
Abstract
Background:
HPV vaccination coverage is important to prevent cervical cancer and other HPV-related diseases. This study estimated the vaccination coverage rate among adolescent schoolgirls aged 12–18 in Greece and identified factors affecting parental vaccination decisions.
Design and Methods:
A cross-sectional study was conducted from September 2021 to March 2022. A nationwide representative sample of 3205 parents/guardians of schoolgirls from 48 schools was selected through a probabilistic multistage sampling. Besides descriptive statistics, estimation, exploration and inferential methods were used, including 95% CI to estimate the vaccine rate, exploratory factor analysis to emerge the factors of HPV knowledge and multiple logistic regression analysis to identify the crucial parameters associated with vaccination, after adjusting for mutual confounding.
Results:
About 62.5% [95% CI: 61.1–63.9] of the girls were fully vaccinated. Mother’s HPV vaccination (OR [95% CI] = 2.90 [1.77, 4.73]), parental education level (OR [95% CI] = 2.50 [1.65, 3.79]), child’s attendance at the Upper secondary school (OR [95% CI] = 2.36 [1.83, 3.03]) and the level of HPV vaccine knowledge (OR [95% CI] = 1.59 [1.37, 1.84]) influenced parents’ decision to vaccinate their daughters.
Conclusions:
A significant increase in HPV vaccination coverage was recorded in Greece, compared to previous estimations. The identified determinants of parents’ vaccination decisions, especially HPV vaccine knowledge, can feed into targeted public health policies, to achieve the WHO’s goal to vaccinate 90% of adolescent girls by 2030. Policies may include the implementation of school-based awareness programmes for students and parents, state incentives for parents and expert recommendations for vaccination.
Keywords
Introduction
Cervical cancer is the fourth most common type of cancer among all types of cancer and the fourth leading cause of cancer deaths worldwide. In 2020, there were 604,127 cases worldwide and it was responsible for the death of 341,831 women. In Europe in 2020, 58,169 women were diagnosed with cervical cancer, of whom 25,989 died. 1 In Greece, during 2020, the crude incidence rate was 13.1 per 100,000 women, and the crude mortality rate was 5.31 per 100,000 women, thus making cervical cancer the 10th most common cancer in the country and third amongst those aged 15–44 years. 2 Yet cervical cancer is perhaps the most understood cancer and is almost 100% preventable. 3
Human papillomavirus (HPV) is the main causative factor for cervical cancer. 4 Specific types of the virus (16, 18, 31, 45, 33, 35, 39, 51, 52, 56, 58, 66, 68, 70) 5 with a high risk of causing cancer are together responsible for almost 5% of human cancers worldwide, the focus being on the two most prominent of these (HPV16 and 18). 6 HPV is also a causative factor for genital warts, benign morphomas created by specific low-risk types of the virus, such as types 6, 11, 42, 43 and 44. 7 It is estimated that about 5%–10% of all infected women develop a persistent infection of a high-risk type which can develop into precancerous and malignant conditions. 8
In August 2020, the World Health Organization (WHO) announced three main objectives of the global strategy to be achieved by 2030 to eradicate cervical cancer. The first of these objectives is that the vaccination coverage of girls up to 15 years of age reaches 90%. 9
HPV vaccination is considered one of the most effective preventive practices. 10 The safety of HPV vaccines is already documented, 11 and the reduction of cervical cancer through vaccination programmes has been documented 12 and proved to be cost effective. 13
HPV vaccination at the appropriate age, before the start of sexual life, significantly reduces the risk of a woman being diagnosed with intraepithelial lesions grade 2 or worse (CIN2+). 14
Despite the above documentation, there is still a large distance from the WHO target regarding global vaccination coverage and a great discrepancy between countries regarding vaccination coverage against HPV. 15 According to the WHO, 16 in 2021, global vaccination coverage with all doses of the HPV vaccine for girls up to 15 years was 15%. On a regional level, coverage ranged from 1% in Southeast Asia to 82% in Australia. In Europe, the rate was 27%. Among European countries, vaccination coverage ranged from 8% in Bulgaria to 94% in Portugal. Thus, one of the main challenges for public health authorities is to increase HPV vaccination coverage rates. 17
Greece has incorporated HPV vaccination into its national vaccination programme for children and adolescents, following a two-dose regimen. The vaccine is recommended for both girls and boys between the ages of 9 and 11 and is provided free of charge. If not administered within the recommended age range, a catch-up vaccination is available up to the age of 18, also in two doses. In such cases, the vaccine will remain available free of charge until the end of 2025. 18
Regarding vaccination coverage rates in Greece, the National Vaccination Committee estimates that the average vaccination coverage in the period 2017–2021 among girls was 55.4% for ages 11–18 and 43.8% for all ages. 19 Studies published during the last 3 years among non-representative samples in Greece estimated the percentage of coverage, ranging from 25.8% to 52.3%.14,18,20–23
Parental hesitancy has been suggested as a factor contributing to low vaccination coverage, potentially linked to the lack of a national school-based vaccination programme. Parents’ vaccine hesitancy remains 1 of 10 global threats, according to the WHO. 24
On the other hand, factors positively associated with parents’ decision to vaccinate their daughters include: (a) a doctor’s recommendation and parents’ trust in healthcare providers 25 ; (b) mothers’ as opposed to fathers’ responsibility to decide to vaccinate the child 26 ; (c) parents’ beliefs, attitudes and intentions for the vaccine 27 ; (d) insurance and coverage of vaccination costs 28 ; (e) parents’ history of risk or illness from HPV 29 ; (f) parents’ HPV knowledge and awareness 29 ; and (g) socio-demographic factors such as residency (i.e. urban vs rural) and the age of the child. 30 All the above factors highlighted by the previous research were included and measured in our study. Nevertheless, in the current paper, we report data referring only to factors related to actual vaccination until the data collection time and not to those influencing parents’ intention to vaccinate their daughters in the future.
Given the lack of relevant nationwide studies and fully recorded data from the National Health System in Greece, the purpose of this study was to estimate the rate of vaccination coverage against HPV throughout Greece among girls aged 12–18 years and record the factors that influence parents’ decision to vaccinate their daughters. Although HPV vaccination is important for both girls and boys, this study focused only on girls, as until March 2022 the HPV vaccine was not available to boys in Greece through the National Vaccination Programme.
Design and methods
Study design and sampling
Parental studies constitute a common method of estimating vaccination rates. 31 The current cross-sectional study was conducted between September 2021 and March 2022 among a representative sample of parents/guardians of schoolgirls aged 12–18 from all types of secondary schools in Greece. Secondary education in Greece lasts 6 years and includes two levels: High School (lower secondary) and Lyceum (Upper secondary school), each comprising three grades (A, B, and C). Students typically attend High School from ages 11–12 to 14–15, and Upper secondary school from 15–16 to 17–18.
A national officially published list of all types of secondary schools in Greece (3543 schools in 2019), with a total of 312,363 schoolgirls, was used as the sampling framework. The units of investigation were the Regional Educational Directorate (RED; primary). RED is a decentralized administrative body of the Ministry of Education responsible for overseeing and coordinating educational matters within a specific geographic region of the country. Greece has 13 REDs. Τhe school unit (secondary), and the parent/guardian of each schoolgirl (tertiary).
A probabilistic multistage cluster sampling technique was applied as follows: Stage 1: stratified sampling by RED based on the number of schoolgirls; Stage 2: cluster randomized sampling with unequal cluster sizes (school was a cluster); and Stage 3: single cluster sampling (all schoolgirls were included).
Participants
A sample of 6329 girls from 56 secondary schools were invited to participate in the study (a = 0.05, 0.8 power, difference at 1.22 of vaccination) and received the equivalent closed envelopes with the questionnaire and the guidelines for completing it to hand over to their parents. An empty envelope was also included for the parents to put the completed questionnaire and return it through their girls. There was no guidance on which of the parents/guardians should be given the envelope or who should complete the questionnaire. In total, 3205 envelopes were returned (response rate: 50.6%) from 48 schools, accounting for 4697 girls, given that some families had more than one daughter. Written informed consent was obtained from the legally authorized representatives of the MINOR participants for this study. Eight schools (14.2%; four public peripherals, two private, two ecclesiastical) did not participate due to the school directors’ denial and the late granted permission from the Greek Ministry of Education for the ecclesiastical schools.
Study tool
An anonymous self-completed questionnaire constructed by the first three authors was used (See Supplement). The first section consisted of seven questions exploring parents’ demographics and family characteristics. The second section consisted of 13 questions related to parents’ HPV and vaccine knowledge, daughters’ vaccination status and parents’ intention to vaccinate their daughters. In this section, participants were instructed to indicate whether each statement was “right,” “wrong,” or “don’t know.” The third section consisted of 13 questions that explored parents’ reasons for not vaccinating, and their attitudes, beliefs and feelings about vaccination derived from the Capability, Opportunity, and Motivation Behaviour (COM-B) model, following COM-B developers’ guidelines. 32 More specifically, the questions represented the Physical and Psychological Capability (C), Physical and Social Opportunity (O), Automatic and Reflective Motivation (M) components, which are the basic and necessary components to produce a behaviour (B). Most questions were closed-ended or mixed and they were in various formats (e.g. multiple choice, Likert scale). Although the questionnaire was not subjected to full formal validation procedures, several steps were taken to ensure its appropriateness and reliability: A pilot implementation was conducted with a sample of 30 parents, leading to amendments that improved clarity and comprehension. Face validity was established through expert review, during which experts rated the relevance of each item. Internal consistency of the tool was high (Cronbach’s alpha = 0.789), and content validity was supported by pilot data from parents. Furthermore, exploratory factor analysis confirmed the internal structure of the knowledge items, supporting the robustness of the tool. These steps, although not constituting full validation, provided adequate assurance of the questionnaire’s suitability for the purposes of this study.Ethical approval and data collection
The study was approved by the Greek Ministry of Education (No 90032/ΓΔ4/23-7-2021) and the Ethics Committee of the University of West Attica (No 37937/11-5-2021). Following the approvals, email notifications and subsequent reminders were sent to the selected schools to organize the first author’s (AE) visits to the schools to distribute the envelopes with the questionnaires, the consent forms to be signed by the participating parents and the empty envelope for their return. A telephone communication confirmed the scheduled visit. Before the distribution of the envelopes, the first author had a 15–20-min informative discussion with the students about the aim and the significance of the study, particularly stressing the importance of parents’ participation. The sealed return envelopes were placed in a designated collection box located in the Headteacher’s office at the school, where they were remained throughout the collection period (approximately 1 week). At the end of this period, the box was sent to the first author via courier service. This process ensured that all envelops were securely collected and delivered to the research team.
Statistical analysis
The statistical analyses were performed using the statistical software SPSS, version 2022. Before analysis, data processing techniques were applied to ensure consistency and facilitate interpretation. Specifically, variables were recoded where necessary so that higher values reflected higher levels of knowledge. Composite scores were then calculated to represent participants’ knowledge regarding the HPV virus and vaccine, by aggregating the relevant items through computation of the mean score per construct. Exploratory factor analysis (EFA) was conducted to examine the internal structure of the knowledge items and confirm unidimensionality, which supported the aggregation.Descriptive statistics and frequency measurement were used to describe the demographic characteristics of the sample, knowledge and vaccination data. Statistical significance was defined at the 5% level. Inferential techniques were used to estimate the vaccine ratio and its 95% CI.
Initial items for virus and vaccine knowledge were guided by a literature review. 33 Face validity was established from the experts’ review and appropriate feedback was received based on their expertise. Experts were asked to rate the relevance of each item using a 5-point Likert scale (1 = not relevant to 5 = highly relevant). Internal consistency was high (Cronbach’s alpha = 0.789). Content validity was conducted using pilot data from parents. Exploratory factor analysis (EFA) was applied in the virus (10 items – item B4.4 was excluded) and vaccine knowledge (nine items) items to examine the internal structure of the questionnaire 34 and provide the appropriate factor scores as independent variables for further analysis (Supplemental Tables 1 and 2). A Principal Component Analysis and Oblimin rotation method were used to handle potentially non-normal data and to recover weak factors. 35 Kaiser–Meyer–Olkin was used to assess sampling adequacy, for conducting the EFA. 36 The following criteria were used for extracting the number of factors. First Kaisers’ criterion, 37 to identify factors with eigenvalues greater than 1.0; then the % of total variability, the scree plot criterion 38 by plotting the eigenvalues on a curve and seeing the point at which the curve stops decreasing and flattens; finally, the Parallel analysis used to provide further evidence to decide the number of final factors and interpretability criteria. 39
Odds ratios for vaccination and socio-demographic variables were also calculated, after recoding them into dichotomous variables, to examine their significance on vaccination. Then multiple logistic regression analysis was applied to identify factors after adjusting for mutual confounding. Bartlett’s Test of Sphericity was used to test the correlation of variables entered in EFA. Hosmer–Lemeshow test was used to test for goodness of fit for the logistic regression model.
The manuscript was prepared according to the STROBE (strengthening the reporting of observational studies in epidemiology) statement.
Results
About 6329 parents received closed envelopes with the invitation to the survey and research material. Of these, 3205 parents signed the consent form and participated in the study answering and returning the questionnaire in a sealed envelope (response rate: 50.6%), corresponding to 4697 daughters. There was no exclusion criterion for any parent who had an 11–18-year-old daughter.
Table 1 shows the demographic characteristics of the participants. The mean age was 45.6 years [SD 5.0, range 27–70 years]. The majority (93.2%) was female, had finished secondary education (57.6%), lived in a city (87.2%), worked as a civil/private servant (59.2%), identified the financial status of their family as medium (72.9%), and had only one daughter (60%).
Participants’ demographic characteristics (N = 3205).

The numbers in the table may not sum to the totals due to missing data; The levels of missing data were small, ≤0.5% for most of the variables in Table 1, gender (n = 1), age (n = 12), educational level (n = 9), occupation (n = 13), financial status (n = 11), number of daughters (n = 12), except the place of residence (n = 229, 7.5%).
HPV vaccination coverage is presented in Table 2. Of the total of 4697 daughters, 2936 (62.5%) of girls were fully vaccinated, that is they had received two doses of the vaccine. Even higher rates (67.2%) were reported regarding those parents who had vaccinated their daughter with at least one dose.
HPV vaccination coverage in student population 12–18 years old in Greece (N = 4697).
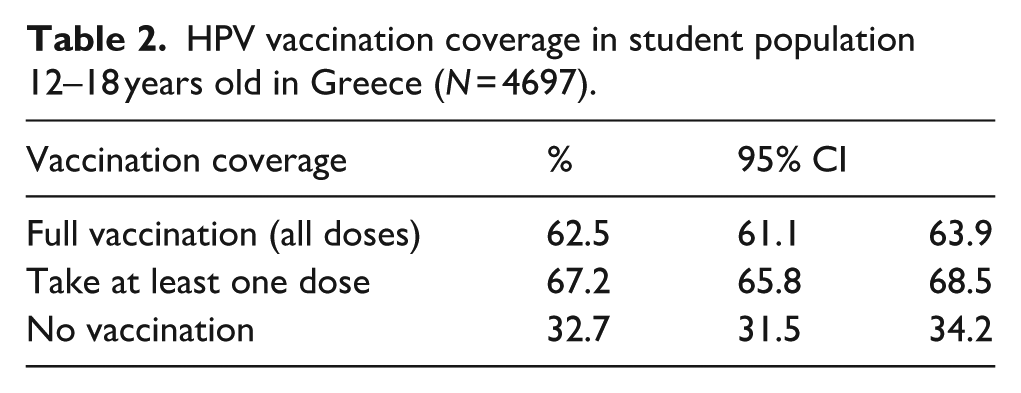
Table 3 shows data on subjects’ knowledge of HPV and the related vaccine. It seemed that participants answered the knowledge questions about both the virus and the vaccine correctly at very high rates: B2.4 (95.3%), B3.1 (91.7%), B4.2 (95.5%), B7.2 (75.7%), B7.4 (96%), B8.2 (96.6%).
Participants’ knowledge of human papillomavirus (HPV) and HPV vaccine (N = 3205).

C: correct answer; W: wrong answer.
The numbers/percentages under the “Right,” “Wrong,” “Don’t know” correspond to the number/percentage of people who selected each of the options. The numbers in the table may not sum to the totals due to missing data; the levels of missing data were small, for B1 (n = 24, 0.7%), and aware of HPV vaccine (n = 25, 0.8%); for the correct answers, B2.4 (n = 46, 1.4%), B3.1 (n = 66, 2.1%), B4.2 (n = 62, 1.9%), B7.2 (n = 1014, 31.6%), B7.4 (n = 199, 6.2%), B8.2 (n = 288, 9.0%). For the wrong answers the levels of missing were high, for Β.2.1 (n = 1261, 39.3%), B2.2 (n = 1295, 40.4%), B2.3 (n = 1275, 39.8%), B3.2 (n = 1240, 38.7%), B3.3 (n = 1195, 37.3%), B4.1 (n = 1255, 39.1%), B4.3 (n = 1249, 38.9%), B4.4 (n = 1350, 42.1%), B7.1 (n = 1312, 40.9%), B7.3 (n = 1349, 42,1%), B7.5 (n = 1295, 40.4%), B8.1 (n = 1442, 45%), B8.3 (n = 1497, 46,7%), B8.4 (n = 1533, 47.8%).
Factor analysis revealed new independent factors instead of the huge number of correlated variables for virus and vaccine knowledge. Regarding HPV virus knowledge, three factors emerged which explained 60.85% of the variance. Factor 1, “Core HPV knowledge” represented the correct knowledge of HPV transmission, HPV symptoms and the consequences of HPV. Factor 2, referred to as “Misconceptions about HPV consequences.” Finally, factor 3 addressed “Misconceptions about HPV transmission.” The results of Kaiser-Meyer-Olkin (KMO = 0.764) values and Bartlett’s Test of Sphericity [χ2 = 4625.97, p < 0.001] showed that factor analysis was well performed (Supplemental Table 1).
Regarding of the HPV vaccine knowledge, three factors emerged, explaining 57.33% of the variance. Factor 1 measured “Misconceptions about the age of vaccination,” factor 2 referred to the “Core vaccine knowledge” and factor 3 measured the “Misconceptions about vaccine benefits.” The results of Kaiser-Meyer-Olkin (KMO = 0.66) values and Bartlett’s Test of Sphericity [χ2 = 2065.081, p < 0.001] showed that the factor analysis was well performed (Supplemental Table 2). Τhe results of the exploratory factor analysis are consistent with those designed in the development of the questionnaire and overlap with the item-factor distribution defined in the original questionnaire for vaccination and virus knowledge scale.
Furthermore, for more clear results, the independent socio-demographics variables were recoded as dichotomous and their Odds ratios with vaccination were all significant.
Finally, a multiple logistic regression model was used to identify sociodemographic variables, as well as the virus and vaccine knowledge factors that could affect parental decisions for their daughter’s vaccination (Table 4).
Multiple logistic regression model for parents’ decision to vaccinate their daughters against HPV.

(R): recoded.
As can be seen in Table 4, after controlling for mutual confounders, only “School of daughters’ attendance,” “Parents’ age,” “Parents’ educational level,” “Maternal vaccination,” and the “Core vaccine knowledge” significantly predicted parents’ decision to vaccinate their daughters. More specifically, with one unit of increase in “Core vaccine knowledge” the odds of vaccination increase by a factor of 1.69 (OR [95% CI] = 1.69 [1.40, 2.03]). Furthermore, the odds of vaccination increase by a factor of 2.45 if one has a child at the Upper secondary school (this is indirectly related to the age of the children, meaning that the odds of being vaccinated increase by the age of the daughter; OR [95% CI] = 2.45 [1.88, 3.20]). In addition, the odds of a decision to vaccinate increases by a factor of 2.37 if the educational level of parents changes from High School to Upper secondary school (OR [95% CI] = 2.37 [1.52, 3.69]). Finally, the odds of a decision to vaccinate increase more than triple by a factor of 3.115 if the mother has been vaccinated (OR [95% CI] = 3.115 [1.857, 5.362]).
It is noticeable in Table 4 that “Core HPV knowledge” is not significant (p = 0.17), although it was significant (p = 0008) in Step 0 of regression (Supplemental Table 3), probably due to a complex correlational relationship with the “Core vaccine knowledge” variable. The Sobel test 40 (0.53) indicated that “Core vaccine knowledge” does not demonstrate a statistically significant mediating effect in the relationship between “Core virus knowledge” and vaccination decision (p = 0.5961).
Discussion
The main finding of our study is that the estimation of full vaccination coverage against HPV of girls 12–18 years old in Greece, reaches 62.5%. Another finding is that the major factors that influence parents’ decision to vaccinate their daughters are the mother’s vaccination status, the school grade of the student, the parent’s educational level, the parent’s level of basic knowledge about the HPV vaccine and the age of the parents if they are over 40 years old.
In 2022, HPV vaccination coverage in girls up to 15 years old, in selected European countries was: Austria 53%, Bulgaria 9%, Denmark 82%, Finland 67%, France 42%, Germany 54%, Italy 61%, Sweden 85%. 16
Previous studies on the vaccination coverage against HPV in Greece have provided lower rates. More specifically, in 2016, within a sample of 500 female university students, the vaccination coverage rate was 29.4%. 41 In 2020, in another prospective study among 466 women, the percentage of vaccination coverage was 30%–35%. 21 In 2022, in a convenience sample of 883 adult men and women aged 17–35, the vaccination rate among women was 52.3%. 19 In addition, in another study in 2022, in a sample of 1000 parents of girls 11–18 years old, the percentage of fully vaccinated girls was 35%. 22 Finally, the National Vaccination Committee estimated that the full vaccination rate for ages 11–18 is 43.8%. 23 The current study was conducted on a nationally representative sample of parents from across Greece. The differences in vaccination rate observed compared to previous Greek studies may be attributed, at least in part, to the limited representativeness or the use of convenience sampling that those earlier studies. Even though our study recorded an increase in the vaccination coverage rate in Greece, this percentage is still significantly far from the goal set by the WHO whereby, by 2030, 90% of girls up to 15 years old all over the world should have been vaccinated against HPV. 9 This poses a challenge to Greek policymakers and actors to intensify their efforts to achieve the goal by increasing the awareness of parents and students, as well as health professionals.
Since the introduction of vaccines against HPV, plenty of studies have explored the factors that influence the acceptance and uptake of the vaccine and certified that awareness and knowledge about the virus and the vaccine were prerequisites for making informed decisions. 28 In our study, 92.9% of parents said that they were aware of the HPV infection and 95.8% were aware of the vaccine, similar to a previous Greek study (99.4% and 98.8%, respectively). 22
Our findings, similarly to those of previous studies, 29 showed that mothers who had already been vaccinated against HPV had 3.1 times greater odds of vaccinating their daughters than mothers who were not vaccinated. It might be the case that mothers’ own positive experience reduces hesitancy related to vaccine safety and strengthens their positive attitude towards their daughters’ vaccination.
HPV vaccine-related knowledge is a crucial factor guiding parents’ decision to vaccinate their daughters. In the current study, parents having high core vaccine knowledge and education level up to Upper secondary school were 1.7- and 2.4-times greater odds to vaccinating their daughters. Knowledge about the vaccine and prevention methods, as well as people’s educational level, can affect attitudes towards prevention methods for cervical cancer. 42
Previous studies have shown significant misconceptions among parents, even among those who are informed about the virus, 17 although there is evidence that the uptake of vaccination increases when the target population is well informed about the risks and benefits. 43 Our study confirmed the above findings, as it showed that around one in four parents did not know whether the virus was transmitted by droplets or by kissing, while a similar percentage wrongly considered the age of 19–32 years as the recommended age of vaccination.
HPV knowledge was significant only at the initial step of the regression analysis, while its significance was lost at the following step, possibly due to the effect of the vaccine knowledge. However, the Sobel test indicated that “Core vaccine knowledge” does not demonstrate a statistically significant mediating effect in the relationship between “Core virus knowledge” and vaccination decision (p = 0.5961). There may be a more complex correlation between these variables, which warrants further investigation in future studies.
As shown by the results, the school that the schoolgirls attended (High School or Upper secondary school) had a very strong effect on vaccination. This finding is probably linked to the age of the parents, since our study also showed that parents who were old than 40 years had 1.4 times greater odds to have vaccinated their daughters. Similar finding has been appeared to previous studies, 44 confirming that the mature age of parents acts as a motivating factor for them to decide the vaccination of their daughters. This may be due to the possible perception of parents that they could delay the start of HPV vaccinations, as it is a disease that is primarily sexually transmitted and is obviously related to both the age of the daughters and their own.
It is worth noting that Greece has implemented a National Cervical Cancer Prevention Programme since January 2023. Under this programme, women aged 21–65 are eligible for free cervical cancer screening. Based on age and clinical criteria, participants are offered a gynaecological examination and either a Pap test or HPV-DNA test. Appointments are pre-scheduled, and women are notified via SMS. The participation rate in the programme currently stands at 72.9%. This study is the first in Greece to use a representative sample of Greek parents to estimate HPV vaccination coverage, applying the methodological model of sampling used by the Hellenic Statistical Authority for national health surveys. Consequently, it accurately approximates the level of HPV vaccination coverage of girls aged 11–18 in Greece and sets a significant policy starting point.
The findings of the current study are likely to have an impact on the reorientation of public health policies in Greece to further increase vaccination coverage. Additionally, it offers the opportunity for international organizations to be informed for the first time with reliable data, as no such data are so far available for our country. With the availability of these data, the relevant bodies will be able to set the appropriate goals for increasing vaccination coverage against HPV in Greece through specific public health policies and schedules.
Limitations of the study
This study has some limitations. A 14% non-participation rate at the school level raises the possibility that parental views in non-participating schools may differ. Additionally, 49% of eligible parents within participating schools did not complete the survey. Parents who had already vaccinated their daughters may have been more likely to participate, potentially skewing the sample towards pro-vaccination attitudes. However, the study still captured data on 1535 unvaccinated girls (32.7% of the total in participating schools), suggesting that a broad spectrum of parental perspectives—including vaccine-hesitant views—was represented.
A key limitation of this study is the response pattern observed in the knowledge t items: many participants answered only the correct statements, while skipping the incorrect ones, despite explicit instructions to complete all items. This led to disproportionately high missing data for distractor items due to systematic response behaviour rather than random nonresponse. To address this, we calculated core knowledge scores using only the correctly formulated items, which had minimal missing data. While this preserved data interpretability, it limited the scale’s psychometric completeness and underscores the need for future refinement. On the other hand, the use of a questionnaire not subjected to full formal validation procedures may introduce measurement bias and limit the interpretability of the results.
Lastly, another limitation of the study is that it mainly focuses on the role of parents’ knowledge about HPV and the vaccine in their decision to vaccinate their daughters, without considering other influential factors such as attitudes, religiosity, or acceptance of vaccines.
Conclusion
In this national representative Greek study, HPV vaccination coverage among girls aged 12–18 years was estimated at 62.5%. This figure is higher than previously reported in smaller or non-representative studies, but still remains below the WHO target of 90% coverage among girls up to age 15 by 2030. Parental decision to vaccinate was associated with maternal vaccination status, parental education, daughters’ school level, parents’ age and knowledge of the HPV vaccine. While progress has been made in HPV vaccination coverage in Greece, important gaps remain. Addressing these gaps may benefit from initiatives that strengthen vaccine-related knowledge among parents, improve communication strategies and support healthcare professionals in providing clear recommendations. Future research could further examine additional factors, such as attitudes, cultural influences and healthcare access, that were not within the scope of this study but may play a role in vaccination uptake.
Significance for public health
This study makes a valuable contribution to public health by providing, for the first time, an accurate estimate of full HPV vaccination coverage among girls aged 11–18 in Greece, based on a nationally representative sample. This estimate offers a clear picture of the current situation and highlights two key points. First, it demonstrates that recent health policies have had a positive impact, contributing to a significant increase in vaccination coverage. Second, it provides a foundation for refining the national strategy to achieve the WHO target. This strategy can be shaped by the factors identified in the study as influencing parents’ decisions to vaccinate their daughters, pointing to an effective combination of policies needed to reach this goal in Greece.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251388594 – Supplemental material for Vaccination coverage against HPV in a national representative sample of schoolgirls aged 12–18 years in Greece and core knowledge factors in parents’ decision to vaccinate their daughters
Supplemental material, sj-docx-1-phj-10.1177_22799036251388594 for Vaccination coverage against HPV in a national representative sample of schoolgirls aged 12–18 years in Greece and core knowledge factors in parents’ decision to vaccinate their daughters by Apostolos Efkarpidis, George Koulierakis, Anastasia Papastilianou, Antonia Paschali and Kyriakoula Merakou in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251388594 – Supplemental material for Vaccination coverage against HPV in a national representative sample of schoolgirls aged 12–18 years in Greece and core knowledge factors in parents’ decision to vaccinate their daughters
Supplemental material, sj-docx-2-phj-10.1177_22799036251388594 for Vaccination coverage against HPV in a national representative sample of schoolgirls aged 12–18 years in Greece and core knowledge factors in parents’ decision to vaccinate their daughters by Apostolos Efkarpidis, George Koulierakis, Anastasia Papastilianou, Antonia Paschali and Kyriakoula Merakou in Journal of Public Health Research
Footnotes
Acknowledgements
This article is based on research conducted in the framework of the implementation of a doctoral dissertation. The authors are grateful to those who contributed to its implementation as a whole, and especially to the parents from all over Greece who answered the questionnaire.
Author contributions
Conceived and designed the study: Apostolos Efkarpidis, George Koulierakis. Performed the data collection: Apostolos Efkarpidis. Facilitated acquisition of data: Apostolos Efkarpidis. Analysed the data: Anastasia Papastilianou, Apostolos Efkarpidis. Wrote the paper: Apostolos Efkarpidis, George Koulierakis, Anastasia Papastilianou. Critically revised the manuscript for important intellectual content: All the authors.
Funding
The authors disclosed receipt of the following financial support for the publication of this article: This study did not receive any specific grants from public, commercial or non-profit funding bodies. The cost for the publication wasbe covered by the Special Research Account of the University of West Attica.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data of this study are available from the first author upon reasonable request. The dataset used and/or analysed during the current study is part of the first author’s Ph.D. Thesis. The dataset is available from the corresponding author on reasonable request, when he finishes his Ph.D.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.