
Abstract
Background:
Dengue fever, a viral infection transmitted by Aedes mosquitoes, has emerged as a global public health concern according to the World Health Organization (WHO). Given the geographical proximity of Iran to countries that have reported outbreaks of this disease in recent years, this issue needs careful attention.
Design and methods:
The present study aims to identify the knowledge, attitudes, and practices of rural populations concerning dengue fever in Fars Province, southern Iran.
Methods:
A cross-sectional study was conducted over 2 months, from October to December 2024, involving 17 rural regions and encompassing a total of 653 households. The data were collected using a questionnaire designed to assess knowledge, attitudes, and practices regarding dengue fever.
Results:
Of the 653 individuals participating in the study, 370 were male and 283 were female. The overall average scores, along with their standard deviations, for the rural population’s knowledge (10.76 ± 2.10 out of 15), attitude (13.65 ± 2.90 out of 20), and practice (8.24 ± 1.70 out of 12) regarding dengue fever were at moderate levels. Pearson’s correlation coefficient analysis indicated a direct and statistically significant relationship between knowledge, attitudes, and practices. The findings revealed a substantial positive association between the participants’ knowledge and their attitudes (r = 0.47, p < 0.001), as well as a strong direct relationship between knowledge and practices (r = 0.51, P<0.001). Furthermore, a notable positive correlation was observed between attitudinal variables and practical behaviors (r = 0.45, p < 0.001).
Conclusion:
Overall, the knowledge, attitude, and practice of the rural population regarding dengue fever were found to be moderate. Therefore, it is recommended that health system policymakers should adopt suitable approaches, such as ensuring comprehensive public health education for all, creating educational materials, and enhancing awareness campaigns. Effective strategies for mitigating and controlling the spread of dengue fever depend on public knowledge and attitude changes, along with appropriate measures for successful disease control.
Introduction
Dengue fever, a mosquito-borne viral infection, has become endemic in most tropical and subtropical regions worldwide. 1 In 2009, the World Health Organization (WHO) declared that dengue fever was an international public health concern subject to International Health Regulations, due to the global health threat posed by its rapidly spreading epidemics worldwide. These regulations urge countries to implement specific measures to prevent the dissemination of this disease. 2 Thus, assessing public perception and behavior regarding the Aedes mosquito has become a significant issue in preventing dengue fever outbreaks. 3 According to the World Health Organization (WHO), dengue fever is endemic in over 100 countries, predominantly in tropical and subtropical areas. 4 Annual estimates suggest that, of the 400 million individuals who contract dengue infection, approximately 100 million manifest clinical symptoms, with 22,000 succumbing to severe dengue. 5 The highest incidences are reported in Southeast Asia, the Western Pacific, and the Americas, particularly in countries such as India, Brazil, Vietnam, and the Philippines. 6 Thus, dengue poses a significant global public health challenge. It is imperative to find out the knowledge, attitudes, and behaviors of the community regarding dengue fever for developing effective prevention and control strategies. 7 In viral disease epidemics, the awareness and attitudes of the population become further important. Identifying the public’s knowledge, attitude, and practices (KAP) regarding dengue can help governments define and address local barriers to implementing vector control. 8
Community integration in dengue control requires assessments of knowledge, attitudes, and practices (KAPs). 9 A recent study conducted in Malaysia revealed that the general population possessed only moderate knowledge and revealed poor attitudes as well as practices concerning dengue prevention. The researchers identified that a significant percentage held misconceptions about dengue vector control, which resulted in a false sense of security while neglecting necessary preventive measures. 10 Similarly, a study by Asadian (2024) on the knowledge, attitudes, and behaviors of Hormozgan Province residents in Iran has concluded that more targeted educational interventions are needed by the general population aiming at enhancing both knowledge and preventive behaviors regarding Aedes mosquitoes and dengue fever. 11 Identifying the knowledge, attitude, and performance of the general population is one of the effective factors in preventing dengue fever. In this regard, Kumaran et al. 12 conducted a study on the knowledge, attitude, and practices in an urbanized residential area of Cambodia. They concluded that there was a need to strengthen health promotion activities to enhance the knowledge that forms the foundation for preventive practices as part of the strategy to control dengue fever outbreaks. 12
Background in Iran
In Iran, although dengue fever is not classified as a high-risk disease, sporadic cases have emerged, particularly in provinces bordering countries with higher transmission rates. On June 14, 2024, the Ministry of Health and Medical Education (MoHME) in Iran announced the first two cases of locally transmitted dengue fever in the country. The confirmed cases were reported in Bandar-Lengheh, located in Hormozgan Province in southern Iran. 13 The unique geographical and sociopolitical landscape of Iran presents both challenges and opportunities for dengue management. The proximity of our country to regions that have experienced significant dengue outbreaks, including Southeast Asia and the Arabian Peninsula, raises concerns about virus importation and the potential for local transmission. 14 Further, public health infrastructure of Iran, which has historically focused on controlling diseases such as malaria and leishmaniasis, needs to adapt to the emerging threat of dengue fever. 15
Dengue KAP surveys are typically performed in communities where dengue is endemic or where there have been ongoing or recent outbreaks. As the risk of dengue spreads to new regions, understanding the population’s knowledge base can help better design and implement community-based interventions. Given the importance of the issue and the very few studies that have been conducted in this area, it is recommended that the present study should also be conducted in different countries to develop knowledge translation. Examination of the knowledge, attitude, and performance in the field of dengue fever disease can help policymakers and managers of the health system to implement control plans and prevent the outbreak of the disease. Thus, since no study has been conducted in Fars province in the south of Iran in this field and that there are research gaps which need to be filled, the present study aimed to identify he knowledge, attitudes, and practices of the rural population in Fars Province, Southern Iran, regarding dengue fever.
Design and methods
This cross-sectional multicenter study was undertaken over three months from October to December 2024.
Sample size
For the sample size calculation, the formula for the proportion in the population is p = 0.50, based on the study by Selvarajoo et al., 16 which found that the total participants had good knowledge. 16 Considering α = 0.05 (z = 1.96) and d = 0.05, the calculation is based on the following formula:

The minimum sample size was calculated to be 384. To enhance the credibility of the findings, the researchers enrolled 700 participants. Finally, a total of 653 participants filled out and returned the questionnaires, thus yielding a response rate of 93.28%.
Data collection process
The studied population consisted of 653 residents of 17 villages at Fasa city, in Fars Province, Southern Iran, who were selected using a cluster sampling method. The researcher obtained a list of households by visiting the health centers in each village. Then, each household, the one study participants were selected using simple random sampling method regardless of family size to minimize response biases and ensure all households had an equal chance of being selected. Household were invited to participate in the study after we obtained their informed consent. If the household was not present or refused to participate, the next household was included until we reached the sample size required.
Inclusion and exclusion criteria
Inclusion criteria were willingness to participate and ability to communicate, while the sole exclusion criterion was unwillingness to continue participation for any reason.
Data collection
The data collection instrument consisted of two parts: (1) demographic characteristics, including age, gender, marital status, education level, and occupation; and (2) a questionnaire evaluating individuals’ knowledge, attitudes, and practices regarding dengue fever.
The questionnaire assessing individuals’ knowledge, attitudes, and practices regarding dengue fever was developed by Asadian et al. in Iran. 11 The knowledge, attitudes, and practices questionnaire, designed to measure the respondents’ self-care behavior against Aedes mosquito bites, consists of five knowledge questions, four attitude questions, and four practice questions. Knowledge questions are scored using a three-point Likert scale (correct, incorrect, I don’t know), with scores ranging between 5 and 15. Based on the expert consensus of the research team, scores of 5–7 indicate poor knowledge, 8–12 moderate knowledge, and 13–15 good knowledge. Attitude questions are scored using a five-point Likert scale ranging from strongly agree (5) to strongly disagree (1), with score ranges of 4–20. Based on the expert consensus of the research team, scores of 4–10 poor attitudes, 11–14 moderate attitudes, and 15–20 good attitudes. Practice questions are scored using a three-point Likert scale (never = 1, sometimes = 2, always = 3), with scores ranging from 4 to 12. According to the expert consensus of the research team, scores of 4–6 reflect poor practices, 7–9 moderate practices, and 10–12 good practices. The reliability of the questionnaire was reported with a Cronbach’s alpha of 0.74 in Azadian, et al.’s study, with an overall correlation coefficient of 0.94, demonstrating acceptable reliability. In the present study to measure content validity, we determined the Content Validity Ratio (CVR) and Content Validity Index (CVI) of the questionnaire. As to CVR, a panel of experts assessed the necessity of the items. Accordingly, 20 experts (Ten infectious disease specialists and ten experts in tool design and validation) were consulted and the items with values higher than 0.42 were considered as acceptable based on the Lawshe table. 17 The CVRs of 13 items were found to be higher than 0.42. As to CVI, the 20 experts were asked to rank the items in terms of relevance, clarity, and simplicity; scores higher than 0.79 were considered as acceptable. The results revealed that the CVIs of 13 items were higher than 0.79. 18 The reliability of the instrument was determined using the test-retest method. Accordingly, the questionnaire was completed by 50 individuals who lived in rural areas in Fars Province in the south of Iran in two stages with a two-week interval. The intra-class correlation coefficient ICC) for the 36 items was 0.87, indicating that the questionnaire had appropriate internal consistency. Supplementary file: Questionnaire.
Data analysis
The collected data were analyzed using descriptive statistics, including mean and standard deviation, along with inferential statistics, One-way ANOVA, Multiple linear regression method and Pearson correlation coefficient. To predictive role of demographic characteristics, attitude, and practice in knowledge, multiple linear regression analysis was performed using the simultaneously (Enter) method.The significance level was set at p < 0.05. Before performing multivariate linear regression, the researchers tested the assumptions of normality of data, homogeneity of variance, and independence of residuals. The Shapiro-Wilk test showed that the variables were normally distributed (p > 0.05). Data analysis was performed using SPSS version 26.
Results
Of the 653 individuals who participated in the study, 370 were male and 283 were female. The cohort predominantly consisted of individuals within the 30-44-year-old age range, with a mean of 44.21 years (SD = 7.36). Table 1 reports the other demographic characteristics of the participants. In this study, the rural populations revealed moderate levels of knowledge, attitudes, and practices. The total mean score ± SD of their knowledge was found to be 10.76 ± 2.10 (out of 15). The total mean score ± SD of their attitudes was 13.65 ± 2.90 (out of 20). Finally, the total mean score ± SD of their practices scores was 8.24 ± 1.70 (out of 12). (Table 2). Table 3 displays the findings of the correlational analyses investigating the relationships between demographic variables (age, gender, education level, occupation, marital status) and knowledge, attitudes, and practices. No statistically significant correlations were observed between demographic variables and knowledge, attitudes, and practices.
Individual characteristics of the subjects (n = 653).

The rural population’s mean scores for knowledge, attitudes, and practices regarding the dengue fever (n = 653).
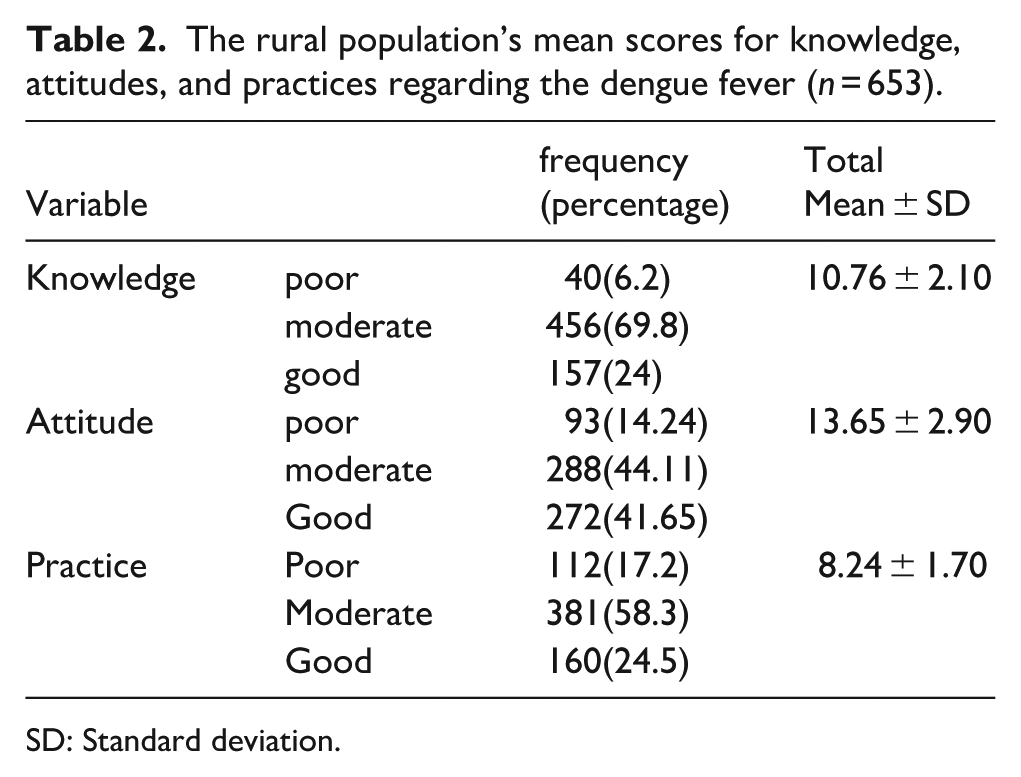
SD: Standard deviation.
Associations between sociodemographic factors, knowledge, attitudes, and practices among rural populations regarding the dengue fever (n=653).
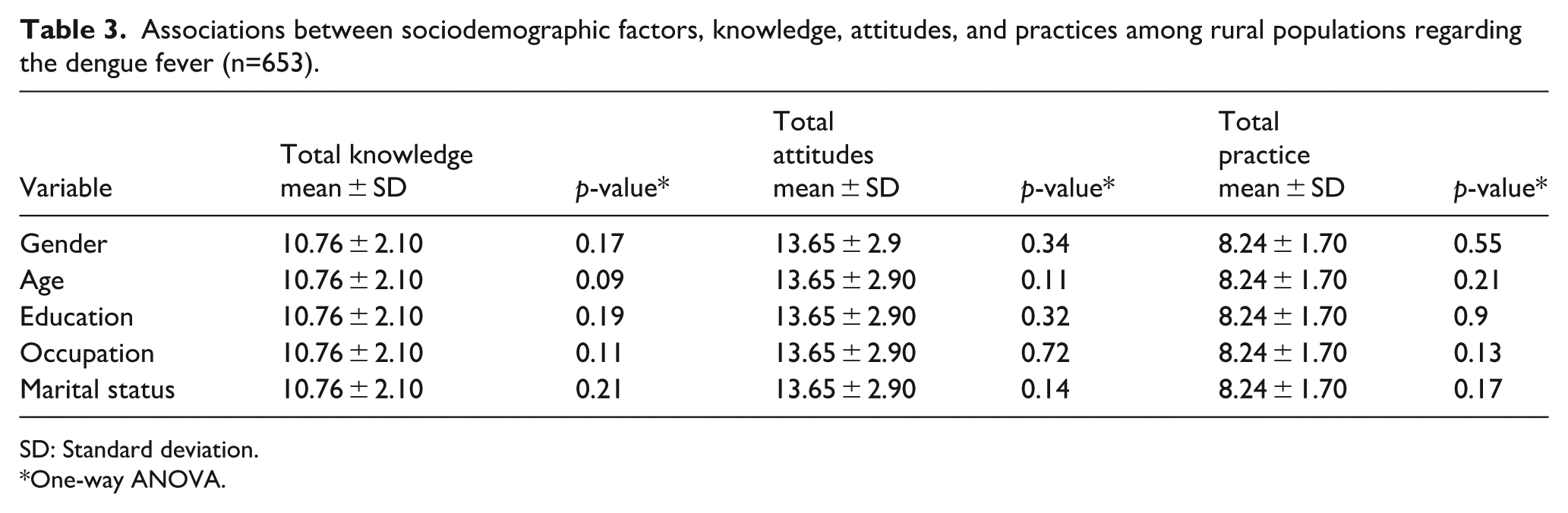
SD: Standard deviation.
One-way ANOVA.
Pearson’s correlation coefficient analysis revealed a direct and statistically significant relationship between knowledge, attitudes, and practices. The findings revealed a substantial positive correlation between the participants’ knowledge and their attitudes (r = 0.47, p < 0.001), as well as a strong direct relationship between knowledge and practices (r = 0.51, p < 0.001). Further, a noteworthy positive correlation was found between attitudinal variables and practical behaviors (r = 0.45, p < 0.001) (Table 4).
The relationship between knowledge, attitude, and practice regarding the dengue fever.
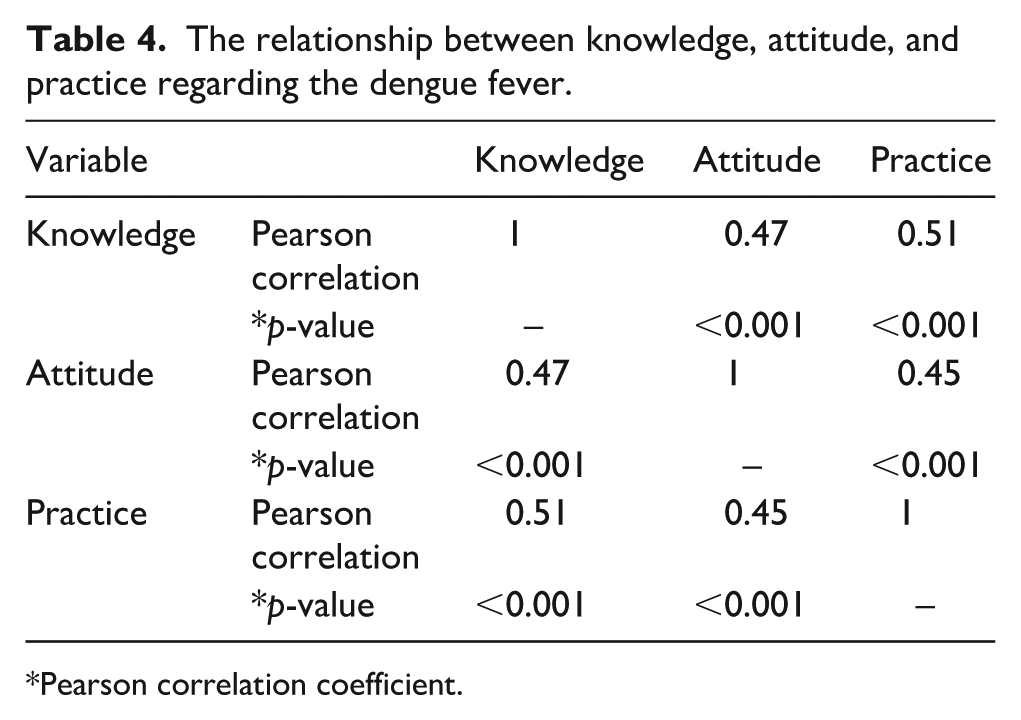
Pearson correlation coefficient.
Table 5 indicates the results of multiple linear regression analysis regarding the predictive role of demographic characteristics, attitude, and practice in knowledge regarding dengue fever among the rural population. The results showed that attitude and practice explained 45% of the variance in knowledge (R2 = 0.45, p < 0.001). In addition, attitude (β = 0.123, p = 0.001), and practice (β = 0.172, p < 0.001) had the highest predictive impact on knowledge (Table 5).
Factors predicting on rural populations knowledge regarding dengue fever.

Multiple linear regression (simultaneous (Enter) method); VIF: Variance inflation factor; B: Unstandardized coefficients; SE: Standard error; ß: Standardized coefficients, Adj R2: 0.45; F: 9.505; Durbin- Watson (DW: 1.75); p ≤ 0.05.
Discussion
The present study aimed to examine knowledge, attitudes, and practices regarding dengue fever among the rural population in Fars Province, Southern Iran. Results indicated that the mean scores for knowledge, attitudes, and practices related to the Aedes mosquito were moderate among the population of 17 villages in Fars Province, Southern Iran. This finding highlights the need for enhanced education and awareness campaigns regarding the Aedes mosquito and dengue fever; thus, the implementation of educational interventions in this domain is strongly recommended.
A study conducted by Al-Yousef et al. (2016), exploring families’ knowledge, attitudes, and practices towards dengue fever in urban Yemeni communities, indicated that most urban residents possessed a clear understanding of dengue fever and manifested positive attitudes towards its severity and potential transmissibility. These findings are not in the same line with the results of the present study. The discrepancy in outcomes may be attributed to the effective implementation of public educational interventions concerning the Aedes mosquito and dengue fever by Yemen’s health authorities as well as mass media. 19 In the present study, the rural population’s knowledge, attitudes, and practices were found to be moderate, suggesting that a segment of this population has received some education regarding the Aedes mosquito and dengue fever. Nevertheless, to improve and elevate their level of knowledge, attitudes, and practices, further educational programs and interventions are required. In this regard, Asadian et al. (2024) concluded that the level of knowledge, attitudes, and self-care behaviors concerning dengue fever was low, recommending the enrichment of public health education programs. 11 In contrast, Chellaiyan et al. (2017) found that the rural population in India had a high level of awareness about dengue fever, which is inconsistent with our findings. Note that Chellaiyan’s study solely examined the level of awareness regarding dengue fever in the rural population, while the present study explored not only knowledge but also attitudes and practices regarding the Aedes mosquito and dengue fever. 20 In comparison to the present study, research in Nepal revealed a low level of public knowledge about dengue fever. 21 Diaz-Quijano et al. (2018), in a study on the correlation between educational level and knowledge, attitudes, and preventive practices associated with dengue fever in Colombia, demonstrated a positive correlation between increased knowledge about dengue fever and changes in attitudes as well as preventive behaviors. 12 Sim et al. (2020), who studied dengue control programs in Singapore, concluded that one of the crucial factors in preventing and controlling dengue fever is the active participation of all local residents in adopting preventive behaviors against Aedes mosquito bites. 22 Further, a study by Suwanbamrung (2021) in Thailand revealed a significant positive correlation between attitudes and practices regarding dengue fever. For strengthening awareness, attitudes, and practices in preventing Aedes mosquitoes, regular health education programs in communities and schools are essential. 23
Given the established presence of the Aedes mosquito in Fars Province in Iran, there is an urgent need for educational programs in this area. 24 Further, some countries have had successful experiences in dealing with dengue fever. For example, in the northern Queensland in Australia, various strategies implemented from 2011 to 2018 have enabled favorable local control of dengue fever. They reported the involvement of the public, including school students, in reducing the transmission routes of this disease. Engaging public participation necessitates raising awareness across the population and encouraging preparedness for the occurrence of dengue fever, as well as understanding its transmission mechanisms. 25
The results of the study by Elson et al. (2020) in Villa El Salvador, Lima, Peru, indicated that the level of awareness, attitude, and performance of the urban populations regarding dengue was high, which is not in accordance with the results of the present study. This difference could be due to the health policies of the Peru country in the field of prevention and control of dengue fever. Also, strengthening educational programs in the field of prevention methods in school‑based health education, developing educational programs in urban areas, and taking effective measures in the field of environmental improvement have been other reasons for the success of this country in controlling this disease. 26
According to the present results, a positive correlation was reported between the attitude, knowledge, and performance of the rural population regarding dengue fever. In this regard, the results of the study by Ghimire and Pangeni (2024) also demonstrated that while the community had good knowledge about dengue and positive attitudes towards prevention, their preventive measures were inconsistent, representing a gap between knowledge and practice. Positive attitudes were associated with better adherence to preventive measures. For addressing this gap, it is crucial to promote positive attitudes towards dengue prevention through initiatives such as strengthening educational campaigns and social mobilization programs. Implementing social and behavior change communication programs with a focus on dengue prevention and control measures can help bridge this knowledge-practice gap 27 . The findings of Hamed’s (2024) research in Saudi Arabia revealed that the average score of knowledge, attitude, and practice regarding dengue was at a high level, which does not align with the results of the present study. The difference in results could be due to the target population, the type of measurement tool, and health policies in the field of preventive measures. 28 The results of Mohamed et al.’s (2025) research in Pakistan demonstrated that the average score of knowledge, attitude, and practice regarding dengue was at a high level among the medical professionals; this is not in the same with the results of the present study. The good knowledge, attitude, and practice about dengue among medical professionals may be because they have easier access to reliable information. Based on the results of this study, promoting public health education programs and health measures in the field of environmental improvement plays a significant role in the prevention and control of dengue fever. 29
Limitations
The present study had a cross-sectional design, making it difficult to conclude the causes of the problem. Further, as the study was carried out in 17 villages in the south of Iran, the findings may not be generalizable to all rural regions in Iran and other countries. Thus, it is suggested that similar studies should be conducted in other regions of Iran and other countries. Another limitation of the study was the use of a self‑report questionnaire, so the participants’ responses may not have been truthful; as such, there may have been social desirability bias or acquiescence bias. This study might be limited by its cross-sectional design since changes in knowledge and the way it can affect practices related to dengue fever cannot be assessed.
Conclusion
Overall, the knowledge, attitudes, and practices of the rural population regarding dengue fever were at a moderate level. Thus, health system policymakers are highly recommended to implement appropriate strategies, including universal public health education coverage, the development of educational packages, and enhancement of educational campaigns. Effective strategies for mitigating and controlling the spread of dengue depend on public knowledge and attitude changes as well as appropriate measures for successful disease control. It seems that health education can play a key role in promoting public awareness, management, and control of dengue. It is also essential to enhance the active participation of the community in implementing dengue control. Workshops, seminars, and digital training modules should be developed to equip healthcare workers with the necessary skills for early detection and effective management of cases, thereby lowering the likelihood of disease outbreaks. In addition, public health campaigns aiming at raising the community’s awareness of mosquito breeding sites should be prioritized.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251376881 – Supplemental material for An investigation of knowledge, attitudes, and practices regarding dengue fever among rural populations: A cross-sectional, multicenter study
Supplemental material, sj-docx-1-phj-10.1177_22799036251376881 for An investigation of knowledge, attitudes, and practices regarding dengue fever among rural populations: A cross-sectional, multicenter study by Zahra Ghazanfari, Mostafa Bijani and Zahra Montaseri in Journal of Public Health Research
Footnotes
Acknowledgements
The authors would like to appreciate Fasa University of Medical Sciences & Clinical Research Development Unit of Fasa Valiasr hospital for financially supporting this research.
Ethical considerations
The present study was conducted in terms of the principles of the revised Declaration of Helsinki, which is a statement of ethical principles that directs physicians and other participants in medical research involving human subjects. The participants were assured about their anonymity and confidentiality of their information. Moreover, the study was approved by the Institutional Research Ethics Committee of Fasa University of Medical Sciences, Fasa, Iran (Ethical code: IR.FUMS.REC.1403.070. Date: 9/10/2024).
Consent to participate
All the participants gave written informed consent to participate in the study.
Author contributions
ZG was involved in the conception and organization of the study. MB, and ZG were involved in the execution and data collection of the study; MB and ZM, participated in statistical analysis design and/or execution. All authors contributed to the preparation, critical review and all of them approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.