,25 While the long-term physical and mental symptoms of COVID-19 have yet to be definitively established, a meta-analysis by Zeng et al, 26 representing >1 million participants with COVID-19 worldwide, suggests that 50% of COVID-19 survivors have symptoms of post–COVID-19 condition up to 12 months after SARS-CoV-2 infection. Furthermore, psychiatric symptoms, primarily depression, posttraumatic stress disorder (PTSD), or anxiety, were observed in 19.7% of patients with post–COVID-19 condition, and cognitive or memory deficits were observed in 19.7% and 17.5% of patients with post–COVID-19 condition, respectively. 26 Women, older adults, and those with severe clinical symptoms or coexisting morbidities are at highest risk of experiencing symptoms of post–COVID-19 condition.21,27 Of those infected with SARS-CoV-2, women are at higher risk than men of developing symptoms of post–COVID-19 condition.28,29
Lifetime Interpersonal Violence and Immune Dysregulation
Exposure to violence, including intimate partner violence (IPV), nonpartner sexual violence, and child physical and sexual abuse, is associated with severe stress-related mental disorders (eg, depression, PTSD, anxiety, substance use) and immune dysregulation among women.30-32 Prolonged exposure to violence-related stress causes alterations in the hypothalamic-pituitary-adrenal (HPA) axis, which can trigger a substantial physiological stress response.33-36 Chronic stress associated with trauma can increase cortisol concentrations caused by HPA-axis dysregulation and lead to neurocognitive deficits and serious mental disorders among women exposed to violence (ie, women exposed to IPV).13,37,38 Child physical and sexual abuse are associated with autoimmune diseases in adulthood.39-41
Given the preponderance of evidence suggesting that chronic stress is related to lifetime interpersonal violence experience and that this stress negatively affects the HPA axis and triggers an immune response, women with lifetime interpersonal violence experience may be more susceptible to developing serious symptoms of post–COVID-19 condition than women with no lifetime interpersonal violence experience.31,42,43 SARS-CoV-2 infection does trigger a strong chronic inflammatory response,44,45 and those with autoimmune disorders and chronic health conditions are at increased risk of developing COVID-19 and symptoms of post–COVID-19 condition. 2 Violence-associated trauma increases the risk of HPA-axis dysfunction linked with chronic stress and the risk of autoimmune disorders31,37,39; we hypothesized that lifetime interpersonal violence experience may be associated with an increased rate of reporting symptoms of post–COVID-19 condition. The objective of this study was to investigate whether lifetime interpersonal violence experience is associated with COVID-19 and symptoms of post–COVID-19 condition among women in Kentucky, where both COVID-19 and lifetime interpersonal violence rates are higher than the national average. 46
Purpose
Wellness, Health & You (WHY) is an ongoing, longitudinal research project, formerly known as Kentucky Women’s Health Registry, developed in 2005 and renamed in 2017.47-49 We used data from the WHY COVID cohort to investigate the following hypothesis: women experiencing IPV, nonpartner sexual violence, or child physical and sexual abuse are more likely to develop COVID-19 and symptoms of post–COVID-19 condition than women with no lifetime interpersonal violence experience. We investigated associations between current pandemic-related stress and lifetime interpersonal violence experience as mediators for the hypothesized association between lifetime interpersonal violence experience and rates of COVID-19.
Methods
Data Source
WHY electronic surveys include several modules to capture a wide range of life experiences, social determinants of health, strategies for prevention of chronic conditions, and health concerns. During the pandemic, October 13, 2020–February 28, 2022, the WHY research team developed additional modules. These modules focused on the impact of the COVID-19 pandemic on both mental and physical health, adaptations to living and working during the pandemic, the use of COVID-19 prevention measures including receipt of vaccinations and boosters, development of COVID-19, and symptoms of post–COVID-19 condition. In this analysis, we focused on the impact of lifetime interpersonal violence experience on life challenges during the pandemic, the rate of self-reported COVID-19, and the risk of developing symptoms of post–COVID-19 condition.
Measures of Lifetime Interpersonal Violence Experience
The WHY baseline survey and the annual “Life Stressors” module included questions on exposure to lifetime interpersonal violence. Child physical and sexual abuse were measured with 2 items from the Adverse Childhood Experiences scale. 50 Adult nonpartner sexual violence and IPV were measured using items from the Centers for Disease Control and Prevention’s National Intimate Partner and Sexual Violence Survey. 51 In this study, we defined lifetime interpersonal violence experience as participant report of child physical or sexual violence or abuse, adult nonpartner sexual violence, and IPV (ie, physical, sexual, or psychological violence and stalking by an intimate partner). Adult violence experiences were measured in the past 12 months (Table 1).

Abbreviation: WHY COVID-19, Wellness, Health & You—COVID-19 Prevention.
Defined to include child physical or sexual abuse, adult nonpartner sexual violence, and intimate partner violence.
During the COVID-19 pandemic, October 13, 2020–February 28, 2022, the WHY research team developed new modules focused on the impact of the pandemic on both mental and physical health, adaptations to living and working during the pandemic, the use of COVID-19 prevention measures including receipt of vaccinations and boosters, development of COVID-19, and symptoms of post–COVID-19 condition.47-49
Child physical and sexual abuse were measured with 2 items from the Adverse Childhood Experiences scale. 50
Adult nonpartner sexual violence and intimate partner violence were measured using items from the Centers for Disease Control and Prevention’s National Intimate Partner and Sexual Violence Survey. 51
Measures of Pandemic-Related Symptoms of Distress, COVID-19 Vaccination, COVID-19, and Symptoms of Post–COVID-19 Condition
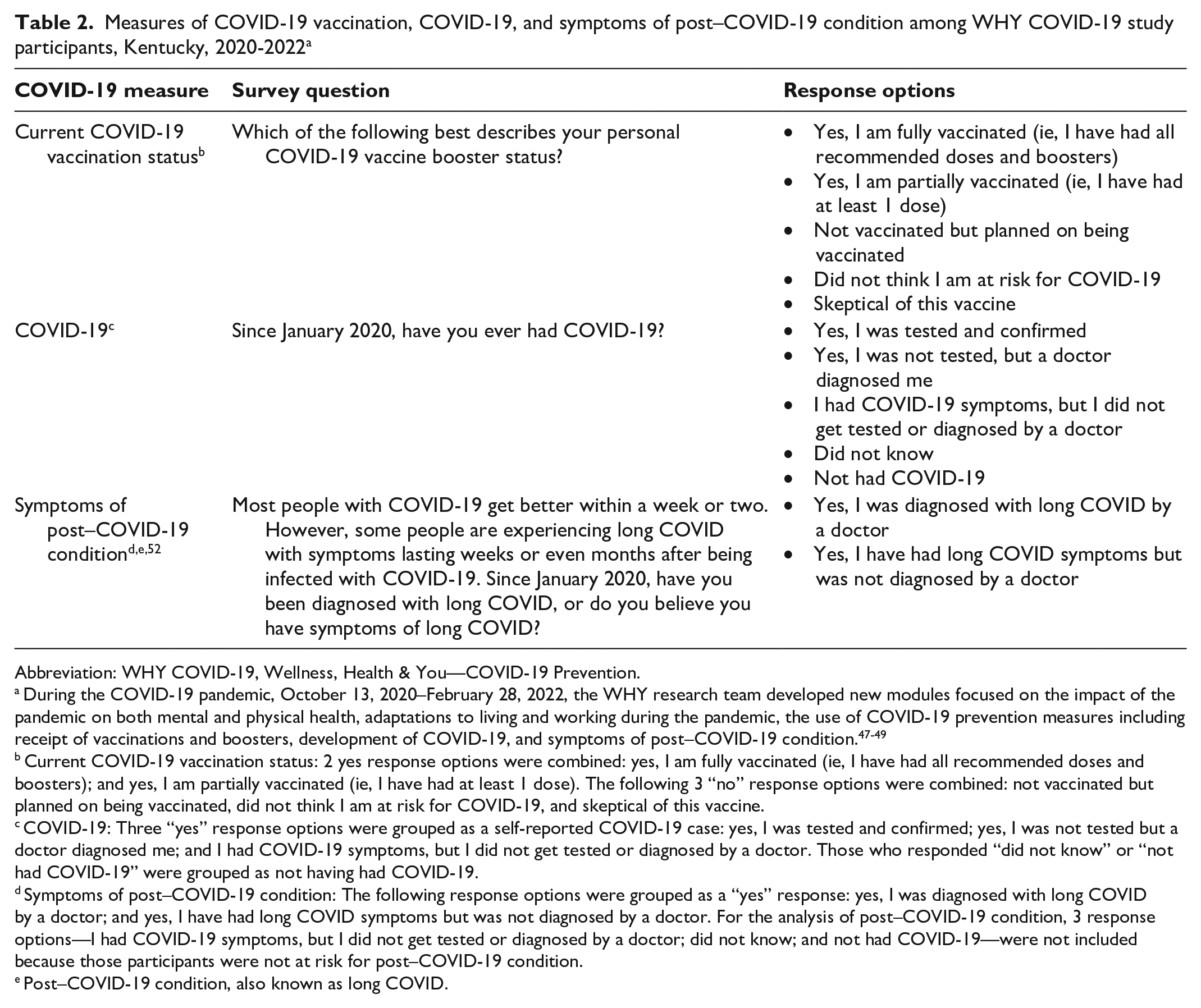
The effect of the pandemic on work or family life, rate of self-reported COVID-19, and risk of symptoms of post–COVID-19 condition was measured using items from the existing COVID-19 Participant Experience survey conducted by the National Institutes of Health All of Us Research Program 52 (Table 2).
Measures of COVID-19 vaccination, COVID-19, and symptoms of post–COVID-19 condition among WHY COVID-19 study participants, Kentucky, 2020-2022 a
Abbreviation: WHY COVID-19, Wellness, Health & You—COVID-19 Prevention.
During the COVID-19 pandemic, October 13, 2020–February 28, 2022, the WHY research team developed new modules focused on the impact of the pandemic on both mental and physical health, adaptations to living and working during the pandemic, the use of COVID-19 prevention measures including receipt of vaccinations and boosters, development of COVID-19, and symptoms of post–COVID-19 condition.47-49
Current COVID-19 vaccination status: 2 yes response options were combined: yes, I am fully vaccinated (ie, I have had all recommended doses and boosters); and yes, I am partially vaccinated (ie, I have had at least 1 dose). The following 3 “no” response options were combined: not vaccinated but planned on being vaccinated, did not think I am at risk for COVID-19, and skeptical of this vaccine.
COVID-19: Three “yes” response options were grouped as a self-reported COVID-19 case: yes, I was tested and confirmed; yes, I was not tested but a doctor diagnosed me; and I had COVID-19 symptoms, but I did not get tested or diagnosed by a doctor. Those who responded “did not know” or “not had COVID-19” were grouped as not having had COVID-19.
Symptoms of post–COVID-19 condition: The following response options were grouped as a “yes” response: yes, I was diagnosed with long COVID by a doctor; and yes, I have had long COVID symptoms but was not diagnosed by a doctor. For the analysis of post–COVID-19 condition, 3 response options—I had COVID-19 symptoms, but I did not get tested or diagnosed by a doctor; did not know; and not had COVID-19—were not included because those participants were not at risk for post–COVID-19 condition.
Post–COVID-19 condition, also known as long COVID.
Statistical Analyses
Participants (n = 1096) in the current WHY cohort who completed both the COVID-19 module and the questions on lifetime interpersonal violence were eligible for inclusion in the analysis. We excluded as missing 158 participants who had not completed the previously launched WHY module that included items on violence. Those not completing this module were older (mean age, 68.6 y) and significantly less likely to be working (P = .005) than those included in the current analysis (mean age, 59.4 y; t = 5.30; P < .001); we found no differences between the 2 groups based on education, race, or having COVID-19. The analytic sample included 938 participants.
We used the Mantel–Haenszel χ2 test using a 2-tailed P value to investigate associations between lifetime interpersonal violence experience and demographic characteristics. In selecting possible confounders, we considered demographic characteristics that might increase COVID-19 risk, including whether participants were currently working or retired and education level as potential indicators of having the option to work remotely or not. The small number of participants with symptoms of post–COVID-19 condition (n = 43) did not allow robust modeling with multiple potential confounders. We examined pandemic-related stressors as potential mediators of the association between lifetime interpersonal violence experience and COVID-19 outcomes.
We estimated rates of developing COVID-19 and symptoms of post–COVID-19 condition in separate log-binomial models, with lifetime violence as the primary exposure, using generalized linear modules (PROC GENMOD, link-log, dist-bin, type3 in SAS version 9.4; SAS Institute Inc). We estimated the association between COVID-19 and lifetime interpersonal violence experience by using unadjusted rate ratios (RRs) and adjusted RRs (ARRs) and 95% CIs. We also explored symptoms of distress as potential mediators for the effect of lifetime interpersonal violence experience on COVID-19 and symptoms of post–COVID-19 condition.
Ethics
This project was approved by the University of Kentucky Institutional Review Board (IRB). All participants provided informed consent prior to participating in the study. All surveys were completed electronically by using a computer, smartphone, or tablet. Consent language indicated that participants could choose not to complete specific questions. Participants were encouraged to complete the survey in a private location. Lastly, information on national domestic violence or sexual resources was provided to all participants at the end of this survey module (IRB #43533).
Results
Lifetime Interpersonal Violence Experience
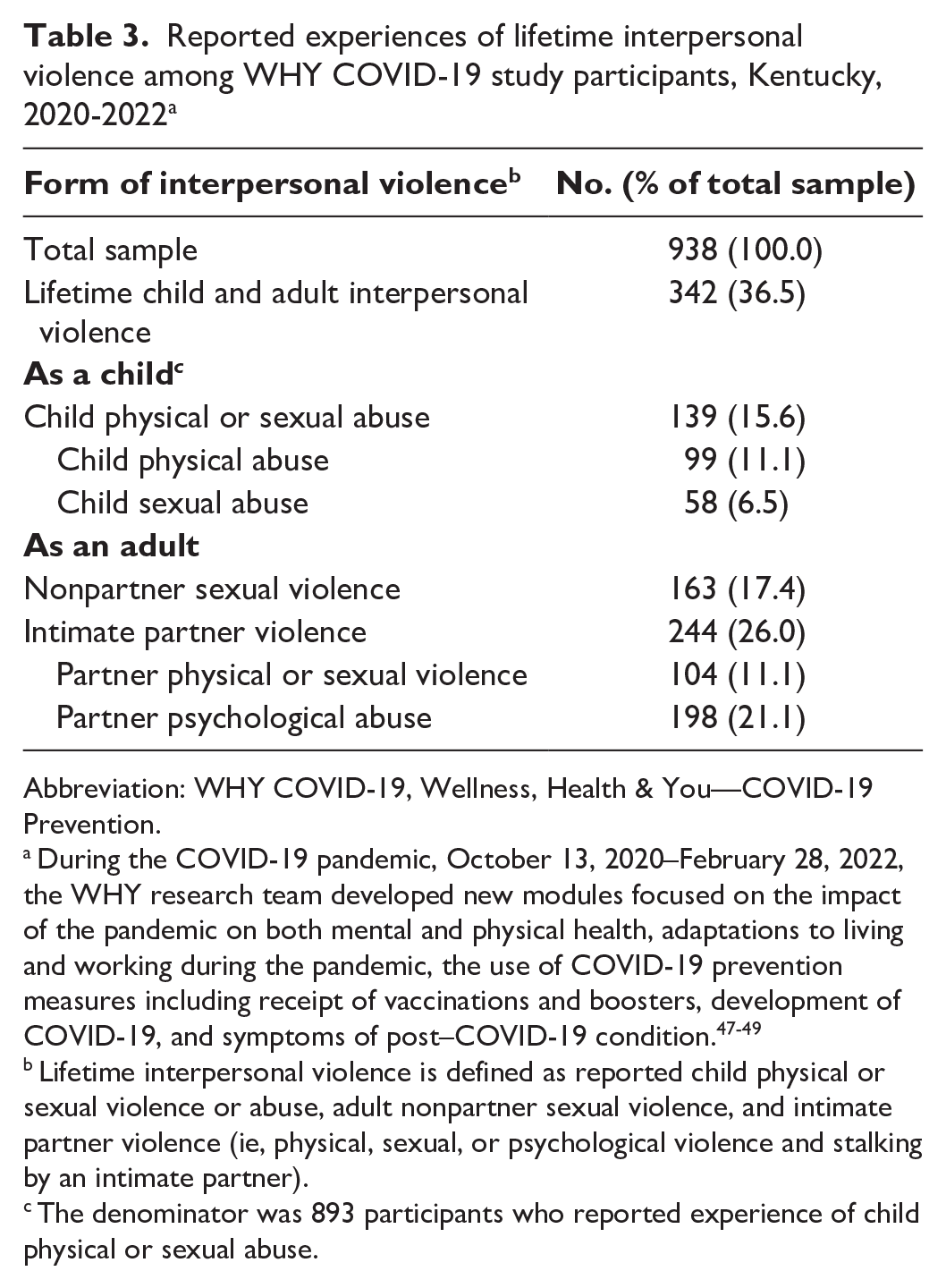
A total of 5431 invitations were sent to current WHY cohort participants from October 13, 2020, through February 28, 2022, and 938 participants completed the WHY COVID-19 survey. The invitations included those who may not have been active in the WHY cohort for some time. More than 1 in 3 women participating in the WHY COVID-19 survey (342 of 938; 36.5%) reported experiences characterizing lifetime interpersonal violence (Table 3). Experiences of child physical or sexual abuse were reported by 15.6% of participants (139 of 893 participants who completed the child abuse questions), and 17.4% (163 of 938) reported experiences of nonpartner sexual violence as adults aged ≥18 years. More than one-quarter of participants (n = 244; 26.0%) disclosed experiences of physical or sexual (11.1%; n = 104) or psychological (21.1%; n = 198) IPV. More than one-third of participants (342 of 938; 46.5%) who experienced interpersonal violence experienced ≥2 forms during their lifetime.
Reported experiences of lifetime interpersonal violence among WHY COVID-19 study participants, Kentucky, 2020-2022 a
Abbreviation: WHY COVID-19, Wellness, Health & You—COVID-19 Prevention.
During the COVID-19 pandemic, October 13, 2020–February 28, 2022, the WHY research team developed new modules focused on the impact of the pandemic on both mental and physical health, adaptations to living and working during the pandemic, the use of COVID-19 prevention measures including receipt of vaccinations and boosters, development of COVID-19, and symptoms of post–COVID-19 condition.47-49
Lifetime interpersonal violence is defined as reported child physical or sexual violence or abuse, adult nonpartner sexual violence, and intimate partner violence (ie, physical, sexual, or psychological violence and stalking by an intimate partner).
The denominator was 893 participants who reported experience of child physical or sexual abuse.
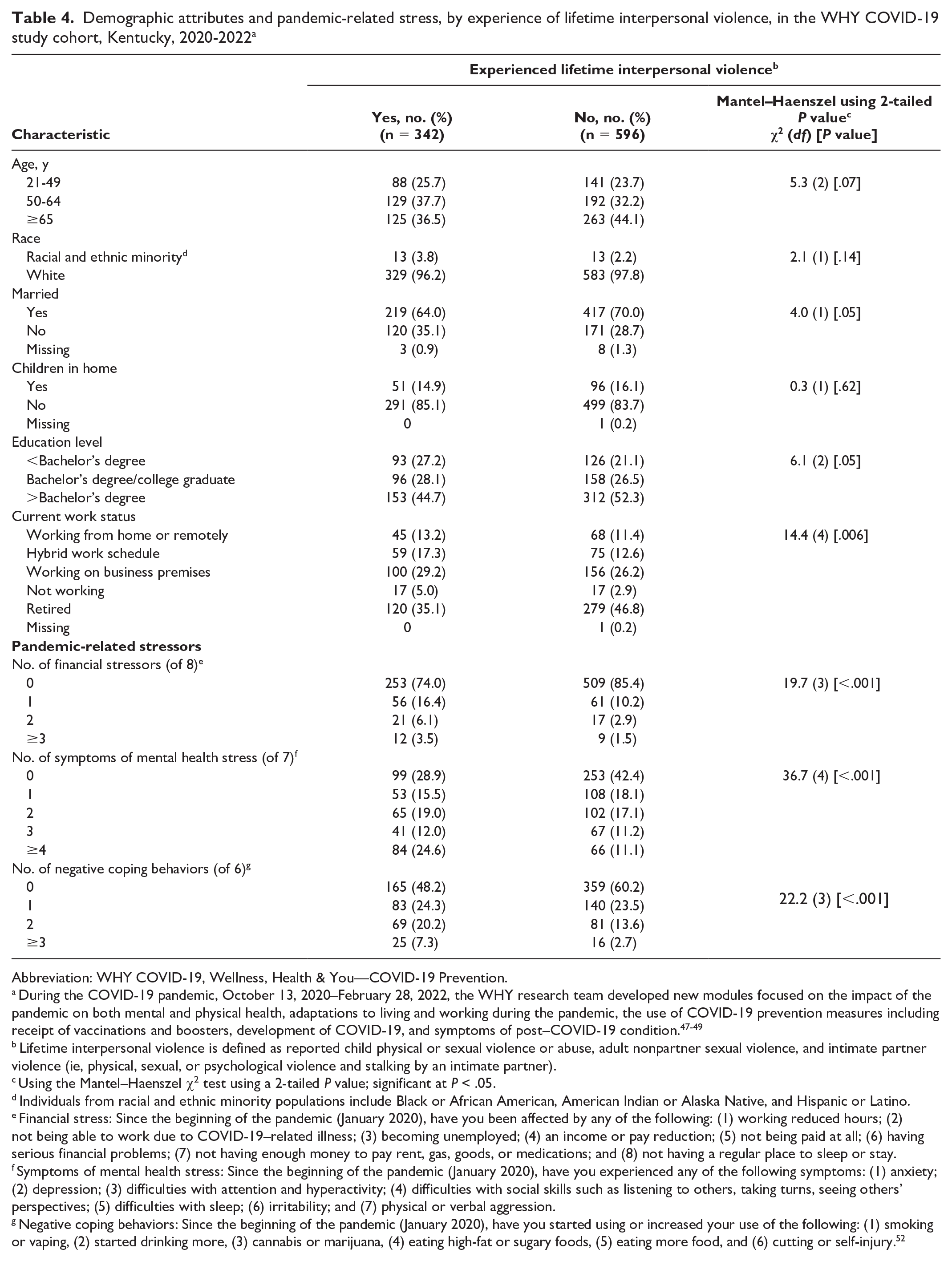
Women who had experienced lifetime interpersonal violence were significantly less likely to be currently married or retired and had significantly lower levels of education than those who had no lifetime interpersonal violence experience (Table 4). Compared with women who had never experienced interpersonal violence, those who had experienced lifetime interpersonal violence disclosed significantly more financial challenges (P < .001), more symptoms of mental health challenges (P < .001), and more negative coping strategies (P < .001). Because financial, mental health, and negative coping strategies were significantly correlated, only the number of mental health stressors was included as a mediator (Table 4).
Demographic attributes and pandemic-related stress, by experience of lifetime interpersonal violence, in the WHY COVID-19 study cohort, Kentucky, 2020-2022 a
Abbreviation: WHY COVID-19, Wellness, Health & You—COVID-19 Prevention.
During the COVID-19 pandemic, October 13, 2020–February 28, 2022, the WHY research team developed new modules focused on the impact of the pandemic on both mental and physical health, adaptations to living and working during the pandemic, the use of COVID-19 prevention measures including receipt of vaccinations and boosters, development of COVID-19, and symptoms of post–COVID-19 condition.47-49
Lifetime interpersonal violence is defined as reported child physical or sexual violence or abuse, adult nonpartner sexual violence, and intimate partner violence (ie, physical, sexual, or psychological violence and stalking by an intimate partner).
Using the Mantel–Haenszel χ2 test using a 2-tailed P value; significant at P < .05.
Individuals from racial and ethnic minority populations include Black or African American, American Indian or Alaska Native, and Hispanic or Latino.
Financial stress: Since the beginning of the pandemic (January 2020), have you been affected by any of the following: (1) working reduced hours; (2) not being able to work due to COVID-19–related illness; (3) becoming unemployed; (4) an income or pay reduction; (5) not being paid at all; (6) having serious financial problems; (7) not having enough money to pay rent, gas, goods, or medications; and (8) not having a regular place to sleep or stay.
Symptoms of mental health stress: Since the beginning of the pandemic (January 2020), have you experienced any of the following symptoms: (1) anxiety; (2) depression; (3) difficulties with attention and hyperactivity; (4) difficulties with social skills such as listening to others, taking turns, seeing others’ perspectives; (5) difficulties with sleep; (6) irritability; and (7) physical or verbal aggression.
Negative coping behaviors: Since the beginning of the pandemic (January 2020), have you started using or increased your use of the following: (1) smoking or vaping, (2) started drinking more, (3) cannabis or marijuana, (4) eating high-fat or sugary foods, (5) eating more food, and (6) cutting or self-injury. 52
COVID-19 Vaccination Status, COVID-19, and Symptoms of Post–COVID-19 Condition
Almost all (91.0%; 854 of 938) survey participants reported receiving COVID-19 vaccinations, including a booster, from January 2020 through February 2022. One-quarter of participants (234 of 938; 24.9%) reported having COVID-19.
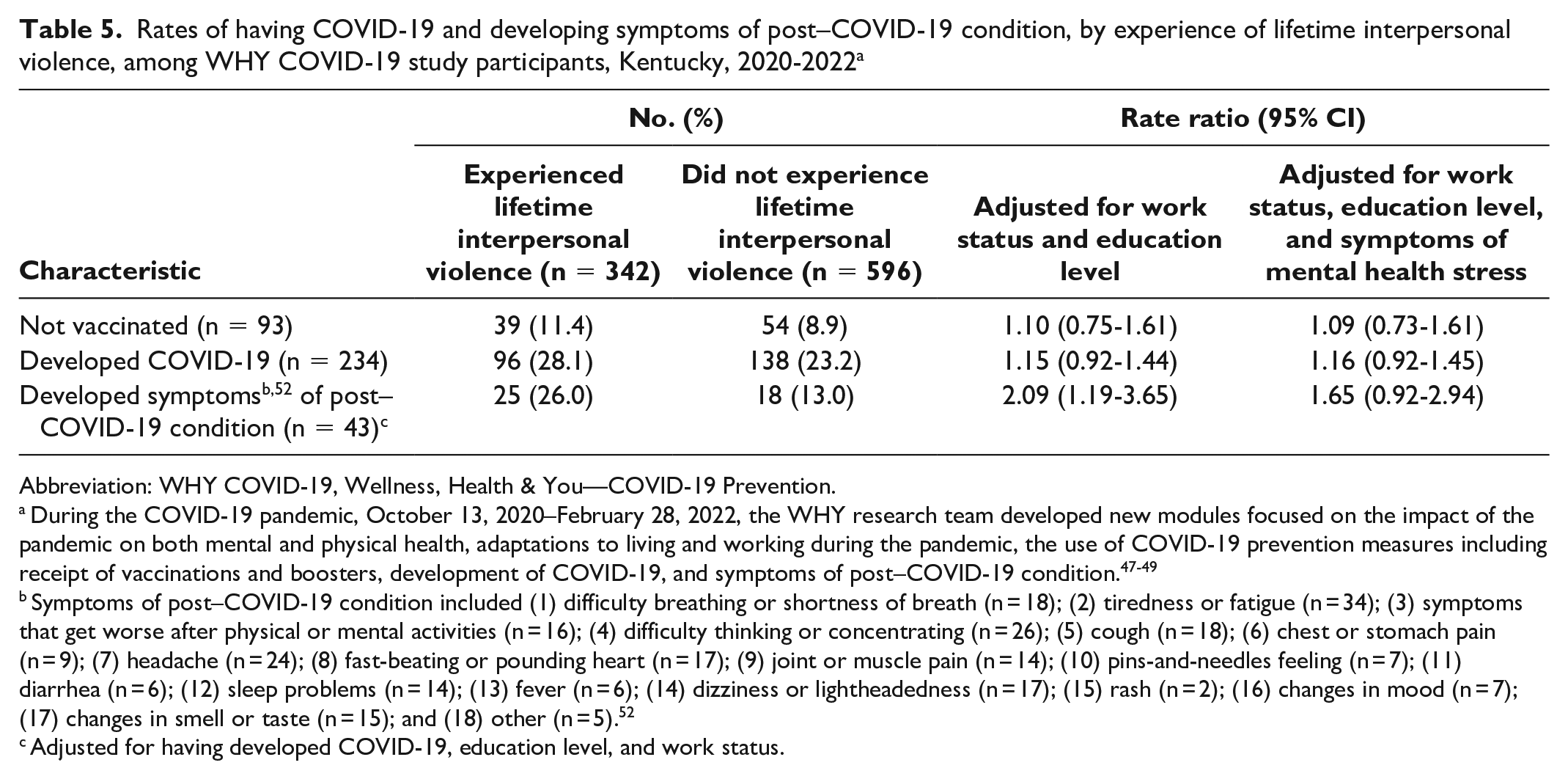
After adjusting for education and current work status, lifetime interpersonal violence experience was not significantly associated with remaining unvaccinated or having COVID-19 from January 2020 through February 2022 (Table 5). However, the rate of developing symptoms of post–COVID-19 condition was more than 2-fold higher among women with a history of lifetime interpersonal violence experience than among women with no such history (RR = 2.09; 95% CI, 1.19-3.65) after adjusting for having COVID-19, education level, and current work status. When symptoms of mental health stressors were added to the model, lifetime interpersonal violence experience was no longer significantly associated with developing symptoms of post–COVID-19 condition (aRR = 1.65; 95% CI, 0.92-2.94) nor having COVID-19.
Rates of having COVID-19 and developing symptoms of post–COVID-19 condition, by experience of lifetime interpersonal violence, among WHY COVID-19 study participants, Kentucky, 2020-2022 a
Abbreviation: WHY COVID-19, Wellness, Health & You—COVID-19 Prevention.
During the COVID-19 pandemic, October 13, 2020–February 28, 2022, the WHY research team developed new modules focused on the impact of the pandemic on both mental and physical health, adaptations to living and working during the pandemic, the use of COVID-19 prevention measures including receipt of vaccinations and boosters, development of COVID-19, and symptoms of post–COVID-19 condition.47-49
Symptoms of post–COVID-19 condition included (1) difficulty breathing or shortness of breath (n = 18); (2) tiredness or fatigue (n = 34); (3) symptoms that get worse after physical or mental activities (n = 16); (4) difficulty thinking or concentrating (n = 26); (5) cough (n = 18); (6) chest or stomach pain (n = 9); (7) headache (n = 24); (8) fast-beating or pounding heart (n = 17); (9) joint or muscle pain (n = 14); (10) pins-and-needles feeling (n = 7); (11) diarrhea (n = 6); (12) sleep problems (n = 14); (13) fever (n = 6); (14) dizziness or lightheadedness (n = 17); (15) rash (n = 2); (16) changes in mood (n = 7); (17) changes in smell or taste (n = 15); and (18) other (n = 5). 52
Adjusted for having developed COVID-19, education level, and work status.
Discussion
While women who had experienced lifetime interpersonal violence were not more likely to develop COVID-19 than women who had never experienced interpersonal violence, they were twice as likely to develop symptoms of post–COVID-19 condition. Our finding that lifetime interpersonal violence experience was no longer significantly associated with symptoms of post–COVID-19 condition after controlling for mental health stressors suggests that this measure of current distress may explain the observed increased rate of symptoms of post–COVID-19 condition associated with lifetime interpersonal violence experience. Our exploration of mental health stressors as a potential explanatory factor requires more thorough investigation.
We anticipated and found that women who had experienced lifetime interpersonal violence had a higher number of pandemic-related stressors that indicated more current financial and mental health challenges and more negative coping behaviors than women who had not experienced lifetime interpersonal violence. Results of our study indicate that having mental health stress, as a proxy for distress, was associated with both lifetime interpersonal violence experience and development of post–COVID-19 condition. This finding could indicate that mental health challenges may explain the observed association between lifetime interpersonal violence experience and symptoms of post–COVID-19 condition. Limited study power could also explain these findings.
Mental health stress could be a current indicator of trauma resulting from past violence. Chronic violent experiences that are characteristic of child abuse, nonpartner sexual violence, and IPV are known to increase the risk of PTSD. 30 Severe trauma exposure from experiencing violence (eg, IPV, sexual violence, child physical and sexual violence) can have lasting adverse effects on the HPA axis and immune response system.31,32,53 SARS-CoV-2 infection causing COVID-19 is associated with a strong chronic inflammatory response.31,43,54 Lifetime interpersonal violence experience may increase the risk of currently having symptoms of post–COVID-19 condition through HPA-axis dysfunction with immune dysregulation associated with physical or mental distress.
Findings from this investigation are consistent with existing research. The pandemic increased stress levels among family members and intimate partners. Statewide, stay-at-home lockdown and quarantine measures had negative effects on individuals’ mental health and disproportionately affected women. 55 Compared with men, women reported more experiences of worry and stress related to SARS-CoV-2 and high levels of anxiety, depression, and PTSD symptoms during the pandemic.56-61 Results of our study indicate that women with lifetime interpersonal violence experience are more likely to report financial challenges, mental health issues (eg, depression, anxiety, tension, aggression), and negative coping behaviors than women with no interpersonal violence experience. The negative mental health effects of the pandemic may contribute to increasing the PTSD symptoms (eg, anxiety, depression) and negative coping behaviors (eg, substance use, tobacco use) associated with experiences of lifetime interpersonal violence. The effects of experiences of lifetime interpersonal violence resulting in trauma or PTSD could elevate current pandemic-related symptoms of distress (eg, anxiety, depression, aggression), which could in turn lead to autoimmune system disorders such as post–COVID-19 condition after having COVID-19 among women who had experienced lifetime interpersonal violence.
More than one-third of this well-educated and relatively affluent sample disclosed experience with lifetime interpersonal violence. This finding speaks to the continuing need to ask patients about current and past experiences of interpersonal violence. Providing online and community resources to address lifetime interpersonal violence experience is key to reducing the impact of the interpersonal violence epidemic that predates COVID-19. The interpersonal violence prevention strategies developed and evaluated by public health providers and researchers are vital to reducing the impact of violence for our next generation. 62 These prevention strategies may include bystander empowerment and education programs and organizational policy and practice changes that promote safety and help-seeking behavior. 62 Prioritizing funding to identify effective interventions and comprehensively implement evidence-based interventions are concrete steps toward reducing the epidemic of violence. Public health programs can promote healthy relationships among couples that are focused on building and strengthening communication and conflict management skills during the pandemic.62,63
We observed that women with lifetime interpersonal violence experience may be at increased risk of developing symptoms of post–COVID-19 condition. The clinical implication of assessing the short- and long-term negative effects of the pandemic needs to prioritize people experiencing lifetime interpersonal violence because interpersonal violence alone has mental and physical health effects. Symptoms of post–COVID-19 condition may be another health condition linked to violence, possibly through stress or violence-associated trauma. Interventions can focus on reducing symptoms of PTSD from experiencing lifetime interpersonal violence with the help of a trauma-informed approach.
As noted, public health and medical professionals have a unique opportunity to ask patients about lifetime interpersonal violence experience. Many patients may not be ready to disclose current or past experiences of interpersonal violence; thus, health care providers may provide information to patients to acknowledge the physical and mental health effects of lifetime interpersonal violence. This universal information may be useful to patients, family, or friends. During the pandemic, health care providers played a critical role in identifying patients who may experience IPV in health care settings, providing counseling, and connecting those patients with needed social services, because many patients who experience IPV tend to seek help from informal sources (eg, family members, friends, neighbors) rather than formal services (eg, health care providers, social workers, counselors).64,65
Limitations
This study had several limitations. First, these preliminary findings were based on small numbers, specifically the 43 women of 234 who reported having COVID-19 who reported post–COVID-19 condition. These results must be interpreted as suggestive of an association between lifetime interpersonal violence experience and development of symptoms of post–COVID-19 condition in this highly educated sample of older women. Second, most women in this cohort were vaccinated and, therefore, may be at lower risk of experiencing symptoms of post–COVID-19 condition than people who are unvaccinated. Lifetime interpersonal violence rates in this cohort were lower than national estimates. 63 Our finding of lower rates of lifetime interpersonal violence could be explained by our narrow definition of lifetime interpersonal violence, which did not include child neglect, reproductive and sexual coercion, and economic and psychological IPV. Our observed lower rates of lifetime interpersonal violence experience could also indicate an underreporting of experiences with lifetime interpersonal violence. Third, our definition of symptoms of post–COVID-19 condition may be misclassified as other health issues or we may have been missing new symptoms of post–COVID-19 condition that were not characterized when this survey module was launched. With self-reported symptoms of post–COVID-19 condition alone, we did not have physician-verified diagnoses of post–COVID-19 condition. This research needs to be replicated in larger and more diverse populations, with infection status validated and symptoms of post–COVID-19 condition confirmed.
Our mediational analysis was undertaken to explore how lifetime interpersonal violence experience might increase the current risk of developing symptoms of post–COVID-19 condition through abbreviated measures of mental health challenges or stress. Our current stress mediational analysis was an attempt to understand how lifetime interpersonal violence experience might increase rates of symptoms of post–COVID-19 condition. Our measure of mental health symptoms included a checklist of current symptoms including anxiety and depression. Thus, our measurement of anxiety and depression may be misclassified, likely underestimated, with this nonstandard measurement approach. We did not have measures of lifetime interpersonal violence intensity and chronicity. These data could be useful to more fully elucidate mechanisms by which violence may increase the risk of symptoms of post–COVID-19 condition. Given the sample size, this analysis represents an exploration of the potential association between lifetime interpersonal violence experience and current symptoms of post–COVID-19 condition.
Conclusion
Results suggest that women with lifetime interpersonal violence experience may be more likely to develop symptoms of post–COVID-19 condition than women with no lifetime experiences of interpersonal violence. Symptoms of post–COVID-19 condition may be linked to lifetime interpersonal violence experience, possibly through stress or violence-associated trauma. Additional research with larger samples is needed to investigate this potential association and explore the mechanism by which lifetime interpersonal violence experience might increase the risk of symptoms of post–COVID-19 condition. Future studies that include people of diverse sociodemographic backgrounds are encouraged to identify underlying risk factors for post–COVID-19 condition, specifically lifetime experiences of interpersonal violence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through grant no. UL1TR001998. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH.