
Abstract
Background:
Tobacco use among adolescents (aged 10–19 years) remains a pressing public health concern, particularly in low-and middle-income countries like Nepal. Despite the presence of tobacco control policies, adolescents continue to access tobacco products. This study assessed effectiveness of a youth-led intervention in shaping adolescents’ attitudes toward tobacco products in Budhanilkantha Municipality, Nepal.
Design and Methods:
Quasi-experimental pre-post study was conducted among 305 adolescents. The intervention, implemented under the “Youth for Tobacco Initiative,” included sensitization, peer-led education, and stakeholder engagement. Data were collected using a structured, self-administered questionnaire, which was completed by students in their classroom setting. The questionnaire assessed sociodemographic characteristics, tobacco exposure, and attitudes toward tobacco use. Changes in attitudes were analyzed using paired t-tests and McNemar’s test, with effect size measured by Cohen’s d. Statistical significance was set at the 5% level.
Results:
Age of the participants ranged between 12 and 18 years (mean age: 15.0 ± 1.32 years). At baseline, 18.7% of adolescents reported tobacco use, and 13.8% reported currently smoking tobacco. Post-intervention, there was a statistically significant improvement in attitudes toward tobacco (mean score increased from 5.86 to 6.12; p = 0.001), with higher recognition of secondhand smoke harms and greater support for public smoking bans. The proportion of adolescents who anticipated smoking in the future declined. Although the effect size was small (Cohen’s d = 0.26), the change was meaningful.
Conclusions:
Youth-led awareness initiatives can positively influence adolescents’ attitudes toward tobacco, particularly through peer education and community involvement. Integrating such interventions into broader, multi-sectoral strategies can enhance their long-term impact.
Keywords
Introduction
Tobacco use remains a significant global public health challenge, contributing to preventable morbidity and mortality worldwide. It has been estimated that tobacco use is responsible for more than 8 million deaths annually, with the vast majority occurring in low- and middle-income countries (LMICs) due to higher consumption rates, weaker tobacco control policies, and limited access to cessation programs.1,2 The adverse effects of tobacco use extend beyond those who actively smoke, as second-hand smoke exposure accounts for approximately 1.2 million additional deaths each year, disproportionately affecting children and adults who do not smoke.1,3 Nearly half of all children globally breathe air polluted by tobacco smoke, and 65,000 children die annually from illnesses related to secondhand smoke exposure, reinforcing the urgent need for effective tobacco control measures. 1
Adolescents (aged 10–19 years), represent a particularly vulnerable group, as early exposure to tobacco and nicotine significantly increases the risk of long-term nicotine dependence.4,5 The global prevalence of adolescent tobacco use is estimated to be 19.33%, with a higher prevalence among males (23.29%) compared to females (15.35%). 6 The initiation of tobacco use during adolescence is concerning because it sets the foundation for lifelong addiction, making it crucial to implement preventive measures during this developmental stage. 5 Although high-income countries have made progress in reducing adolescent tobacco use through stringent regulations and widespread awareness campaigns, the prevalence remains high in many LMICs, where weaker enforcement mechanisms and sociocultural acceptance of tobacco use contribute to continued consumption.6–8 The harmful effects of tobacco on adolescents extend beyond addiction and are associated with severe health issues, such as gingivitis, dental caries, mental health problems, and periodontal disease, further exacerbating the health burden associated with smoking and smokeless tobacco products.6,9 The Southeast Asian region accounts for approximately 280 million people who use smokeless tobacco and 11 million adolescents who use tobacco, making up nearly 30% of the global burden of adolescent tobacco consumption. 10 The prevalence of tobacco use among adolescents remains particularly high in many LMICs, with smoking rates reaching up to 46% among male adolescents in countries like Laos and Indonesia, reflecting broader societal smoking patterns.11,12 This persistence of tobacco use in specific regions underscores the need for targeted interventions that address the unique sociocultural and economic factors influencing tobacco consumption patterns.
In Nepal, comprehensive national data on adolescent tobacco use remain limited. However, findings from the Global Youth Tobacco Survey (GYTS) conducted in 2007 revealed that 7.9% of Nepalese students aged 13–15 years had smoked cigarettes at least once, while 8% had used other tobacco products. 13 More recent studies indicate that the prevalence of tobacco use among adolescents has increased significantly, with estimates suggesting that approximately 20.5% of Nepalese adolescents currently use tobacco in some form. 6 Gender disparities in tobacco use remain prominent in Nepal. According to a nationally representative survey of individuals aged 15–49 years, 52.3% of males and 8.4% of females reported using some form of tobacco. Among these individuals, 27.4% of males and 5.5% of females reported smoking cigarettes, while 40.1% of males and 3.8% of females reported using smokeless tobacco. 14 Within the adolescent subgroup (aged 15–19 years), 15.8% of males and only 0.5% of females were identified as current smokers. 14 The health consequences of tobacco use in Nepal align with global trends, as long-term smoking is a significant risk factor for respiratory diseases, cardiovascular diseases, and various forms of cancer. 1 Smoking has been found to reduce life expectancy by an average of 10 years, further highlighting the severity of the public health implications associated with tobacco use. 15
Nepal has introduced several policies to regulate tobacco use, particularly among young people. The Tobacco Product Control and Regulatory Act 2011 aims to reduce tobacco consumption by prohibiting the sale of tobacco products to minors and restricting tobacco sales within 100 m of educational institutions. 16 In addition to these regulatory measures, the act also bans the advertisement and promotion of tobacco products through various media channels, including television, radio, newspapers, and online platforms. 17 However, despite these legislative efforts, there are considerable gaps in implementation and enforcement. Adolescents continue to access tobacco products with ease, particularly in areas where vendors do not adhere to age verification protocols. 16 A lack of awareness about tobacco control laws further exacerbates the issue, as many students are uninformed about existing regulations, and enforcement mechanisms remain inadequate. 18
Recognizing the limitations of existing tobacco control policies, the Youth for Tobacco Initiative has emerged as a promising intervention to curb adolescent tobacco use in Nepal. This program aims to prevent tobacco initiation among adolescents by fostering negative attitudes toward tobacco products through peer-led health education programs, advocacy efforts, and interactive awareness campaigns. Adolescents play an active role in these interventions, engaging their peers through workshops, discussions, and media campaigns designed to shift social norms around tobacco consumption. Such peer-led programs have been proven effective in high-income settings as well, such as the ASSIST (A Stop Smoking In Schools Trial) program in England and Wales trained influential adolescents to discourage tobacco use among peers, significantly reducing smoking prevalence by up to 22% at follow-ups up to 2 years. 19 Findings from a mixed-methods evaluation of ASSIST in Scotland showed that the intervention was feasible and acceptable in new contexts, with added benefits such as improved communication skills and ripple effects within the community. 20
The Theory of Planned Behavior (TPB) suggests that attitudes, social norms, and perceived behavioral control significantly influence behavioral intentions. Youth-led awareness programs align with this framework by promoting negative perceptions of tobacco use, reinforcing social norms against smoking, and empowering adolescents to resist peer pressure. 21 A comprehensive review of 66 adolescent tobacco cessation trials indicates that classroom-based and peer-influenced approaches can increase quit rates, further reinforcing the utility of such interventions. 22 These findings provide a solid foundation to adapt and scale peer-led strategies within LMICs like Nepal, where culturally appropriate, youth-empowered models can fill enforcement and awareness gaps. This study aims to assess the prevalence of tobacco product use among adolescents in Nepal while evaluating the impact of peer-led health education interventions on shaping their attitudes toward tobacco products. By identifying barriers that hinder the effectiveness of youth-led initiatives, this research seeks to provide evidence-based recommendations for strengthening adolescent tobacco prevention strategies. The findings have important policy implications for enhancing youth-focused tobacco control efforts in Nepal and other countries with similar socio-cultural contexts. Given the rising prevalence of adolescent tobacco use, investing in youth-led interventions has the potential to yield long-term public health benefits by reducing tobacco-related morbidity and mortality.
Method
Study design and setting
This study employed a quasi-experimental, pre-post intervention design without a control group to assess the effectiveness of a youth-led awareness initiative on adolescents’ attitudes toward tobacco use. The study was conducted in Budhanilkantha Municipality, Nepal, among school-going adolescents. The intervention was part of the Youth for Tobacco Initiative, a community-driven program aimed at reducing tobacco use among young people through peer-led education and awareness campaigns. Baseline data were collected between 27 December 2024 and 5 January 2025. The youth-led intervention was implemented over a 2-week period from 6 January to 19 January 2025. Post-intervention data collection was conducted from 11 to 27 March 2025, approximately 7 weeks after the completion of the intervention
Sample size determination
The sample size for this study was determined using the formula for comparing means (n = ((Zα/2+Zβ)2 × 2 × σ2)/d2), where Zα/2 = 1.96 corresponds to a 95% confidence level, Zβ = 0.84 accounts for 80% power, σ represents the estimated standard deviation of the outcome variable, and d denotes the minimum expected difference between pre-and post-intervention scores. Given the absence of prior intervention studies reporting the standard deviation of attitude scores toward tobacco use among adolescents σ was assumed to be 1. The expected effect size was set at 0.5, representing a moderate effect. Substituting these values, a required sample size of 62 participants per group. Since five schools were randomly selected from a total of 10 public schools using the lottery method, the sample size was adjusted by multiplying the required number of participants per group (62) by five schools, resulting in a total of 310 participants. Adolescents enrolled in grades 8, 9, and 10 in these schools were selected consecutively until the required sample size (62 per school) was reached, totaling 310 participants. A total of 305 adolescents provided their complete responses in both pre and post-test and included in the final analysis.
Intervention program
The “Youth for Tobacco Initiative” was co-developed with youth leaders trained in tobacco-related health risks, behavioral change communication, and advocacy skills. Peer educators conducted a series of interactive workshops, storytelling sessions, street dramas, and gamified learning activities, complemented by digital media messages shared via school networks and social platforms. The intervention was systematically implemented across five selected public schools within Budhanilkantha Municipality, Nepal. The program was facilitated by a research team comprising public health experts, educators, and trained student leaders, ensuring comprehensive monitoring and evaluation throughout the process. The intervention consisted of three key components: sensitization, youth-led advocacy and education, and stakeholder engagement.
Sensitization program
The intervention began with a sensitization program led by the research team to introduce the Youth for Tobacco Initiative to schoolteachers, parents, and students. The sessions focused on increasing awareness about the harmful effects of tobacco consumption, existing tobacco control policies, and the role of youth in preventing tobacco use. These sessions were conducted through interactive presentations, discussions, and multimedia resources to ensure participant engagement and comprehension.
Youth-led advocacy and education program
A youth-led advocacy and education component was implemented after the sensitization program. Three students from each school were selected as peer leaders based on their leadership skills and willingness to participate. Each school also designated one teacher as a facilitator to guide and support the peer leaders. These selected students underwent structured training sessions conducted by public health professionals, equipping them with knowledge of tobacco-related health risks, the legal framework governing tobacco use, and effective peer education strategies. After completing their training, the peer leaders conducted various advocacy activities within their schools. These activities included classroom sessions where they educated their fellow students on the dangers of tobacco, interactive workshops, quiz competitions, exhibitions, and role-playing exercises. Demonstrations and gamified learning activities were integrated to maintain student engagement and make learning more impactful. The peer leaders also initiated social media awareness campaigns and poster competitions to spread anti-tobacco messages beyond the classroom setting. The intervention program was closely monitored through regular check-ins with peer leaders and facilitators to assess participation levels and knowledge retention among students.
Community stakeholder engagement
To ensure the sustainability of the intervention, community stakeholder engagement was a key component. Meetings were conducted with school administrators, local government officials, municipal authorities, healthcare professionals, and representatives from non-governmental organizations working on tobacco control to discuss long-term strategies for integrating tobacco prevention into school curricula. Parents and community leaders were also engaged in dialog sessions to reinforce the importance of collective efforts in preventing adolescent tobacco use. In addition to these discussions, key stakeholders actively participated in youth-led activities, attending workshops, judging competitions, and providing mentorship to students to further strengthen their advocacy efforts. Feedback was collected from teachers, students, and community stakeholders to monitor the progress and effectiveness of the intervention. The research team provided ongoing support and facilitated discussions to address any challenges encountered during implementation.
Data collection
Data were collected using a structured, self-administered questionnaire at two-time points: baseline (pre-intervention) and post-intervention. Both rounds of data collection were conducted in the students’ regular classroom settings during dedicated 1-hour sessions, coordinated with the support of schoolteachers to minimize disruption to academic schedules. The questionnaire was divided into four sections to ensure comprehensive data collection. The first section captured sociodemographic information, including age, gender, ethnicity, parental education, and employment status. The second section focused on environmental exposure, assessing parental and peer tobacco use, exposure to anti-tobacco messages, and school-based tobacco education. The third section measured attitudes toward tobacco use through a Likert-scale questionnaire adapted from validated tobacco perception scales. This section evaluated perceptions of smoking, the perceived harm of secondhand smoke, and support for smoking bans. The final section included self-reported tobacco use behaviors to monitor changes before and after the intervention. The questions were based on the Global Youth Tobacco Survey (GYTS). 23 To ensure data reliability, the questionnaire was pre-tested among a subset of students from non-participating schools to refine wording and clarity. Data collection was facilitated by trained enumerators who provided clear instructions and monitored the process to ensure completeness. To maintain confidentiality while ensuring accurate matching of pre- and post-test responses, each participant was assigned a unique identification code at baseline. This code was used on all questionnaires instead of the participant’s name. A confidential linkage file (containing participants’ names, school, grade, and roll number mapped to their assigned code) was securely maintained by the research team and was not shared beyond the core investigators. The primary assessment focused on changes in adolescents’ attitudes toward tobacco use, specifically their intention to use tobacco products and their perceived harm from secondhand smoke.
Assessment of attitudes toward tobacco use
The attitude of adolescents toward tobacco use was assessed based on a structured questionnaire developed in consultation with experts in public health, health promotion and education, and community medicine. The tool was developed in reflection of the Global Youth Tobacco Survey (GYTS) tool and focused on capturing participants’ perceptions of smoking, awareness of tobacco-related harm, and their stance on tobacco control measures. The attitude assessment scale comprised seven items, each rated on a binary response format (Yes/No). The items assessed key domains, including susceptibility to smoking, perceived harm of secondhand smoke, and support for smoking bans. Higher scores indicated stronger anti-tobacco attitudes. The detailed questionnaire used in this study is attached as supplementary document.
Statistical analysis
The data were entered through EpiData and exported to SPSS version 16 for further analysis. Descriptive statistics, including frequencies and proportions, summarized categorical variables such as sociodemographic characteristics and different tobacco use patterns among adolescents. The paired t-tests were used to compare pre-and post-intervention attitude scores, while McNemar’s test was applied for paired categorical comparisons. Effect sizes were calculated using Cohen’s d to assess the magnitude of the intervention effect. A significance level of p < 0.05 was considered statistically significant.
Ethical approval and informed consent
Ethical approval for this study was obtained from the Ethical Review Board of the Nepal Health Research Council, Kathmandu, Nepal (Ref. No: 1274; Proposal ID: 420_2024). With the support of the schools, parents were oriented about the study and provided with written informed consent forms, which they returned with either a signature or thumbprint. Written informed assent was obtained from the adolescents at school after explaining the study procedures. Participation was voluntary, and participants had the right to withdraw from the study at any time without consequence. The confidentiality and anonymity of participants were strictly maintained throughout the study.
Result
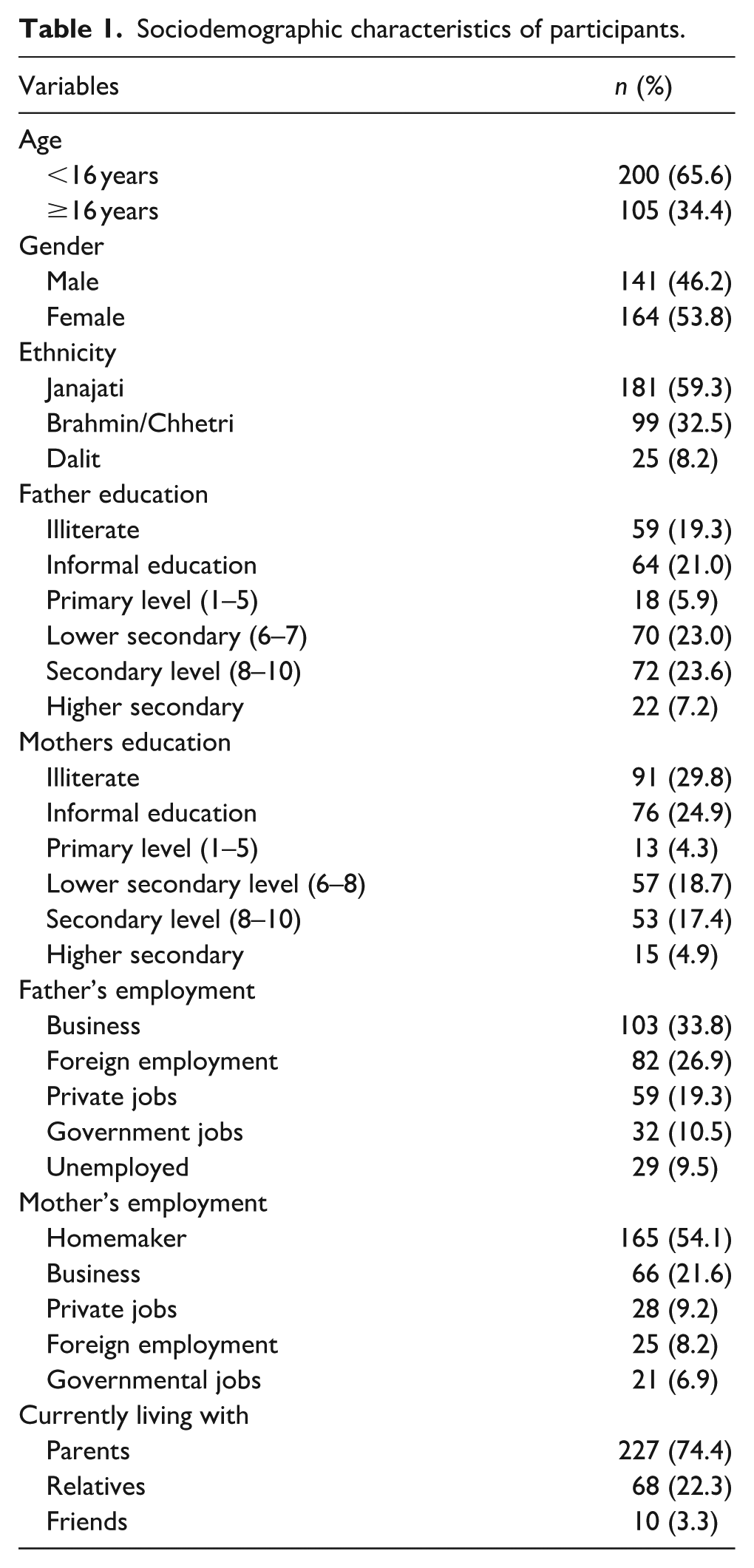
A total of 305 adolescents participated in the study, with ages ranging from 12 to 18 years (mean age: 15.0 ± 1.32 years). The sample comprised almost equal proportion of female and male students at 53.8% and 46.2%, respectively. In terms of ethnicity, Janajati adolescents made up the largest proportion (59.3%), followed by Brahmin/Chhetri (32.5%) and Dalit (8.2%). In terms of parental education, 19.3% of fathers and 29.8% of mothers were illiterate, while 23.6% of fathers and 17.4% of mothers had secondary-level education. Regarding household composition, 74.4% of participants lived with their parents, 22.3% with relatives, and 3.3% with friends (Table 1).
Sociodemographic characteristics of participants.
The overall prevalence of tobacco use among adolescents was 18.7% (95% CI: 14.7–23.4), while 13.8% (95% CI: 10.4–18.1) were classified as people who actively smoke. Lifetime smoking was reported by 7.9% of participants, with 5.6% identified as currently consuming cigarette. Additionally, 4.6% reported bidi smoking, while 7.2% used other forms of smoking products. The use of smokeless tobacco was lower, with 3.0% consuming Gutka, 6.6% using pan masala, and 2.0% consuming khaini (Table 2).
Prevalence of tobacco use among students.

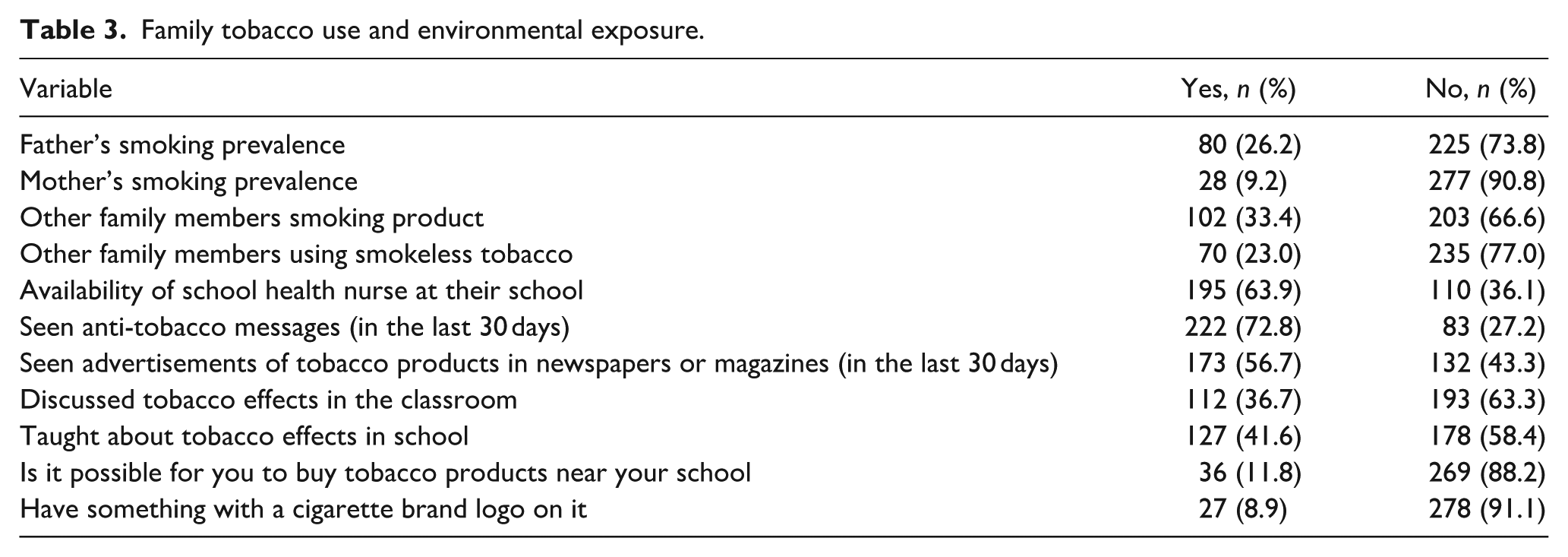
Parental smoking prevalence was notable, with 26.2% of fathers and 9.2% of mothers identified as individuals who use tobacco through smoking. Among other family members, 33.4% reported smoking tobacco, while 23.0% used smokeless tobacco products. The majority of the studies (72.8%) reported being exposed to anti-tobacco messages through mass media in the last 30 days. However, only 36.7% had discussed tobacco effects in class, and 41.6% had received formal education about the risks associated with tobacco use (Table 3).
Family tobacco use and environmental exposure.
Following the intervention, negative attitudes toward tobacco products increased, as evidenced by greater recognition of the harms of secondhand smoke and stronger support for smoking bans. The proportion of participants who stated that they would accept a cigarette from a friend declined from 2.3% to 1.3%, while those who believed they would smoke in the next 12 months decreased from 2.3% to 1.6%. Similarly, the proportion of adolescents who thought they would be smoking in 5 years decreased from 5.2% to 2.0%. Recognition of the harmful effects of secondhand smoke increased from 77.7% to 87.9%, and support for banning smoking in enclosed public spaces rose from 57.4% to 63.6%. Meanwhile, perceptions regarding smoking’s impact on attractiveness remained largely unchanged. The overall attitude score showed an increase from 5.86 (SD = 0.95) to 6.12 (SD = 1.02). The paired t-test indicated a statistically significant improvement (p = 0.001), and the effect size measured using Cohen’s d was 0.26, indicating a small effect of the intervention (Table 4).
Comparison of attitude toward tobacco products before and after intervention.

The Paired t-test.
The Wilcoxon signed-rank test after checking normality by Shapiro-Wilk test.
Items A1–A4 are reverse-coded (Yes=0, No=1), while A5–A7 are coded normally (Yes=1, No=0); higher scores indicate stronger anti-tobacco attitudes
Discussion
This study evaluated the effectiveness of a youth-led awareness initiative in shaping adolescents’ attitudes toward tobacco use in Budhanilkantha Municipality, Nepal. The findings indicate that peer-led educational interventions can contribute to a shift in adolescent perceptions regarding tobacco, particularly by increasing awareness of secondhand smoke risks and strengthening support for smoking bans. The study found that 18.7% of adolescents had used tobacco products, while 13.8% were actively smoking. These findings are comparable to those from previous studies conducted in Nepal. A study in Dharan, Nepal, reported that 19.7% of adolescents had used tobacco products, 24 while research from Saptari found a slightly higher prevalence if tobacco consumption among adolescent at 24%. 25 Similarly, the study based on Kaliya Nepal reported adolescent tobacco use prevalence of 25.3%. 26 The observed prevalence in this study is also aligned with national estimates from the Global Youth Tobacco Survey (GYTS) Nepal Report 2011, which found that 20.4% of adolescents had ever used tobacco, while 9.0% were actively smoking. 13 The Tobacco Atlas further estimates that 4.5% of males and 2.1% of females aged 10–14 years smoke in Nepal, reinforcing the urgency of targeted tobacco prevention efforts. 27 In a broader regional and global context, adolescent tobacco use in Nepal appears comparable to other South Asian nations. In India, adolescent tobacco use stands at 6.9%, 28 while in Bangladesh, it reaches 19.0%. 29 A systematic review of 20 studies published between 2000 and 2018, reported adolescent smoking prevalence ranging from 5.9% to 49% across India. 30
The study also identified gaps in exposure to tobacco-related education and prevention efforts among Nepalese adolescents. While 72.8% of adolescents reported seeing anti-tobacco messages through mass media, only 41.6% had received formal education on the risks of tobacco use, and just 36.7% had discussed tobacco effects in classrooms. This limited exposure to structured tobacco education aligns with previous findings from Nepal, where only 12% of school personnel had received formal training to prevent youth tobacco use. 31 For instance, teachers’ anti-tobacco attitudes can positively influence students’ perceptions and behaviors regarding smoking. 32 The role of parental smoking in shaping adolescent tobacco attitudes has been widely documented. In this study, 26.2% of fathers and 9.2% of mothers reported to smoke, suggesting a potential pro-tobacco influence within the household. Previous studies in Nepal and South Asia have shown that adolescents with smoking parents and poor parenting are significantly more likely to have favorable attitudes toward tobacco use.26,33,34 Despite this exposure, the study demonstrated a positive shift in anti-tobacco perceptions following the intervention, indicating that school-based interventions can counteract some of the parental influences that contribute to adolescent smoking initiation.
As per the fifth edition of the WHO global report on trends in prevalence of tobacco use 2000–2030, in SEA Region only India and Nepal are likely to achieve at least a 30% relative reduction in tobacco use by 2025, assuming they are able to continue implementing tobacco control measures. 10 Nepal has established comprehensive tobacco control policies, including the Tobacco Product Control and Regulatory Act (2011) and participation in the WHO Framework Convention on Tobacco Control (FCTC). Key measures such as graphic health warnings, advertising bans, and public smoking restrictions have been implemented. 16 The act also prohibiting the sale of tobacco products to minors and within 100 m of educational institutions. 17 However, in this study 11.8% student reported access to tobacco products nearby the premises of their school. Similar observation was made in Arghakhanchi district, where only 14.7% of retailers were found in compliance with the provision of not selling tobacco to minors and only 5.8% retailers were found restricting sale of loose cigarettes. 35 Adolescents can easily purchase tobacco products from shops near schools, often without being asked for their age. 16 Many students are unaware of tobacco control policies, and even fewer are prevented from buying tobacco due to age restrictions. 18 Thus, enforcement of the regulations remains a critical challenge, particularly in maintaining smoke-free environments and ensuring the effective integration of tobacco education in schools. The findings of this study support stronger implementation of school-based tobacco education, as mandated by Nepal’s National Health Education, Information, and Communication Strategy. While mass media campaigns are effectively reaching adolescents, the lack of structured classroom-based education limits long-term prevention efforts.
The study demonstrated a statistically significant improvement in adolescents’ anti-tobacco attitudes following the intervention. The overall attitude score increased from 5.86 (SD = 0.95) pre-intervention to 6.12 (SD = 1.02) post-intervention, with a small but meaningful effect size (Cohen’s d = 0.26). Notable changes included an increase in the recognition of secondhand smoke risks (77.7%–87.9%) and greater support for banning smoking in enclosed public spaces (57.4%–63.6%). The proportion of students willing to accept a cigarette from a friend declined from 2.3% to 1.3%, and those who believed they would smoke in the next 5 years decreased from 5.2% to 2.0%. However, certain perceptions, such as the belief that smoking affects attractiveness, remained largely unchanged, indicating that some attitudes may be more resistant to change. The effectiveness of school-based tobacco prevention programs has been documented in previous studies.36–38 Adolescents are engaged as active participants in the fight against tobacco, empowering them to lead anti-tobacco campaigns in their schools and communities. Research from India found that students who received school-based tobacco education were significantly more likely to have negative attitudes toward tobacco and less likely to use it. 39 Similarly, a study in Indonesia indicated that health education interventions improved knowledge, attitude, and self-efficacy in smoking prevention. 40 Research from China, involving a 1-year intervention in 15 schools, also demonstrated positive effects on students’ knowledge, attitudes, and behaviors toward tobacco use. 41
Strengths and limitations
This study has several notable strengths. The findings suggest that youth-led, peer-driven interventions are an effective strategy for engaging adolescents in tobacco control efforts in Nepal. By positioning students as change agents within their schools and communities, this initiative demonstrated measurable improvements in knowledge and behavior. A key strength of this study is its co-designed, youth-led, peer-to-peer intervention model, which has been shown in other settings to improve both engagement and message retention among adolescents. Bias mitigation in this non-randomized intervention was achieved through a standardized, youth-led curriculum consistently delivered by trained facilitators across all schools. Furthermore, rigorous and uniform data collection procedures, employing piloted questionnaires at both pre- and post-intervention, minimized measurement bias. Additionally, the study utilized a pre-post design, enabling direct measurement of changes in knowledge and attitudes. The sample was drawn from multiple schools, enhancing contextual relevance and generalizability to similar urban school environments within Nepal.
While this study provides valuable insights, several limitations should be acknowledged. First, the study employed a pre-post design without a control group. This decision was influenced by logistical and ethical constraints within the school setting, where withholding potentially beneficial educational content from certain students was not considered appropriate. These limitations restrict the strength of causal inferences, as the absence of a control group limits the ability to attribute observed changes in attitudes and susceptibility solely to the intervention. External factors such as concurrent health campaigns, media exposure, or parental influence may have also contributed to these changes. Future studies should consider employing controlled or randomized designs where feasible with longer follow-up periods to assess the sustained impact of youth-led interventions on both attitudes and behavioral outcomes. Second, the reliance on self-reported data may introduce recall bias and social desirability bias, where participants could have underreported tobacco use or overreported positive changes in attitudes due to perceived expectations. Third, the study was limited to a single municipality, potentially limiting representation of adolescents in rural or socio-economically diverse areas of Nepal. We did not conduct sensitivity analyses to compare these students with those who completed both assessments. While the small number is unlikely to have introduced significant bias, we acknowledge this as a limitation. Although advanced analytical methods such as repeated measures ANOVA are often recommended for studies with multiple time points, our study involved only two measurements and a single group, making such analyses unsuitable. Future research should explore longitudinal and geographically diverse designs to assess better whether attitude changes translate into sustained behavioral modification over time.
Implications and recommendations
The findings suggest that school-based, youth-focused interventions can play a role in improving adolescents’ attitudes toward tobacco in Nepal. While the intervention demonstrated a measurable impact in changing tobacco-related attitudes and susceptibility, a more comprehensive, multi-sectoral approach is essential for sustained behavioral change. This includes active engagement from schools, families, health systems, and policymakers. Strengthening life skills–based school curricula, enforcing school-level and national tobacco control policies, and incorporating community and parental education into adolescent-focused prevention strategies could further amplify the long-term effectiveness of such youth-driven initiatives. Scaling up similar awareness activities through integration with existing school health programs could strengthen tobacco prevention efforts. However, future studies should incorporate more rigorous evaluation methods, including randomized controlled trials, longer follow-up periods, and advanced analytical techniques to strengthen the evidence base and assess the sustainability of intervention effects.
Conclusion
This study highlights the potential of youth-led awareness initiatives in shaping adolescent attitudes toward tobacco use. While the intervention demonstrated measurable improvements in anti-tobacco perceptions, a multi-sectoral approach involving schools, families, and policymakers is essential for sustaining long-term reductions in adolescent tobacco susceptibility. Strengthening school curricula, enforcing tobacco control policies, and incorporating parental education into prevention strategies will be crucial in ensuring that tobacco prevention efforts yield lasting public health benefits.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251380778 – Supplemental material for Effectiveness of Youth-Led awareness and advocacy intervention in shaping adolescents’ attitudes toward tobacco products in Nepal: A quasi-experimental study
Supplemental material, sj-docx-1-phj-10.1177_22799036251380778 for Effectiveness of Youth-Led awareness and advocacy intervention in shaping adolescents’ attitudes toward tobacco products in Nepal: A quasi-experimental study by Sandeepa Karki, Dhurba Khatri, Shishir Paudel, Yamuna Chhetri, Ganesh Shetty, Prashant Khadka, Pratikshya Pandey and Bhagawan Koirala in Journal of Public Health Research
Footnotes
Acknowledgements
We would like to express our heartfelt gratitude to all the schools, students, parents, and local representatives of Budhanilkantha Municipality for their generous cooperation and unwavering support throughout the course of this study. We are especially thankful to the peer leaders, whose dedication, enthusiasm, and commitment played a vital role in the successful implementation of the Youth for Tobacco Initiative.
ORCID iDs
Author contributions
SK: conceptualization, project administration, fund acquisition, validation, methodology, and writing–review and editing. DK: conceptualization, investigation, project administration, methodology, and writing–review and editing. SP: conceptualization, methodology, data analysis, visualization, and writing–original draft, writing–review and editing. YC: investigation, project administration, writing–review and editing. GS: investigation, data analysis, writing–review and editing. PK: investigation, data analysis, writing–review and editing. PP: conceptualization, project administration. BK: supervision, and writing–review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by AstraZeneca (Request ID 89903437). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data are within the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.