
Abstract
Objective:
Smoking during pregnancy is an important predictor for birth outcomes that have an impact on their postpartum health, cognitive abilities, and economic standing. While extensive research has been conducted on the association between smoking and preterm birth, there is a scarcity of comprehensive evidence specific to the Africa region. This review aimed at generating summarized evidence on the association between maternal exposure to cigarettes smoking and preterm birth in Africa.
Method:
PubMed, Google Scholar, and the African Journals Online databases were used to conduct a thorough literature search. Review inclusion was open to all designs of observational studies. The Newcastle-Ottawa Scale (NOS), which was used for case-control, cohort and cross-sectional studies, was the measure used for quality assessment. To get the pooled estimates and the associated 95% confidence interval (CI), the random-effects model was utilized.
Result:
A total of four studies were included in the prevalence and association meta-analysis. Among women with active smoking exposure, the pooled prevalence of preterm birth was 19.44% (95% CI [16.04, 22.84]), with moderate heterogeneity (I2 = 63.49%, p = .05). Among passive the prevalence was 17.5% ([10.88, 24.12]) with no observed heterogeneity (I2 = 0%). The overall pooled prevalence was 19.22% ([16.28, 22.16]). For association estimates, the overall pooled AOR across studies was 3.18 ([1.30, 5.06]),
Conclusion:
This review showed that maternal tobacco exposure, whether active or passive, is associated with an increased risk of preterm birth in African countries.
Introduction
Preterm birth (PTB) is an adverse pregnancy outcome that is the leading cause of neonatal morbidity and mortality worldwide. PTB babies are born alive before 37 weeks of pregnancy completed (WHO, 2020). Based on gestational age PTB can be classified as Extremely preterm (<28 weeks), very preterm (28–31 weeks), and late preterm (32–37 weeks). 1 Preterm birth can be also classified by its clinical presentations as spontaneous and iatrogenic preterm (World Health Organization, 2017). Each year, approximately 15 million preterm births occur worldwide, accounting for more than 1 in 10 premature births, with the worldwide PTB rate ranging from 4% to 16%, although this is higher in low and middle-income countries. 2
According to a study report conducted by 3 preterm birth is the top cause of neonatal mortality and the second most common cause of mortality after pneumonia among children under five (WHO,2023). Another study 4 reported that developed countries like, United States, also amongst the top 10 countries with the greatest numbers of preterm births. Moreover, the incidence of preterm births report by 5 is; 9.6% globally, 7.5% in developed countries, 12.5% in developing countries, 9.1% in Asia, 6.2% in Europe, 10.6% in North America, and 11.9% in Africa. He 5 is also reports more than 60% of preterm births occur in Africa and South Asia, in developing countries. Another study conducted by 6 reported that PTB increased to 10.6% in 2014 globally.
There are also studies conducted in different countries that report the rate of premature birth. A study conducted by 7 reported the premature birth rate rose from 9.8% to 17.1% in South East Nigeria, 5% in Northern European countries, 18.1% in Malawi. 8 18.3% of preterm births prevalence reported in Kenya, 9 1.6% in Debremarkos town, Ethiopia, 10 31.4% in Mettu Karl Hospital, Ethiopia, 11 34% in the Tigray region of Ethiopia, 12 35% in Dessie Referral Hospital, 13 25.9% in Jimma, Ethiopia, 14 and 16.1% in Debre Berhan, Ethiopia. 15 A study conducted by 16 Reported Preterm birth causes 75% perinatal mortality and greater than 50% of long term morbidity. A systematic review and meta-analysis study on preterm birth with three single studies also conducted in Ethiopia. 17 The risk of dying from preterm birth complications is 10 times greater for babies born prematurely in low-income countries than for those born in high-income countries. 18
In sub-Saharan Africa, More than 60% of babies are born preterm, which has a severe negative impact on health and productivity. Preterm babies are more susceptible to other illnesses and are the second leading cause of infant mortality. Preterm births continue to be a major challenge in developing countries. 19
Maternal exposure for cigarette smoking during pregnancy has been identified as a key factor contributing to preterm birth.20–23 Recently, a systematic review conducted by 24 Reported the global prevalence of during-pregnancy smoking to be 1.7%. The research results demonstrated the prevalence and incongruous data regarding the adverse impact of maternal cigarette smoking during pregnancy on the course of childbirth.20–23 While extensive research has been conducted on the association between smoking and preterm birth, there is a scarcity of comprehensive evidence specific to the Africa region.
Thus, a thorough comprehension and summary of the effects of maternal smoking during pregnancy on preterm birth are urgently needed in Africa countries. This study aims to provide comprehensive evidence on the pooled prevalence of maternal smoking and preterm birth, as well as the pooled effects of cigarette smoking and preterm birth. The study also provides comprehensive evidence for researchers, practitioners and maternal health intervention policy makers to focus on fetus well-being during maternal pregnancy.
Objectives
The main objectives of this study are:
Quantitatively examine the pooled prevalence preterm birth in Africa
Quantitatively examine the pooled effects of smoking on preterm birth.
Significance for public health
To determine the current prevalence of preterm birth and associated factors among pregnant women who smoke cigarette during their pregnancy in Africa. Additionally, the findings of this study will be useful in helping to make quick decisions.
Materials and methods
This systematic review and meta-analysis was registered on PROSPERO with a protocol number CRD42024504761.
Search strategies
The reporting of this systematic review and meta-analysis adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA 2020) statement guidelines for systematic reviews and meta-analyses. 25 The completed PRISMA checklist is available as Supplemental Material 1.
A comprehensive search has been conducted in electronic databases (PubMed, Google Scholar, African Journals Online and MedRxiv) using a combination of keywords related to cigarette smoking, preterm birth, and Africa. Grey literature and pertinent reference lists have also been manually searched. All possible keyword combinations have been combined in order to conduct systematic searches. A review has been conducted to identify potentially eligible studies from the reference lists of key full-text articles included in the review. No formal sample size calculation was conducted for this meta-analysis. The systematic procedure substantiates that the literature search comprises all studies published from 2018 to 2024 on the impact of smoking during pregnancy on preterm birth in Africa. This date restriction was applied intentionally to include the most recent and methodologically robust studies. Contemporary studies are more likely to reflect current public health policies, updated definitions of preterm birth, and enhanced exposure assessments, including both active and passive smoking. In addition, studies published in this timeframe are more likely to conform to standardized reporting frameworks, and to adjust for critical confounders such as antenatal care utilization, maternal nutrition, and alcohol or substance use. Older studies prior to 2018 were excluded to reduce methodological heterogeneity, particularly due to inconsistent exposure classification, missing adjusted effect sizes, or outdated diagnostic criteria. This exclusion is acknowledged as a limitation in the Discussion section. It is believed that the search strategy is sufficient to lower the chance of bias in detection and selection. After exporting the search results to Mendeley, duplicates were eliminated. The titles and abstracts of the studies were independently screened by two authors (KGA and AAH), and any disagreements between the authors were settled by consensus or by discussion. The search strategy words and MeSH terms. is presented in Table 1. We also used Boolean operators “AND” and “OR.” Moreover the search strategy of PubMed database is presented in Table 1.
PubMed search strategy.

Searching words
In this study the searching terms are used to research the relationship between cigarette smoking and preterm birth. The risk factor examined is cigarette smoking, with the outcome variable being preterm birth. The exposure terms include MeSH terms like tobacco, substance use, tobacco use, tobacco smoking, cigar smoking, and cigarette smoking. Free text terms such as active smoker and passive smoker are also included. The outcome terms consist of MeSH terms like preterm birth, premature birth, abortion, prematurity, pregnancies, and gestation.
Eligibility criteria
Inclusion criteria
All observational studies (cross-sectional, case-control, and cohort) reported the association between cigarette smoking and preterm birth and conducted in African countries were eligible for this systematic review and meta-analysis. Studies published from September 2018 to May 30, 2024, only in the English language were included mainly to avoid mistakes in the translation process.
The following types of studies were excluded:
✓ Articles that did not provide or reported ORs and 95% CIs.
✓ Review studies.
✓ None related to the maternal smoking and specified pregnancy outcomes, and
✓ Studies published before September 2018.
✓ Descriptive reviews randomized controlled trials, systematic review, meta-analysis, Editorials, comments, conference summaries and expert opinions, not precisely measured the prevalence and the association between maternal smoking during pregnancy and adverse specified birth outcome has been excluded.
Outcome measures
There are two main outcomes in this systematic review and meta-analysis. The first outcome was the prevalence of preterm birth. The second outcome of the study is level of association between smoking and preterm birth.
Selection of studies
Two impartial reviewers (KGA and AAH) to determine eligibility based on predetermined standards have screened titles, abstracts, and full-text articles. Any discrepancies were resolved through discussion. Furthermore, a justification for the inclusion and omission of studies in the PRISMA flow diagram has been provided. Finally, a final list of publications is ready for data extraction for systematic reviews and meta-analyses.
Methodological quality assessment
The included studies’ methodological quality was evaluated independently by two authors (KGA and AAH) using the 9-star NOS technique. NOS scale rates observational studies based on 3 parameters: selection, compared between the exposed and unexposed groups, and exposure/outcome assessment. The scale assigns a maximum of 4 stars for selection, 2 stars for comparability, and 3 stars for exposure/outcome assessment. Studies receiving five stars or fewer were regarded as low quality, those receiving five to seven stars as moderate quality, and those receiving more than seven stars as high quality (35).
Data extraction
The data has been extracted using a standardized form. A data extraction form has been developed and piloted to obtain the necessary data for the systematic review and meta-analysis. For the eligible studies, the extraction information included the following: study characteristics, participant characteristics, exposure and outcome measurements, and statistical data required for meta-analysis. Author’s name, year of publication, setting where the study was conducted (country), study design, sample size, study population, socio demographic variables, birth outcome definition, number of cases, prevalence of outcomes, and 95% CI, lists of statistically significant associated factors of adverse birth outcomes, with their effect size and 95% CI. When data is missing from the articles, attempts have been made to retrieve the data by contacting the study’s corresponding author. Finally, the extracted data in Microsoft Excel has been prepared for the analysis and the result is presented using table.
Statistical synthesis
Stata version 17.0 software has been used to conduct the meta-analysis. We calculated the pooled prevalence for preterm birth, along with the 95% confidence interval (CI) and corresponding P-value. We also calculated the pooled adjusted odds ratio (AOR) for the association between smoking and adverse pregnancy outcome which is preterm birth in Africa. Heterogeneity among eligible studies has been assessed using the I2 test. If I2 > 0.5, it is considered that there is significant heterogeneity among the eligible studies, a random-effects meta-analysis model (REML) with the inverse variance method and separate subgroup analysis for active and passive smoking exposure would be used in this case. The sub-group analysis also conducted to assess the robustness of synthesized result. Evaluation of publication bias across studies will be examined through using visual inspection of funnel plots and Egger’s test. Newcastle Ottawa scale (NOS) quality assessment methods could be applied for risk of bias assessment.
Results
From databases, initially, 39,214 studies screened in our search. Due to duplication 30,404 studies were removed. 8810 studies were screened and 8,737 studies excluded by their title and abstract. 73 Full-text articles assessed for Eligibility and 69 studies were removed with reasons (did not met inclusion criteria). Lastly, we recognized 4 studies20–23 appropriate to this systematic review and meta-analysis. In this review, 1,822 samples were included. Moreover the selection and refining process of these articles is presented in Figure 1.

Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow chart.
Study characteristics
In this systematic review and meta-analysis, we included 4 studies of which 2 are cross-sectional and the remaining 2 are cohort and case-control studies focusing on the association between preterm birth and cigarette smoking among pregnant women in Africa. The summarized data of the key characteristics of the included studies were showed in Table 2.
Characteristics of studies assessing smoking during pregnancy as a risk factor for preterm birth (PTB).

Table 3 presents the methodological characteristics of the included studies that investigated the association between maternal smoking and preterm birth in Africa. It points the study settings were exclusively hospital based, and the definition of smoking exposure varied.
Methodological characteristics of the studies on maternal smoking and preterm birth in Africa.

Risk of bias assessment
The risk of bias of included studies was assessed by using the modified Newcastle Ottawa scale (NOS) quality assessment methods. We considered high and moderate quality studies for this review. Accordingly 4 studies20–23 were appraised as moderate and high quality and included for final systematic review and meta-analysis.
Publication bias
The Funnel plot was utilized to identify any possible publication bias for these set of studies. Thus, it appears that all eligible studies have not publication bias, according to the symmetry funnel plot (Figure 2). In addition, The Egger’s test did not detect any statistically significant small-study effects in the meta-analysis (β1 = 0.92, p = 0.38). Therefore, publication bias is unlikely, and the pooled estimate of the AOR is considered reliable with respect to study size effects. Thus, it is possible to say that non-significant studies may not have been published, which could result in an overestimation of the pooled effect size.
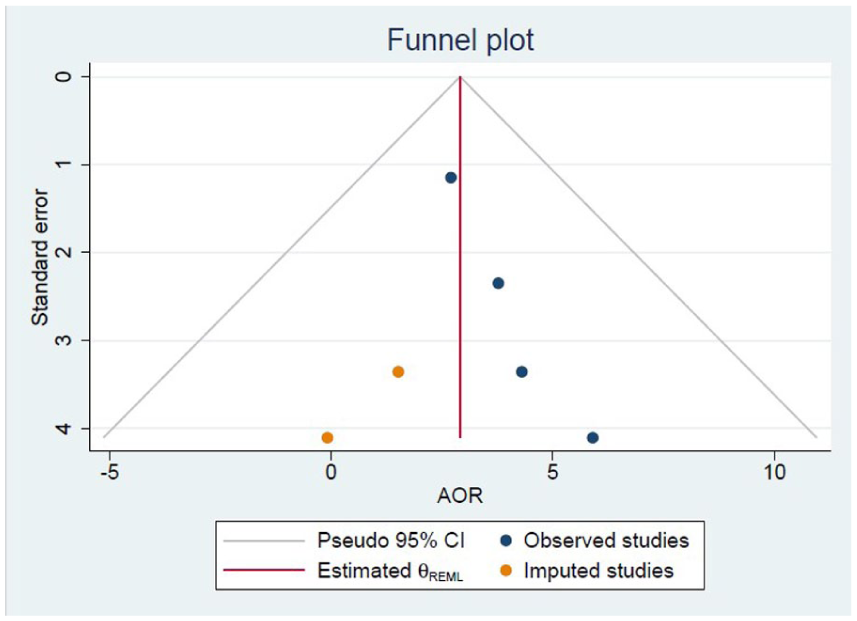
The Funnel plot utilized to identify any possible publication bias for these set of studies.
Meta-analysis results
Pooled prevalence of preterm birth
A total of four studies reported the prevalence of preterm birth occurrence among cigarette smoker mothers during pregnancy, and the pooled prevalence estimate computed was 19.22% (95% CI [16.28, 22.16], I2 = 52.96%), and telling us there is moderate heterogeneity among study findings on prevalence of preterm birth among women who were exposed to both active and passive cigarette smoking during their pregnancy period (Figure 3).

Forest plot for the prevalence of preterm birth among mothers who smoke cigarette during pregnancy.
Pooled adjusted odds ratio
The pooled adjusted odds ratio (AOR) for maternal smoking exposure was 3.18 (95% CI [1.30, 5.06]), indicating that tobacco exposure nearly triples the risk of preterm delivery (Figure 4).

Forest plot illustrating the association between cigarette smoking and preterm birth.
Discussion
This study was conducted to examine the association between cigarette smoking during pregnancy and pregnancy outcome, which is preterm birth in African countries. To the best of our knowledge, this systematic review and meta-analysis is the first of its kind that assessed the association between cigarette smoking during pregnancy and preterm birth in African countries. This study includes 4 articles focusing on the association between cigarette smoking during pregnancy and preterm birth and prevalence of preterm birth in African countries. We believed that all of the included studies are conducted with the ethical guideline. The pooled effect size of the association between cigarette smoking during pregnancy and preterm birth and preterm birth prevalence are discussed.
In our review, the pooled OR and preterm prevalence were computed from four studies23,26–29 that reported both the association and preterm prevalence. The estimated pooled OR showed cigarette smoking during pregnancy was more than three times more likely to give PTB compared to their unexposed counterparts. Another systematic review and meta-analysis study reports comparable evidence. 30 It is conceivable that hazardous chemicals in cigarettes, such as nicotine, affect human germ cells and are known to negatively impact embryonic development, particularly during organogenesis. 17
The outcome of this research is consistence with a growing body of both epidemiological and toxicological research that links maternal cigarette smoking with increased risks of preterm birth.31–34 Systematic reviews and meta-analyses conducted in sub-Saharan Africa confirm our findings, 35 worldwide 36 and Ethiopia. 17 Similarly, national level studies in Bangladesh and Zambia reported that the use of tobacco smoking during pregnancy increases the risk of preterm birth.34,37
There appears to be convincing now that mother exposure to passive and active cigarette smoke during pregnancy increases the risk of preterm birth, one of the poor pregnancy outcomes.23,26–29
The possible reason is that the inhalation of cigarette smoke during active or passive smoking could be the cause. The particles are concentrated and raise the risk of adverse health effects on the developing fetus and reproductive system.38,39 Furthermore, smoking has been linked to preterm birth as mentioned by Gómez-Roig et al. According to an additional large case-control research conducted in Jordan, babies born to moms who smoke had considerably lower birth weights than babies born to passive or nonsmoking mothers. 40
In addition to biomedical and socioeconomic determinants, psychosocial factors may influence smoking behaviors during pregnancy in African settings. Barriers such as limited access to cessation services, low awareness of associated risks, and cultural perceptions of smoking can hinder prevention efforts. Importantly, emerging evidence indicates that stigma surrounding smoking during pregnancy may further discourage affected women from seeking healthcare advice or cessation support. Recent studies by 41 and 42 have shown that perceived and internalized stigma is linked to lower smoking reduction during pregnancy, increased resistance to health warnings, and reduced willingness to discuss smoking with health professionals. Addressing such psychosocial barriers, alongside structural and health system challenges, is essential for developing effective and culturally sensitive public health strategies to reduce maternal smoking and its adverse outcomes, including preterm birth.
The implication of this study is that preterm birth is significant public health problems in Africa. Because of exposure of women to cigarette smoking before and during pregnancy leads women to inhale them for hours which consequently lead to adverse pregnancy outcomes. Despite the progress made to reduce the burden of maternal and infant mortality and morbidity in the continent, the magnitude of this adverse pregnancy outcome is still one of the challenges that need to be addressed. Identifying the association between cigarette smoking with preterm birth can help the efforts to revise, amend or implement treatment guidelines for the clinician and contribute valuable imputes for policy and decision-makers.
While our meta-analysis provides critical insights into the association between maternal smoking and preterm birth in Africa, several methodological limitations warrant acknowledgment. First, the inclusion of only four studies, despite their combined sample size (N = 1822), reflects the scarcity of region-specific research on this topic, which may limit the generalizability of our findings. Second, the restriction of the literature search to studies published between 2018 and 2024. While this decision was made to ensure the inclusion of methodologically consistent and recently conducted studies particularly those using updated definitions of preterm birth and more accurate classifications of tobacco exposure, it may have inadvertently excluded relevant earlier studies. This could have contributed to the relatively small number of eligible articles and may limit the generalizability of findings across a longer historical timeframe. However, we prioritized consistency in exposure measurement and availability of adjusted effect estimates to enhance the validity of the pooled analysis. Third, the evidence base is geographically limited, with included studies drawn only from Ethiopia, Rwanda and South Africa, which restricts generalizability to other African regions. Potential contextual factors, such as the high HIV prevalence in South Africa, may confound the observed associations and were not consistently adjusted for across studies. Second, although both active maternal smoking and passive second-hand exposure were analyzed in subgroups, some primary studies did not clearly distinguish between the two, potentially leading to exposure misclassification. Fourth, the inclusion of different study designs (case–control, cohort, cross-sectional) introduces methodological heterogeneity. While the random-effects model and inverse-variance weighting help account for this, case–control studies cannot provide unbiased prevalence estimates by design, and their inclusion in prevalence pooling should be interpreted with caution. Fifth, covariate adjustment varied across studies, with some controlling for key confounders (e.g., maternal age, socio-economic status) and others adjusting for fewer variables, which may influence effect estimates. Sixth, the number of eligible studies was small, limiting the power of publication bias tests and reducing the robustness of subgroup comparisons. Seventh, substantial statistical heterogeneity was observed in some pooled estimates, likely due to differences in study populations, exposure definitions, outcome definitions, and adjustment sets. Eightnth, No formal sample size calculation was conducted for this meta-analysis, as all eligible studies meeting the inclusion criteria during the search period were included. The final sample size was dependent on the available published evidence, which may limit the statistical power of subgroup analyses. Finally, given these limitations, the findings should be interpreted carefully, with a strong recommendation for further high-quality, multi-country studies in Africa that distinguish between active and passive smoking, comprehensively adjust for major confounders, and utilize standardized definitions and measurements.
Conclusion
The results of this review strongly suggest that smoking cigarettes significantly increases the risk of preterm birth in Africa. The study also found a wide range in the prevalence of preterm birth among pregnant women who were active smoker, and the findings reinforce the urgency of integrating tobacco control into maternal and reproductive health programs in Africa. Routine screening for both active and secondhand smoke exposure should be embedded within antenatal care systems, along with targeted health education, cessation support, and policy level enforcement to reduce household and environmental exposure to tobacco smoke. It is crucial for expectant mothers to be aware of the potential negative effects of smoking on their baby’s health, and to take appropriate steps to safeguard their pregnancy.
In summary, maternal tobacco exposure is a critical, yet under-addressed, contributor to preterm birth in Africa countries. Addressing this modifiable risk factor holds promise for reducing neonatal morbidity, improving maternal health outcomes, and achieving broader Sustainable Development Goals related to maternal and child health across the continent of Africa.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251388567 – Supplemental material for Association between preterm birth and cigarette smoking among pregnant women in Africa: Systematic review and Meta-analysis
Supplemental material, sj-docx-1-phj-10.1177_22799036251388567 for Association between preterm birth and cigarette smoking among pregnant women in Africa: Systematic review and Meta-analysis by Kassaye Getaneh Arge and Aragaw Asfaw Hasen in Journal of Public Health Research
Footnotes
Acknowledgements
The authors acknowledged the researchers of primary studies for this comprehensive review.
Abbreviations
CI: Confidence Interval; MeSH: Medical Subject Headings; NOS: Newcastle Ottawa Quality Assessment Scale; OR: odds ratio; PRISMA: Preferred Reporting Items for Systematic Review and Meta-Analysis.
Ethical considerations
Ethical approval and informed consent are not required as this was a systematic review and meta-analysis.
Author contributions
KGA developed the research question, wrote the first draft, designed the search strategy, and edited and approved the final version of the manuscript and managed the overall works. AAH revised the search strategy of databases, developed the data extraction form, performed data collection, edited and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are contained in the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.