
Abstract
Monkeypox disease (mpox) is an endemic zoonosis, previously restricted to Central and Western African countries. Since 2022, it is the most common orthopoxvirus (OPXV) zoonotic disease observed in non-endemic countries, including Europe and America, and 333 cases of mpox were already confirmed in the Balkan countries. To monitor and control the spread of mpox, a surveillance program was established in line with WHO guidelines. Although the risk of disease has diminished, sporadic cases still occur. The reemergence of mpox cases at the end of 2024 in Greece, where the first case was registered at the end of May 2022, and the first case recorded in Kosovo raised concerns about a potential outbreak of mpox in the Balkans. Here, we describe the clinical data of significant cases to provide a better understanding in terms of epidemiology, clinical symptoms and diagnostic methods for the detection of this disease. Our results reveal that mpox was diagnosed mainly among young and middle-aged men and people with high-risk behaviors, mostly as coinfections with the human immunodeficiency virus (HIV). This suggests that measures for effective tracing as well as vaccination of high-risk groups of the population are essential pillars to control mpox outbreaks.
Keywords
Significance for public health
Over the past two decades, the human monkeypox disease (MPOX) caused by the monkeypox virus (MPXV) has been the most frequent zoonotic infection in many non-endemic states, including the Balkan countries. The recent reemergence of MPOX in Greece, Croatia, Bulgaria, and Romania raised concerns about potential outbreaks in the Balkan countries. This review describes the epidemiology, clinical symptoms and diagnostic methods of the MPOX cases where data was available in the Balkan countries. Understanding the epidemiology is crucial to direct national public health policies for effective tracing as well as vaccination of high-risk groups of the population are essential pillars to control MPOX outbreaks.
Introduction
Monkeypox disease (mpox) is a viral zoonosis caused by the monkeypox virus (MPXV). It belongs to the Orthopoxvirus (OPXV) genus, which also includes the variola virus (VARV), the etiological agent of smallpox. MPXV was first isolated in captive cynomolgus monkeys 1 and was identified as a human pathogen in a 9-month-old baby in the Democratic Republic of Congo (DRC) in 1970. 2 Since the declaration of smallpox-free worldwide at the 33rd World Health Assembly, and the cessation of vaccination campaigns, mpox outbreaks have emerged in the rainforest tropical regions of Central and Western Africa. 3
MPXV includes two major Clades: Clades I and II, of which MPXV Clade I (with Subclades Ia and Ib) was found in Central Africa, and Clade II (with Subclades IIa and IIb) in Western Africa.4,5 These genetic groups exhibit similar symptoms, but Clade I is more severe and has a fatality rate of approximately 10%, compared to 3.6% for Clade II. 6
Although mpox was a sporadic and self-limited disease over the past 50 years, a high incidence has been observed in both Central and Western Africa, and several sporadic outbreaks outside the African continent were detected in the United States (2003, 2021), Israel (2018), United Kingdom (2018), and Singapore (2019). 7 However, no sporadic mpox events or other zoonotic OPXV outbreaks have been documented in the Balkans since the last outbreak of smallpox in 1972, with epicenter in Serbia and in Kosovo, where 175 persons contracted the disease, 35 of whom with a lethal outcome. 8
The Balkan region is located South-East of Europe and is made up of 12 countries, that include Greece, Romania, Slovenia, Serbia, Croatia, Bosnia and Herzegovina, Bulgaria, Montenegro, Kosovo, the Republic of North Macedonia, the Balkan part of Turkey, and Albania.
In response to the 2022 mpox global outbreak, that involved MPXV Clade IIb, coupled with the ongoing outbreaks in Central Africa, that involved MPXV Clade Ib, the World Health Organization (WHO) has recently classified mpox as a Public Health Emergency of International Concern.
From January 2022 up to December 31st, 2024, 124,753 mpox cases were reported to WHO in 128 countries with 272 deaths. In the Balkan countries, Kosovo reported the first case of mpox, whereas Greece registered 22 confirmed cases. 9
Similarly to the global situation, 9 out of 12 Balkan countries registered a total of 333 confirmed cases, whereas in the Republic of North Macedonia, in the Balkan part of Turkey, and in Albania no cases have been reported so far. 9
The recent reemergence of mpox in Greece, Croatia, Bulgaria and Romania raised concerns about the potential outbreaks in the Balkan countries. 10 To provide a better understanding of mpox diffusion in the Balkans, this study aims at discussing the epidemiology, the clinical symptoms and diagnostic methods for the detection of this disease.
Methods
PubMed, Google Scholar, Web of Science, the official website of WHO (https://www.who.int/), European Centre for Disease Prevention and Control (ECDC), European Surveillance System (https://www.ecdc.europa.eu/en/publications-data/european-surveillance-system-tessy), and local health authorities of different countries were inquired.
All of the documents from May 2022 and January 2025, including sociodemographic and clinical data of cases confirmed by polymerase chain reaction (PCR) in the Balkans, were used.
Keywords in English included the terms of mpox cases, epidemiology, clinical outcomes, diagnostic methods, Balkans, Balkan countries, infectious diseases, incidence, mpox incidence, and surveillance programs. Data were extracted from peer-reviewed papers, reports from ECDC or from WHO.
To diagnose a mpox confirmed case, the following criteria were adopted:
one case was defined by WHO as “A person with laboratory confirmed MPXV infection by detection of unique sequences of viral DNA by real-time polymerase chain reaction (PCR) and/or sequencing” 11
to confirm MPXV infection “clinical and epidemiological information should be primarily evaluated, 12 according to WHO case definitions, probable or suspected cases were initially assessed for clinical and epidemiological criteria. Laboratory confirmation is performed only in people who fulfill these criteria”
a confirmation of MPXV infection in suspected cases is performed using an OPXV PCR assay, followed by confirmation of MPXV via PCR and/or sequencing, or positive detection using the MPXV PCR assay. Subsequently, laboratory-confirmed cases should be reported to the WHO. 12 All cases included in this study were confirmed by MPXV real-time PCR”
Results
Sociodemographic characteristics of confirmed mpox cases in the Balkan countries
Since the first case of mpox was confirmed by the UK Health Security Agency at the beginning of May 2022, mpox events have evolved with a remarkable speed also in the Balkan region. On May, 23rd, 2022, Greece documented the first case, followed by Slovenia on May 24th, 2022, other countries on June 2022, 13 and more recently in Kosovo on December 2024.
In our study, we have retrieved detailed information based on clinical data and risk factors in 224 out of 333 confirmed cases between May 2022 and January 2025 (Table 1). Most of these cases belong to the 2022 mpox outbreak, and involve Clade IIb, except for one case of a 30-year-old man from Kosovo, returning from Togo (Africa), and hospitalized on December 24th, 2024, for whom the Clade was not determined.
Distribution of confirmed mpox cases by country of origin.
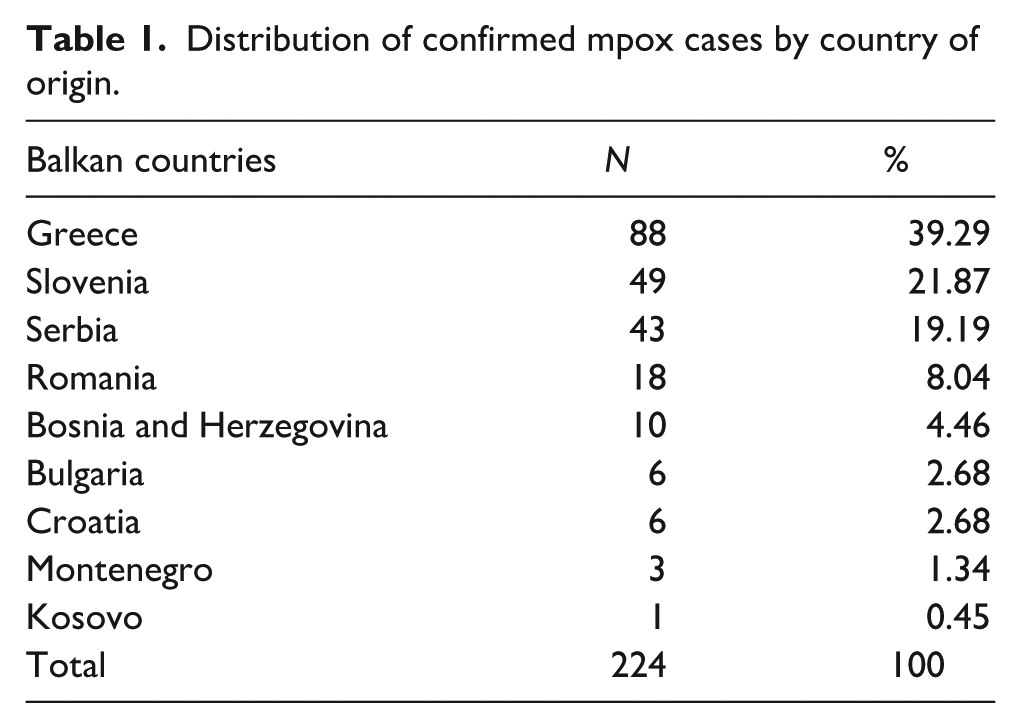
The highest incidence of mpox confirmed cases was in Greece, followed by Slovenia, and Serbia, the reported cases being mainly from the metropolitan areas such as Bucharest, cities of the Attica region and Belgrade. Except for the single case of a 40-year-old female from Montenegro, confirmed cases were males.
Mpox transmission and risk factors
Transmission occurs through contact with wild animals or from inter-human close contacts. 14 During the 2022 mpox outbreak, sexual transmission was documented for the first time, and the majority were men who have sex with men (MSM, 27.30%) and 25.70% were individuals practicing unprotected sex (Table 2). Other high-risk factors were associated to HIV (10.90%) or to traveling people (10.90%). Epidemiological data associated the early reported mpox cases with an international LGBTQI + Pride event held on the island of Gran Canaria, with subsequent transmission chains in several European countries. 15 The majority of cases occurred among males, particularly in MSM, likely due to high-risk sexual behaviors, which facilitated the rapid spread of the virus within interconnected sexual networks. However, confirmed cases were also reported among individuals who did not attend such events, but had recently traveled to endemic regions, such as for the confirmed case from Kosovo. 16
Risk factors, clinical symptoms, and diagnostic methods of mpox cases in the Balkan countries.

NF, not found; data not presented in the article.
-, no reported case; data unavailable in the article or in official sources (WHO or ECDC).
Although it remains unclear whether human immunodeficiency virus (HIV) could be considered as a distinct risk factor, selected studies reported that many of the cases were living with HIV or were people with newly-diagnosed HIV.
Among these multiple factors, the declining smallpox herd immunity remains an important one as the smallpox vaccine can provide cross-protection against mpox in 80%–85% of the cases. 17 Almost half of the confirmed cases (44.64%) were smallpox-vaccine naïve, as only two persons were vaccinated, whereas 54.46% did not have information for their vaccination.
Clinical symptoms
Human mpox has an incubation period of 5–21 days with symptoms that include fever, skin rash, headache, backache, fatigue and mucosal lesions that last 2–4 weeks, and lymphadenopathy. 18 With the fever onset, cutaneous lesions start to develop initially in the face, that spread to other parts of the body, and may also involve the palms of hands and the soles of feet. The lesions evolve at the same stage in every part of the body from macules to papules, vesicles, pustules, and then to crusts and scars.
The clinical evolution of 2022 mpox outbreak showed some differences, with the onset of lesions at various stages of development, and often before the general symptoms, as for the lesions in the anogenital area. 13 The most common symptoms were fever (23.00%) and lymphadenopathy (19.50%). The majority of cases had a rash in the anogenital area, that included penile lesions (14.00%), and anal-perianal lesions (10.50%). A total of 22 patients (4.00%) were hospitalized due to severe complications, but no fatal cases were recorded.
Surveillance system and diagnostic methods
After mpox outbreaks worldwide in 2022, all of the member of WHO institutions, including all the National Public Health centers of the Balkans, followed the guidelines and established an mpox surveillance system to control and prevent disease spreading in the population. A multidisciplinary team, made by Public Health specialists, epidemiologists and clinicians, was formed to implement control and prevention measures.
In several cases, it was difficult to distinguish mpox clinical symptoms from those of other pox-like diseases, especially for cases with an uncommon appearance. It was thus important to train clinicians to distinguish mpox symptoms from those of other diseases. A differential diagnosis for suspected mpox cases includes viral infections that cause rashes, such as herpes simplex 1 (HSV-1) and 2 (HSV-2), varicella, rubella, measles and other febrile rash illnesses. Only two papers from Bulgaria and Serbia mentioned the need of differential diagnosis before testing for mpox (Table 3).
Mpox diagnostic methods used in the Balkan countries for the 224 confirmed cases.
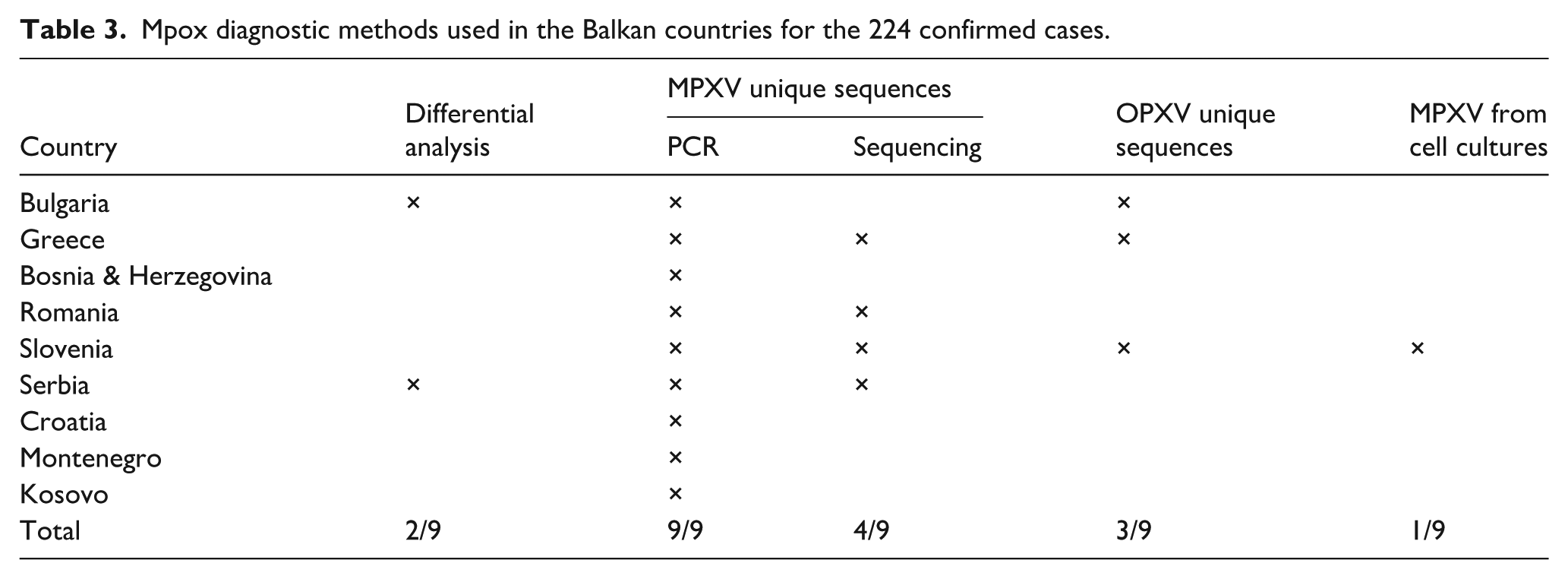
PCR identification of DNA sequences of OPXV and MPXV was used for the unambiguous detection of mpox.
Clinical specimens were often from skin lesions, and from nasal/oropharyngeal positive swabs, but other clinical specimens such as serum, urine, rectal swabs, or seminal fluid were also used.
For the classification of a “mpox positive” case, a PCR-based molecular testing was required by all of the countries. Noticeably, three countries also used a generalized OPXV detection by PCR, which was followed by DNA sequencing of MPXV specific sequences.
As a criterion for confirmed cases, sequencing was used after culturing MPXV in cell lines. Sequencing was used by four out of nine countries, and Slovenia was the only country that reported isolation of the virus in VERO E6 cell line. 19
Different settings were incorporated into the surveillance program within the Balkans. Greece developed an informative setting with a training team that provided guidance information on site by visiting specific laboratories. By the official website of the Greek Public Health Organization, they tried to minimize the spread of fake news, by uploading Frequently Asked Questions and supplying doses of the JYNNEOS vaccine. 20 Slovenia developed and implemented wastewater surveillance between June and September 2023, as MPXV of infected subjects might have entered wastewater through skin lesions, saliva, feces, and urine, via toilets, sinks, and shower drains. 21 Among those detected in Bosnia and Herzegovina, one case was housed in a refugee camp.
Conclusions
Our study is in line with other previously published ones related to mpox distribution, as the sickness occurred mostly among males (99.56%), except for one case of a woman from Montenegro. Likewise, in France almost 30,000 cases (96.3%) were males. 22 However, a multicentric study including 15 countries, among which France, Spain, Italy, Sweden, Denmark, Germany, UK, Switzerland, and other American and African countries, suggested that females infected with MPXV share similar clinical symptoms as males, especially when positive for HIV. 23
Most cases were reported in urban settings such as Belgrade, Bucharest, and cities of the Attica region. These findings may suggest that socio-cultural barriers and stigma can limit access to healthcare, including testing and vaccination, influencing different epidemiological situations in urban and rural settings.
Most mpox cases were detected between June and September 2022, which might reflect the tourism season. Out of the 224 total cases, 10.90% had traveled abroad before the appearance of clinical symptoms and participated to mass gathering events of high-risk groups, like the Gay Pride. 15 However, during the outbreak of African countries, an upsurge of confirmed cases was observed in Greece in the last 2 months of 2024. Notably, Greece is considered as a first gate for African and non-African immigrants.
From 2022 to 2024, 630,170 African and non-African immigrants 24 entering the European Mediterranean countries used the Western Balkan route, as well as Greece and Turkey, 25 as the main pathways to enter Central and Western Europe. The 2022 mpox outbreak overlapped with the war in Ukraine, and contributed to uncontrolled travelling to the Balkan region 25 In fact, 35% Ukrainian people reported they entered Albania in 2022. 26
According to WHO data, refugees and migrants are not included in the national health programs of many countries 27 Refugees are vulnerable to many infectious diseases due to their living conditions in overpopulated camps with poor sanitation, but they lack access to health services. 28 Thus, they are restricted from being tested, diagnosed, receiving treatment, or isolating. The national surveillance system is not notified, which jeopardizes the control and prevention of infectious diseases.
The Balkan national health strategies may formally allow their access to healthcare services, but would only provide limited emergency care. The health status of migrants and refugees in North Macedonia has been fully described by Demiri et al. 29 This global alert suggests the necessity to include refugees and migrants in the national public health program to offer early testing and equity in the access to vaccination. 30
Among the preventive measures, it is fundamental to promote accurate and non-stigmatizing information about MPXV, to increase knowledge and awareness, especially among high-risk groups such as the LGBTQI+ community, and to increase the public positive perception of MPXV vaccines. Although only one case was identified so far from a refugee camp in Bosnia and Herzegovina, 31 the limited data regarding the Balkan region suggest a limited surveillance in refugee camps.
In the majority of the Balkan countries, mpox cases manifested rash, most frequently in the anogenital area, fever, and lymphadenopathy. Some other clinical characteristics were shared with other studies. Studies conducted in the USA 32 report that 46% of the infected patients showed one or more lesions in the genital area as often reported for the Balkan countries. These studies confirm that the anogenital area is the most affected, and suggests that sexual transmission is the most frequent one.
Other studies in the European Union (EU) countries, such as Spain 33 and the Netherlands, 34 also demonstrate that a high percentage of the confirmed cases were co-infected with HIV.
Vaccinations against infectious diseases are the most effective preventive measures. Since the cessation of smallpox vaccination in the early 1980s worldwide, except for France and Egypt that interrupted mass immunization in 1984 35 and Albania in 1987, 36 herd immunity has waned over. Younger age groups are more susceptible, as they have not been exposed to other OPXVs including MPXV in the past, which may have contributed to mpox widespread.
According to the available data, ~90% of the mpox-confirmed cases in the Balkan countries was born from 1980 onwards. 37 Out of 224, 102 (45.54%) knew whether they were vaccinated against smallpox, whereas 122 (54.46%) had no information. In particular, two smallpox-vaccinated persons contracted MPXV infection.
It is important to highlight that the sexual route is a potential vector of disease transmission, as the majority of cases were characterized by rashes in the anogenital areas. Promoting safe sex practices and implementing surveillance programs in different settings can contribute to an effective tracing and identification of MPXV infection and can prevent further transmission of the disease within the community. Vaccination among the highest-risk groups is an essential tool to control and prevent current and future mpox outbreaks, 17 although vaccination against smallpox may not provide a complete cross-protection against MPXV.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
No ethical approval was required, and no new data were created and analyzed, as this study did not involve human participants, human data, or human tissue.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
AM and IM, conceptualization, writing and original draft preparation, review and editing, AR and CDGM, EH, CZ, supervision. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a grant from the Catholic University “Our Lady of Good Counsel,” Tirana, Albania as part of its programs for the promotion and dissemination of scientific research and in part by NATO Science for Peace and Security Programme (SPS). Grant number G5486.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Any other identifying information related to the authors and/or their institutions,funders,approval committees,etc,that might compromise anonymity
Not applicable.