
Abstract
Aims:
In this study, the 10-year cardiovascular disease (CVD) event risk score of three major migrant origin groups was calculated and compared with the general Finnish population. Furthermore, the study examined the association of insufficient serum D-vitamin concentrations (≤50 nmol/L) with CVD event risk.
Methods:
Cross-sectional data from the Migrant Health and Wellbeing Study (Maamu 2010–2012; n = 881) was used. Participants in the Health 2011 study (n = 798) constituted the reference group. The 10-year CVD event risk scores were calculated with the Framingham risk score (FHS). Logistic regression analysis determined the association between insufficient vitamin D concentrations and increased CVD event risk.
Results:
Migrant origin participants were younger and had a lower proportion of those with moderate or high 10-year CVD event risk (Russian 12.4%, 95% CI 17.5–25.0, Somali 5.7%; 95% CI 3.2–10.1, Kurdish 9.2%; 95% CI 6.7–12.5) than the general Finnish population (21.0%; 95% CI 17.5–25.0), while they had higher prevalence of vitamin D insufficiency (Russian 28.35%, 95% CI 23.48–33.23, Somali 72.85%, 95% CI 66.9–78.71, Kurdish 84.96%, 95% CI 81.15–88.76) than the general Finnish population (6.52%, 95% CI 4.80–8.23). Vitamin D insufficiency was associated with moderate to high 10-year CVD event risk (PR 1.32, 95% CI 1.00–1.32) after multivariable adjustment.
Conclusion:
Vitamin D insufficiency was associated with an elevated estimated 10-year CVD risk in this study. These findings highlight the need for further longitudinal research in larger and more diverse migrant-origin populations.
Background
Cardiovascular diseases (CVD) remain the leading cause of death globally and across Europe, with a striking 60% increase in mortality over the past 30 years from 1991 (12.1 million) to 2021 (20.5 million).1,2 In Finland, circulatory diseases were the leading cause of death in 2020, with an age-adjusted mortality rate of 58.6 per 100,000 in the population.3,4
Significant disparities in CVD mortality have been observed between populations of migrant origin and the majority populations in Europe. For instance, CVD mortality is higher among Asian migrants in Spain and Surinamese male migrants in the Netherlands than in their respective general populations.5,6 Conversely, some migrant groups, particularly those migrating for family reunification, have demonstrated better CVD outcomes compared to the population in the country of migration. 6 Refugees have shown higher mortality from certain CVD events, such as acute myocardial infarction, than the general population in Denmark. 7 However, comparisons across studies are complicated due to heterogeneity across migrant-origin populations, country contexts, and variations in the definition of migrant origin.
CVD is largely preventable. Main behavioral risk factors include tobacco use, unhealthy diet, physical inactivity, and harmful alcohol use. These lead to intermediate metabolic changes such as elevated blood pressure, blood glucose, serum lipids, and overweight/obesity. 1 Several studies have found an association between low circulating vitamin D levels with increased risk of CVD events, including stroke, coronary heart disease, myocardial infarction, and heart failure. 8 A follow-up study by Kilkkinen et al. revealed that vitamin D insufficiency may be associated with fatal CVD events. 9 Proposed mechanisms include vitamin D’s role in inhibiting the renin-angiotensin system, reducing vascular smooth muscle proliferation, and preventing vascular calcification. 10
Vitamin D insufficiency is particularly prevalent among migrant-origin population from the Middle East, Asia, and Africa living in Europe.11–13 In Finland, migrants of Kurdish and Somali origin have also been previously reported to have significantly lower serum vitamin D concentrations compared to the general Finnish population. 14 These groups have also been reported to have higher rates of hyperglycemia. Kurdish migrants exhibit lower HDL cholesterol, higher triglyceride concentrations, and a greater prevalence of smoking among men compared to the general population. Obesity rates, based on BMI, are also higher among Kurdish men and Somali women. The metabolic syndrome, defined as the presence of at least three cardiometabolic risk factors, is more common among Kurdish and Somali women than in the Finnish general population. 15 It has also been reported that lifestyle-related factors did not fully attenuate the observed differences in the prevalence of the metabolic syndrome in the migrant-origin population, particularly among men, pointing to a need to further explore additional risk factors for adverse cardiometabolic outcomes.
The current study examined the association between vitamin D insufficiency and 10-year CVD event risk among Russian, Somali, and Kurdish-origin migrants in Finland. To the best of our knowledge, no prior studies have explored this specific association in migrant-origin populations. Moreover, CVD event risk has not previously been quantified in these groups in the Finnish context. The findings from this study aim to enhance understanding of CVD event risks among migrant-origin populations and may inform both targeted and population-level prevention strategies. Given the presence of large Russian, Somali, and Kurdish communities across Scandinavia and other European countries, these findings hold broader relevance for health policy and practice throughout the region.
Methods
Study design
This study is based on cross-sectional data from the Migrant Health and Wellbeing Study (Maamu) conducted by the Finnish Institute for Health and Welfare (THL) in six major cities in Finland (Helsinki, Espoo, Vantaa, Turku, Tampere, Vaasa) between 2010 and 2012. The stratified random sample of the Maamu study was drawn from the Finnish Population Register and consisted of a total of 3000 persons of Russian, Somali, and Kurdish origin (1000 per study group). The selection criteria were age 18–64 years, country of birth in Russia/former Soviet Union, Somalia, Iran/Iraq, mother tongue (Russian/Finnish or Kurdish), city of residence, and minimum 1-year residence in Finland. 16
The study consisted of a face-to-face interview and a health examination, which were conducted in the native language of the participants by multilingual research personnel. Participants could take part in all or only one part of the study. Biomarker data were gathered among those who took part in the health examination. Those who declined to participate in the full interview were offered a brief interview/questionnaire. 16 Altogether, 70% of Russian, 51% of Somali, and 63% of Kurdish origin persons took part in at least one part of the study.
The current study is restricted to a sub-sample of the Maamu study participants aged 30–64 years, who took part in the health examination and for whom biomarkers were available (Russian origin n = 323; Somali origin n = 192; Kurdish origin n = 326). Restricting the sample of this study to those aged at least 30 years was necessary because the Framingham risk score is typically applied for persons aged at least 30. 17 Restriction to those who took part in the health examination and had biomarker data available was necessary, as biomarkers were needed to calculate the Framingham risk score and estimate the vitamin D levels.
Participants in the Health 2011 survey of corresponding age and cities of residence, as for the Maamu study participants, constituted the general population reference group (n = 787). The Health 2011 survey was also conducted by THL and followed a comparable study protocol to the Maamu study.
A flow chart of the study population is presented in Figure 1.

Flowchart of participants in the study.
Vitamin D levels
The serum 25-OHD concentration was used as a biomarker for vitamin D status, 18 and it was measured using a chemiluminescent immunoassay (Architect ci8200; Abbott Laboratories), which is standardized according to the Vitamin D Standardization Program (VDSP). The sampling period for serum 25-OHD in the Maamu study was from December 2010 to April 2012, while it was from August to December 2011 in the Health 2011 Study. 14
Vitamin D insufficiency was defined as 30–50 nmol/L of serum 25-OHD based on the global evidence-based consensus conducted in 2014, while vitamin D deficiency was defined as less than 30 nmol/L. 11 In the current study, serum 25-OHD concentrations of 50 nmol/L or lower were categorized as vitamin D insufficiency.
Assessment of 10-year cardiovascular disease event risk
The FHS risk score formula was used to calculate the 10-year CVD event risk score based on age, sex, smoking status, diabetes, systolic blood pressure, serum total cholesterol, and HDL cholesterol concentration. 17
The equations for calculating the 10-year CVD event risk score were:




In these equations, So(10) represents the baseline survival rate, ß is the regression coefficient, and X is the level for each risk factor. The 10-year cardiovascular disease (CVD) event risk score was expressed as a percentage. In this study, the use of <10% and ≥10% as a binary threshold to distinguish low from elevated 10-year CVD event risk aligns with well-established clinical practice and validated risk model classifications. According to the Framingham risk model, risk is categorized as low if <10%, moderate if 10% to 19%, and high if ≥20%. 19 Due to sample size restrictions, the risk is presented as binary, <10% low, and ≥10% as moderate or high. Such categorizations was also used in previous study. 19
Other covariates
Age was categorized into age groups (30–44 years old and 45–64 years old). Sex was categorized based on the sex assigned at birth (male or female). Length of stay in Finland was categorized into 1–5 years, 6–10 years, and more than 10 years of stay in Finland. The country of origin is based on the country of birth. The abovementioned data were obtained from the Finnish Population Register.
The presence of hypertension and diabetes diagnosis by a physician (yes/no), use of hypertension medication (yes/no), oral multivitamin supplementation (yes/no), and smoking status (yes/no) were self-reported during face-to-face interviews.
Educational level was categorized into low (lower than high- or vocational school and high (high- or vocational school or higher). Economic activity was categorized as economically active (employed full-time or part-time) and economically inactive (student or other).15,20
The health examination included measuring blood pressure, weight, and height. Blood pressure was measured from the right arm with a digital blood pressure monitor (Omron i-C10, Oriola) three times at 1-min intervals in the Maamu study and twice using a manual standard mercury sphygmomanometer in the Health 2011 survey. Body mass index (BMI) was calculated and categorized as normal (<24.9 kg/m²) and overweight or obese (>25 kg/m²). 15
In both studies, trained laboratory technicians took the blood samples, which were centrifuged within an hour and stored at −70°C until analysis. 14 Serum total cholesterol and High-Density Lipoprotein (HDL) cholesterol concentrations were analyzed using enzymatic assays with Abbott Architect c8000 analyzer (Abbott Laboratories, Abbott Park, IL).
Confounding
Confounding variables were selected based on biological plausibility and prior studies, considering also the study design and sample size. Age and sex are established CHD risk factors. 17 There is also evidence on differing cardiovascular health outcomes by country of origin. 21 Winter sampling was selected to account for natural seasonal variations in vitamin D levels. 14 The use of multivitamin supplements was also adjusted as potential determinant of vitamin D status and its potential to lower the risk for CVD events. 22
Statistical analysis
The prevalence of categorical variables was determined using frequency and percentage, while continuous data were presented as mean, standard errors of mean, and confidence intervals. The Kruskal-Wallis test was used to determine the differences in ranking of the 10-year CVD event risk score among the three migrant groups and the general population. We opted for a non-parametric test due to the 10-year CVD risk score distribution being markedly right-skewed. Logistic regression analysis was used to model the event of an elevated or moderate to high 10-year CVD risk score in the migrant-origin participants as a function of vitamin D insufficiency (Model 1, unadjusted), and was also adjusted for country of origin, age, sex, multivitamin supplement, and season of blood sampling. Odds Ratios and Prevalence Ratios were calculated.
A p-value of p < 0.05 was considered statistically significant. Inverse probability weights (IPW) were used in all models, based on the register information from the National Population Register on age, sex, marital status, country of origin and municipality were used to correct for the effects of non-response bias and different sampling probabilities to provide representative results with the survey and register data. 23 The population size being relatively small, a significant proportion of the total population was included in the sample of Maamu, and thus, the finite population correction was applied in all analyses. The data were analyzed using R statistical software version 4.3.3 22 and packages survey 24 and marginal effects. 25
Results
In all study groups, the proportion of men was lower than that of women, except among the Kurdish-origin group (Table 1). Migrant-origin groups were generally younger and demonstrated lower levels of economic activity compared with the general population. Educational attainment was lower among Somali- and Kurdish-origin participants, whereas it was higher among those of Russian origin. Most individuals from migrant backgrounds in the study had resided in Finland for more than 10 years.
Descriptive characteristics of the study participants.
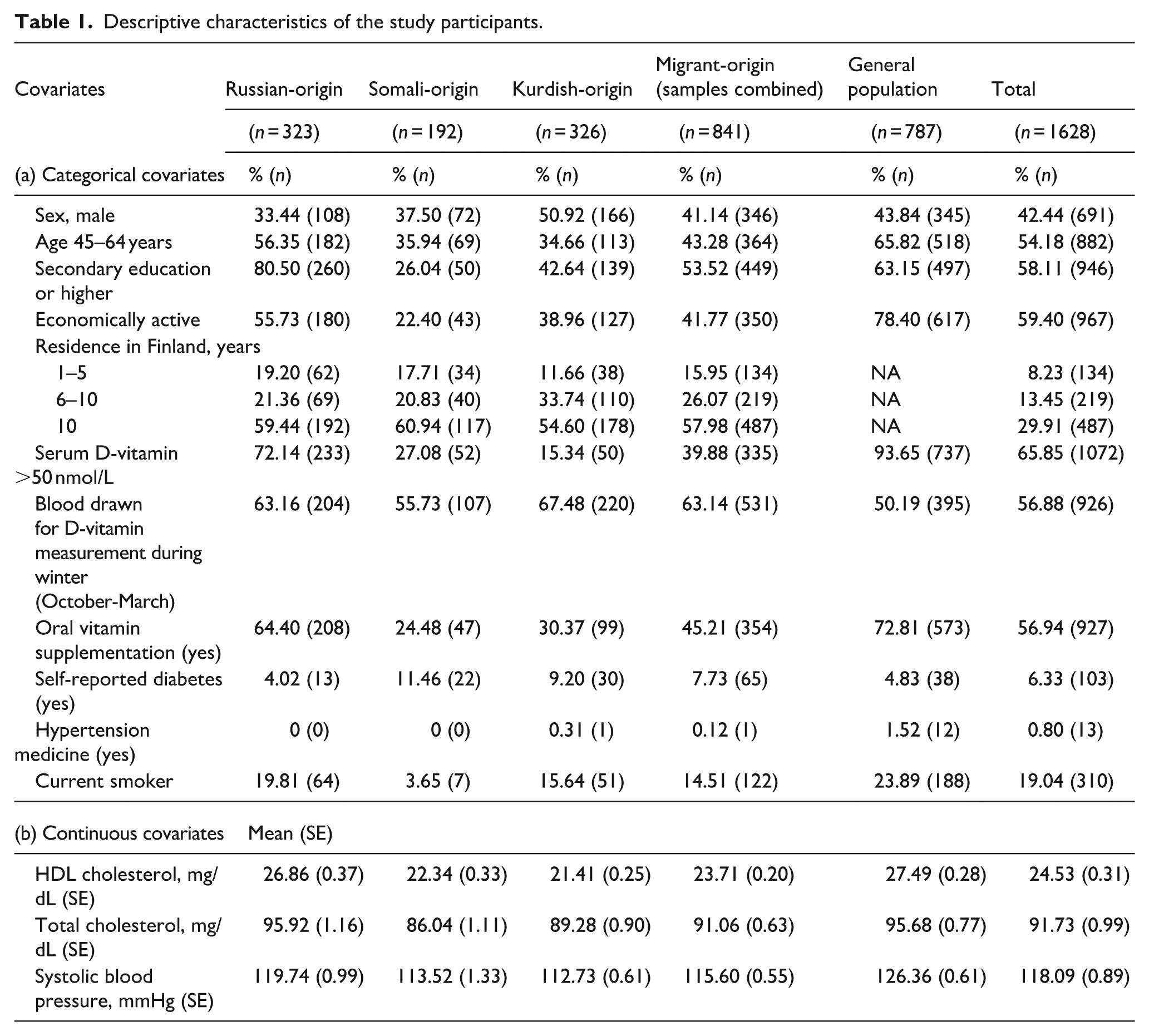
Vitamin D sufficiency, defined as serum 25-hydroxyvitamin D (25[OH]D) concentrations ≥50 nmol/L, and the use of oral multivitamin supplements were less prevalent among migrant groups—particularly those of Kurdish and Somali origin—compared with the general population. Blood samples for measuring 25(OH)D concentrations were primarily collected during the winter months (Table 1).
A higher proportion of participants from migrant-origin groups reported having diabetes, with particularly elevated rates among Somali and Kurdish-origin participants (Table 1). The reported use of hypertension medication was low across all study groups. Smoking was more prevalent in the general population than among migrant groups. Among migrants, the highest prevalence of smoking was reported in the Russian-origin group, followed by the Kurdish-origin group, with the lowest prevalence observed among Somali-origin participants.
Total cholesterol, high-density lipoprotein (HDL) cholesterol, and systolic blood pressure (SBP) were higher in the general population compared with the migrant groups. Among the migrant groups, participants of Russian origin had the highest levels of total cholesterol, HDL cholesterol, and SBP.
The prevalence of ≥10% 10-year CVD event risk was highest in the general population (21.0%; 95% CI 17.5–25.0), followed by participants of Russian (12.4%; 95% CI 9.0–16.9), Kurdish (9.2%; 95% CI 6.7–12.5), and Somali (5.7%; 95% CI 3.2–10.1) origin. Overall, the prevalence of elevated CVD risk was significantly lower among all migrant groups compared with the general population (Figure 2). This finding was in line with the Kruskal-Wallis test indicating statistically significant rank differences among the groups for the 10-year CVD risk score (χ2(3) = 91, p < 0.001) and distributions showing mean values with the same ordering: the mean risk score was highest in the general population (mean = 6.5; 95% CI 5.8–7.1), followed by participants of Russian (mean = 5.1; 95% CI 4.4–5.9), Kurdish (mean = 4.1; 95% CI 3.7–4.6), and Somali (mean = 3.3; 95% CI 2.8–3.8).

Prevalence of moderate to high 10-year cardiovascular event risk score (95% CI).
The unadjusted model estimates indicated that participants in the study with vitamin D insufficiency had a lower likelihood of having an elevated 10-year CVD event risk score (Table 2). However, after multivariate adjustment for country of origin, age, sex, multivitamin supplement intake, and season of blood sampling, the marginal prevalence ratio revealed that the probability of an elevated CVD event risk was 32% higher for individuals with vitamin D insufficiency. The Nagelkerke pseudo-R2 indicated that 31% of the variance in the 10-year CVD event risk scores was explained by the variables in this adjusted model.
Model estimates for the association of insufficient vitamin D concentration with moderate or high 10-year cardiovascular disease event risk.
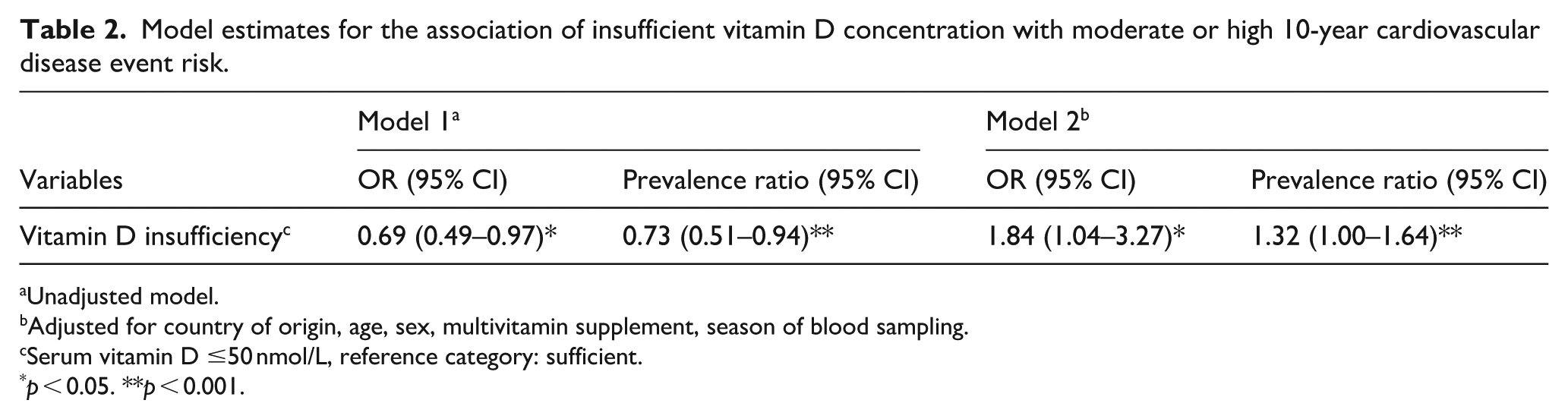
Unadjusted model.
Adjusted for country of origin, age, sex, multivitamin supplement, season of blood sampling.
Serum vitamin D ≤50 nmol/L, reference category: sufficient.
p < 0.05. **p < 0.001.
Discussion
This study is the first in Finland to examine the association between vitamin D insufficiency and estimated 10-year cardiovascular disease (CVD) event risk among Russian, Somali, and Kurdish-origin populations. Migrant origin groups in this study had lower 10-year CVD event risk scores and a higher prevalence of insufficient vitamin D concentrations compared with the general population. After adjustment for key covariates, including age, sex, country of origin, multivitamin supplement intake, and season of blood sampling, vitamin D insufficiency was associated with an elevated 10-year CVD event risk score. These findings contribute to the limited body of evidence assessing CVD risk among diverse migrant populations in high-income countries.
Participants from the general population in the Health 2011 Survey have significantly higher 10-year CVD event risk scores than the migrant-origin participants in the Maamu Study. This may be partially explained by differences in age structure, as the general population sample was older. Age is a major determinant in the FHS risk score and exerts considerable influence on 10-year risk estimations. 17 Consequently, lower risk among migrants may not fully reflect their future CVD burden. Similarly, findings from the Finnish Diabetes Prevention Program (FIN-D2D) reported elevated mean 10-year CVD event risk among Finnish participants, particularly among men, with a mean score of 19.9, which decreased after lifestyle counseling. 5
Among the migrant groups, participants of Russian origin have the highest prevalence of elevated 10-year CVD event risk consistent with their elevated biomarker profile, such as smoking prevalence, total cholesterol, and systolic blood pressure. These risk profiles were also comparable to those observed in the general Finnish population. These findings align with previous research from the Know Your Heart (KYH) study, which reported similarly elevated mean systolic blood pressure and smoking prevalence among Russian men. Furthermore, total and HDL cholesterol levels in the KYH cohort were similar to those reported in the Tromsø 7 study from Norwegian population. 28
The Somali-origin group has the lowest 10-year CVD event risk score. This result may appear counterintuitive given their higher prevalence of diabetes 21 and vitamin D insufficiency. However, Somali-origin group has lower mean total cholesterol levels and SBP, as well as lower prevalence of smoking compared to the general population, which likely contributed to lower calculated 10-year CVD event risk scores. Notably, previous studies have shown a higher prevalence of hypertension among Somali men and elevated cholesterol in both sexes in the Oslo cohort; however, their 10-year CVD event risk scores did not significantly differ from those residing in Somaliland. 19 These findings suggest that alternative or more tailored risk models may better capture long-term CVD risk among Somali migrants.
Kurdish-origin migrants living in Finland demonstrated a lower prevalence of smoking, as well as lower mean total cholesterol, HDL cholesterol, and systolic blood pressure compared to the general population. However, findings from the same cohort revealed that Kurdish men in Finland had a lower prevalence of hypertension but a notably higher prevalence of dyslipidemia and hyperglycemia than those in the general population. 15 This again highlights the limitations of conventional risk models like the FHS score, which may not fully incorporate relevant risk factors such as waist circumference or triglyceride levels.
Considering the higher prevalence of various cardiovascular risk factors and metabolic syndrome reported in previous studies among the migrant origin groups examined, 21 the observed lower prevalence of elevated 10-year CVD event risk in this study may appear somewhat unexpected. Despite a higher incidence of metabolic syndrome, particularly among Kurdish- and Somali-origin women in Finland, their 10-year CVD event risk scores were significantly lower than those of the general population. This discrepancy likely reflects differences in the risk components included in the metabolic syndrome criteria versus the 10-year FHS risk score. Although migrant populations in this study exhibited higher rates of abdominal obesity, elevated blood pressure, triglycerides, and fasting glucose, not all these factors are incorporated into the FHS risk calculation. 21 Future research should investigate which risk metrics more accurately predict long-term CVD outcomes in migrant populations.
The Framingham Heart Study (FHS) risk score was selected to calculate the 10-year CVD event risk scores due to its validation across multiple ethnic groups.17,19 Alternative models include SCORE, which estimates fatal CVD risk in European populations; 21 WHO/ISH charts, 29 which are tailored to regional epidemiological profiles using basic clinical indicators; and QRisk, a UK-based model that incorporates a broader range of variables such as ethnicity, chronic conditions such as type 2 diabetes, rheumatoid arthritis, atrial fibrillation, and chronic kidney disease, and social deprivation. 30 The FHS score was considered most appropriate for this study because it has been validated in multiethnic cohorts, 17 and not all required variables for QRisk were available, and WHO/ISH and SCORE were less aligned with the study population and available data.
Vitamin D insufficiency was associated with an elevated 10-year CVD event risk score in the adjusted model. This finding support previous prospective study, which reported that individuals with higher serum 25(OH)D concentrations (≥25.00 nmol/L) were significantly associated with lower risks CVD events as compared to those with levels <25.00 nmol/L, while the greatest risk reductions of CVD death were observed to those with ≥50.00 nmol/L. 31
Moderate to severe vitamin D insufficiency has been identified as a significant risk factor for developing CVDs, such as hypertension, with studies indicating a three- to six-fold increased risk among individuals with insufficient vitamin D levels. 32 Additionally, a prospective study found that each 10 nmol/L increase in baseline [25(OH)D] concentration was associated with lower serum triglyceride and very low-density lipoprotein (VLDL) cholesterol levels, as well as a reduced incidence of metabolic syndrome after 5 years of follow-up. 22
Strengths and limitations
This study has several notable strengths. It utilized a population-based study design, a representative sample of three distinct migrant-origin groups—Russian, Somali, and Kurdish—in Finland, alongside a general population reference group. The study employed standardized protocols for data collection, including health examinations and laboratory analyses, ensuring comparability across groups. The use of multilingual personnel and culturally sensitive methodologies enhanced participation and data accuracy. Importantly, this is the first study to quantify 10-year CVD event risk and examine its association with vitamin D status among these migrant populations in the Finnish context.
Despite these strengths, several limitations warrant consideration. First, the cross-sectional nature of the data limits causal interpretation. Although an association between vitamin D insufficiency and elevated CVD event risk was observed, temporal relationships cannot be established. Second, data on other lifestyle factors—such as diet, alcohol consumption, and physical activity—were not included in the current analysis. Additionally, the study lacked detailed information on vitamin D supplementation, including dose, duration, and adherence, which may influence serum 25(OH)D concentrations.
The presence or absence of diabetes was based on self-report, and fasting blood glucose was not taken into consideration, as it would necessitate limiting data to only those who had fasted. This may potentially underestimate metabolic risk. Additionally, there were minor differences in how blood pressure was measured in the Maamu and the Health 2011 studies. 20 However, it is unlikely that these differences had a significant influence on the findings of this study.
Finally, the FHS risk score, while widely validated, was primarily developed in predominantly Caucasian populations. Its applicability to multiethnic groups—particularly in the context of migration—remains limited. There is currently no CVD risk model calibrated for multiethnic populations in Finland, underscoring the need for future validation studies using longitudinal data.
In summary, while this study provides valuable insights into the cardiovascular health of migrant populations in Finland, future research should address these limitations through longitudinal study designs, inclusion of additional lifestyle and genetic variables, and more inclusive risk models calibrated for diverse populations, incorporating nontraditional risk factors, such as vitamin D status, which may enhance CVD risk stratification in migrant health assessments.
Conclusion
Vitamin D insufficiency was associated with an elevated estimated 10-year CVD risk in this study. These findings highlight the need for further longitudinal research in larger and more diverse migrant-origin populations to confirm this association and explore its implications for prevention strategies.
Footnotes
Acknowledgements
The authors express gratitude to the researchers, participants, and field workers in the Maamu project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NS received funding from the Signe and Ane Gyllenberg Foundation (Grant number 5725) and the EU4Health Joint Action on Cardiovascular Diseases and Diabetes (JACARDI) project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.