
Abstract
Objective:
Measles is a highly contagious disease with significant morbidity and mortality, particularly among children under five. Despite the availability of an effective vaccine, in 2022, 22 million children worldwide missed their first dose and 11 million missed their second. This study aimed to explore the reasons for measles vaccine refusal and delay among mothers of young children in Yerevan, Armenia, using the constructs from the Health Belief Model and the Theory of Planned Behavior.
Methods:
Eight mothers of children aged 13–36 months were recruited through convenience and snowball sampling. In-depth interviews examined their beliefs about measles and vaccination, perceived social norms, and sources of information. A thematic analysis was conducted.
Results:
Although participants generally understood measles’ severity and transmissibility, many believed their children’s natural immunity was sufficient protection. Concerns about vaccine safety and effectiveness were common. Despite reporting no structural barriers and expressing trust in individual healthcare providers, participants exhibited a broader mistrust of health institutions. Social media was a key source of anti-vaccine messaging, while family norms strongly influenced vaccination decisions.
Conclusion:
The study revealed that vaccine hesitancy among participants was primarily driven by a strong belief in natural immunity, mistrust in health institutions, and the influence of misinformation on social media. To improve vaccine uptake in Armenia and similar contexts, it is essential to rebuild public trust in health authorities and actively counter false information, particularly on social media platforms.
Keywords
Introduction
Measles is a highly contagious vaccine-preventable infection associated with considerable morbidity and mortality. 1 The virus spreads through air droplets from contact with the infected person. 2 Those most at risk for severe illness and complications from measles include children under 5, pregnant women, and people with low immune status. 3
Before the introduction of vaccine, measles epidemics caused an estimated 2.6 million fatalities each year. 4 Currently, the measles vaccination is administered as part of the measles-mumps-rubella (MMR) vaccine combination in most countries. 5
According to the Centers for Disease Control and Prevention of the United States (CDC), children should receive measles vaccination’s 1st dose after their first birthday (with effectiveness of 93%) and the second dose between 4 and 6 years of age (with effectiveness of 97%). 3 There are very few contraindications to the vaccine, including severe allergies to the vaccine or its components, or serious immune system issues, which might be caused by chemotherapy, long-term immunosuppressive therapy, or advanced HIV. 3
Despite the availability of MMR vaccine, 22 million children had not received their first dose of measles vaccine and 11 million had not received their second dose in 2022, globally. 6 Between 2021 and 2022, the global incidence of measles increased by 18%, with a 43% increase in mortality. 7 Around 136 000 estimated measles deaths occurred worldwide in 2022. 4
The WHO defines vaccine hesitancy as a “delay in acceptance or the refusal of vaccination despite their availability.” 8 While being hesitant may cause parents to postpone or skip their children’s recommended vaccinations, it is important that providers offer timely support and guidance to help them choose vaccination for their children. 9 Children who miss timely vaccinations face the danger of never completing the required immunization schedule. 10 Vaccination timeliness is increasingly acknowledged as vital for effective child protection, drawing attention in various countries. 11
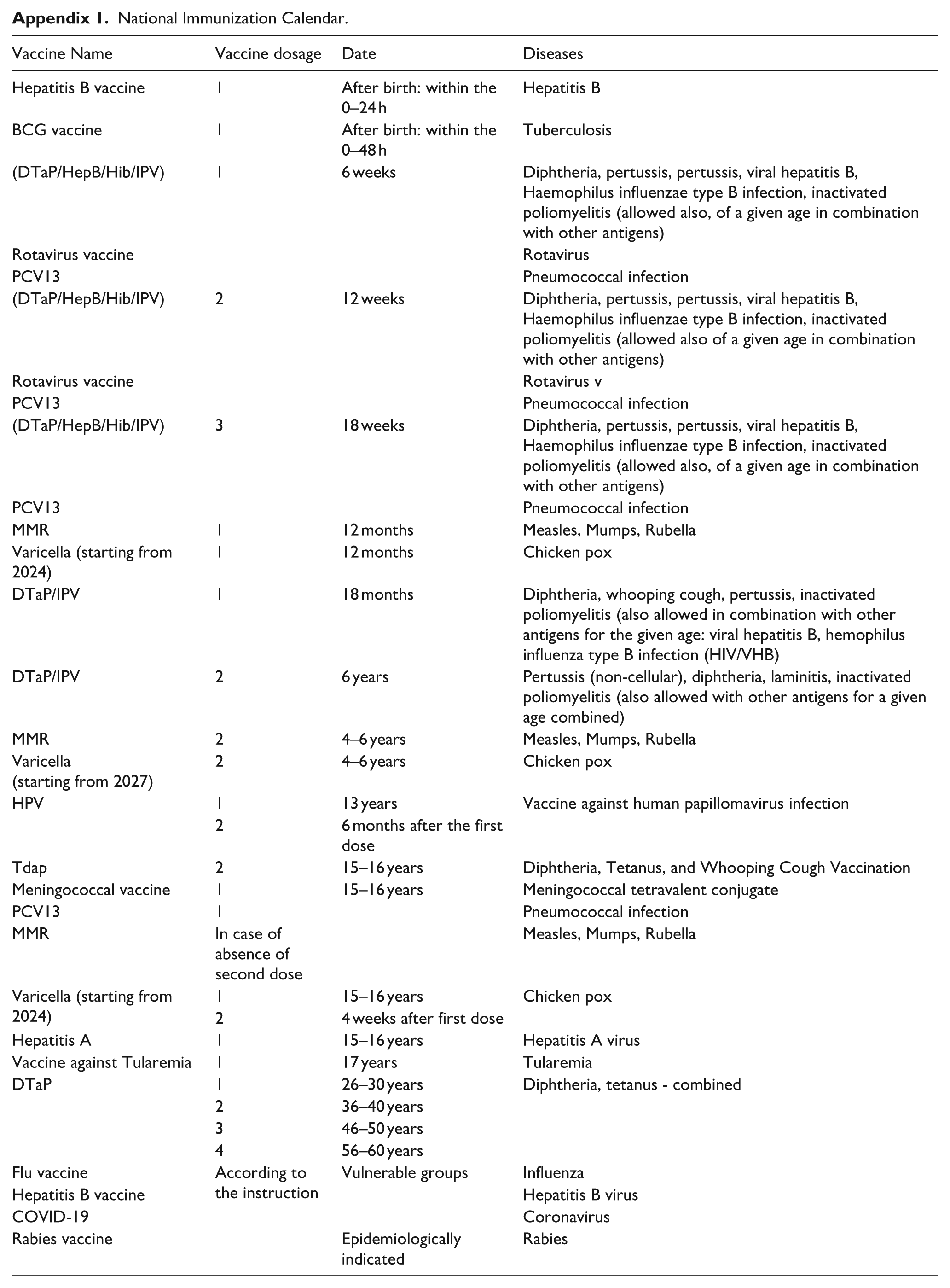
The government of Armenia has implemented a comprehensive national immunization program that includes the administration of the MMR vaccine with the first dose of the vaccine given at 12 months and the second dose between 4–6 years of age. (Appendix 1). 12
Armenia’s measles vaccination rates have ranged from 92-94% coverage in both 2020 and 2021, 13 The government’s continued commitment, in close collaboration with international partners such as the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF), has significantly mitigated the burden of measles in the country. Since 1994, UNICEF has supported Armenia in procuring vaccines for six WHO-designated vaccine-preventable diseases, including tuberculosis, diphtheria, tetanus, pertussis, polio, and measles. This support has extended beyond vaccine supply to include syringes, safety boxes, and cold-chain equipment. Over time, UNICEF also introduced immunization effort through training for healthcare providers, public health education and communication initiatives. 14
Despite these efforts, according to the 2015/2016 Armenia Demographic and Health Survey(ADHS) data only 79.6% of 12-35 months old children in the study sample received the first dose of the measles vaccine, while many children had delayed or unknown immunization status. 15 Another study reported that the median age of the MMR vaccine delay was 61.1 weeks in Armenia. 16
A study conducted in 2015 in Armenia and Kyrgyzstan using the DHS datasets of 1997 to 2012 analyzed measles-containing vaccine (MCV) vaccination timing and coverage among children aged 18-59 months. Analysis of the data of child health cards showed that the vaccination delays in Armenia among the 4,629 children were more common in urban areas than rural ones. Furthermore, investigations showed that children of younger mothers had a higher chance of receiving MCV immunizations on time. 17
On March 2, 2023, the Armenian Ministry of Health (MOH) announced the emergence of a measles outbreak in the country. By the end of 2023, a total of 545 confirmed measles cases were reported, with 71.9% of them occurring in children and one death case. 18 According to data from the National Center for Disease Control and Prevention, the number of measles cases in Armenia continued to rise in 2024. As of December 2024, a total of 561 cases had been detected, including 336 (60%) among children. 19 As the evidence shows that the reoccurrence of outbreaks of infectious diseases in high immunization coverage countries is positively correlated with delayed and refused vaccination, 17 investigations are needed to understand the reasons for vaccine hesitancy in Armenia.
Theoretical frameworks, such as the Health Belief Model (HBM) and the Theory of Planned Behavior (TPB), have been utilized to analyze vaccine hesitancy and to inform interventions aimed at increasing vaccination acceptance.20,21 The HBM focuses on the perceived threat of a health condition as well as the perceived advantages and obstacles to adopting a certain health behavior, while the TPB stresses the effect of perceived social norms and perceived behavioral control in addition to individual attitudes. 22
This study explored the reasons for delay and refusal of measles vaccination among mothers of 13- to 36-month-old children in Armenia focusing on the HBM and TPB constructs.
The pursued research questions were:
1) What are the mothers’ beliefs about measles and measles vaccination and how do they impact their decision-making?
2) What social norms and peer influences affect mothers’ decisions to delay or refuse measles vaccination?
3) What are the healthcare-level barriers to measles vaccination?
Materials and methods
Study design
This qualitative study used phenomenological approach to explore mothers’ perceptions regarding measles vaccination, providing in-depth insights into their lived experiences and main influences on their decision-making. 23
Study population and setting
The study was conducted in the capital Yerevan, where vaccination delays were found to be more common. 24 The sample inclusion criteria were the mothers of children aged 13–36 months residing in Yerevan who had not received the first dose of the measles vaccine. The lower age limit was set based on the definition of a vaccination delay as failure to vaccinate the child within 30 days after the recommended age of 12 months. 25 The sample was limited to children under 3 years of age to minimize the recall bias. Exclusion criteria included mothers who self-reported medical contraindications to vaccination in their children, such as allergies or immunodeficiency disorders. These conditions are considered contraindications according to both CDC guidelines and Armenian primary health care protocols. 3 As a result, five mothers were excluded from the study due to these reported medical restrictions.
Study Instrument
In-depth interviews conducted individually with each participant allowed for a more detailed account of beliefs and experiences and provided ample opportunities for exploring issues thoroughly. 26 A semi-structured interview guide with open-ended questions, probes and prompts was developed based on the HBM and TBP constructs, commonly used to study parental hesitancy of childhood immunizations. 27 The instrument included domains of perceived susceptibility, perceived severity, perceived benefits and barriers, perceived self-efficacy, cues to action and subjective norms. A screening form determined participants’ eligibility based on child’s age and vaccination status. A brief questionnaire collected demographic information.
Data collection and analysis
Convenience and snowball sampling methods were used to assemble the study sample. Data collection was conducted from March 4 to April 8, 2024. Participants were first contacted by phone to determine their willingness to participate. Interviews were conducted by the first author who received graduate level training in qualitative research methods. Data were collected through both in-person and Zoom interviews, all conducted in private settings with only the participant and the interviewer present. Interviews were recorded, and notes were taken with participants’ permission. Saturation was reached after eight interviews. Interviews were transcribed verbatim in Armenian, and the data was coded manually by the interviewer. HBM and TPB frameworks guided data coding. Thematic analysis approach was used.
Ethics statement
The study received approval from the Institutional Review Board (IRB) of the American University of Armenia (AUA) under protocol number AUA-2024-001. Before the interviews, verbal consent form detailing the study’s purpose, contact information, confidentiality assurances, and voluntary nature of participation was administered. The written consent was waved by the IRB; instead, verbal consent was obtained from each participant and audio recorded as part of the data collection process.
Results
Participants had a mean age of 32.8 years (range: 29–37 years). All of them were married, had university education, and more than one child. The mean age of their youngest child was 27.2 months (range: 14–36 months). The mean duration of the completed interviews was 35.8 min, ranging from 29 to 47 min (Table 1).
Demographic characteristics.

Maternal knowledge of the measles symptoms, course, and treatment
Participants demonstrated some awareness of disease symptoms and course. Five out of eight participants listed common symptoms, like fever, rash, and respiratory problems, and knew that catching measles can result in the development of natural immunity against disease. Many also knew that measles is a viral infection. Respondents who had personal or family experience with measles showed better understanding.
“As far as I know, it is a viral infection, and children have high fever, rash …it usually requires hospitalization. It can cause pneumonia.”(P4) “It’s a viral infection that, once you get it, you get immunity for life. The rash occurs on child’s body, the temperature is rising, but it has “expiration days”, then it goes away…. I had measles when I was young, and I was not vaccinated. I had high temperature; my sister had a more serious case… but we both have lifelong immunity.”(P5) “…. fever, rash, and I don’t know, as far as I know, the disease spreads to the lungs, or I can’t say otherwise, but chickenpox spreads to the lungs.”(P2)
Perceived susceptibility
Most of the participants believed their children were susceptible to the virus, especially in shared environments like kindergartens or public playrooms. They saw interaction with infected people as the main risk factor. Even though mothers realized the inevitability of illness transmission among children, they stressed the importance of strong immune system in reducing infection risk.
“…if my child goes to the kindergarten, it is possible for him to get various diseases…. as soon as one gets infected, it spreads among children in the kindergarten (laughs). Anyway, if the immunity is not too low, the child will not get it…”(P2) “Well…..it is possible. Like all viruses…But if you have good immunity, the risk of getting infected is lower.”(P6)
Perceived severity
The perceptions of the severity of measles were similar across the respondents. They shared similar views on measles severity, mentioning consequences like pneumonia, hospitalization, and medical management of the disease. Most mothers knew that measles imposes a serious risk for health, especially for children with compromised immune systems and underlying health conditions. However, they were confident in their children’s robust immunity citing the absence of chronic diseases and frequent infections. Consequently, many mothers assumed that if their children contracted measles, it would likely be mild and not pose significant health challenges.
“……. if the child doesn’t have a strong immune system, it will be severe, just like the flu or chickenpox or the coronavirus can be serious in case of having low immunity.”(P1) “I think it’s severe, if you don’t watch the progress of disease properly or if the child doesn’t have a strong immune system, it can be serious.”(P2) “…. it depends on whether there is an accompanying illnesses that can weaken the immunity … if there are none, I am sure that he should take it more lightly…..”(P3)
Perceived benefits of vaccination
The participants expressed disbelief in the effectiveness of all vaccines, including vaccine against measles. Several respondents compared measles vaccination to COVID-19 immunization, reporting increased occurrences and severe disease in their families following immunization. Participants who had been vaccinated but still contracted COVID-19, doubted vaccines’ effectiveness. Some respondents viewed vaccines as providing only temporary immunity that diminishes over time, questioning their long-term effectiveness.
“If my child is going to get infected, the vaccine won’t protect him 100%…..therefore this vaccine has no advantage for me.”(P3) “We were vaccinated against Covid, but we got infected two or three times and it was not mild, even much more severe.”(P5)
Along with stressing the vaccine’s ineffectiveness, mothers expressed a belief in the superiority of natural immunity, favoring natural exposure over vaccination. They emphasized the body’s innate ability to fight off virus and were sceptic about artificial immunity induced by vaccinations. Mothers stressed that their children should be allowed to experience illness to develop life-long immunity, and that it is a better path to health“Since he may get the virus, let him get infected and get immunity naturally.”(P6) “There is no need to infect your child unnaturally and…then treat it. It is better to get sick naturally at once.”(P8) “No one is insured against getting a disease, let him get sick and acquire natural immunity. Thanks God, hospitals and treatments are available today. He will have natural immunity for life.”(P7)
Perceived barriers
Most of the respondents had a concern that vaccination threatens immunity. They reported increased frequency of illnesses following vaccinations, which they interpreted as an evidence of a compromised immune system.
“I did not want to suppress the natural immunity of my child by vaccination…”(P1) “In terms of illnesses, my children don’t get sick very often. I know someone, whose son is vaccinated and sick twelve months a year. And when he gets sick, we tell “look, they vaccinated him, but he gets sick very often.”(P2) “In general, I think that it does not contribute to strengthening the immunity, but the opposite.”(P3)
Other perceived obstacles to vaccination centered on concerns about side effects and vaccine safety, contributing to vaccine hesitancy. Participants mentioned stories they have heard and personal experiences as reasons for their skepticism. Some reported witnessing adverse effects in children who had been vaccinated against viruses such as Rotavirus and Polio, impacting their decision not to vaccinate their children against measles. No other barriers related to healthcare providers, financial, time limitations, or other logistical obstacles to vaccination were mentioned by the participants.
“I have heard that they vaccinated (the child) and the child died, a six-month-old child… they said that the death was from getting the vaccine. And after hearing such things, I thought that it is better not to vaccinate..”(P2) “One of my extended family members, who is in France, had her child vaccinated with MMR vaccine, after which her son became deaf…”(P3) “I didn’t vaccinate the child against polio because I knew cases when it affected the child’s brain, and I knew many cases when after polio vaccine children had defective development, Autism.”(P5)
Sources of information about vaccination
Many participants told they obtained information on vaccination from healthcare professionals during their visits. According to them, pediatricians and nurses emphasized the importance of vaccinations for children’s health. Pro-vaccination posters in polyclinics also served as reminders and cues, but most mothers noted that none of these influenced their decisions.
“Of course, she presented papers about vaccinations and gave them to me. She also told that it is essential and tried to explain why we should vaccinate our child, etc., but if the person does not want it, as in my case, it is difficult to convince me.”(P1) “They say you should vaccinate, you’re making a mistake not to vaccinate, your child may have complications, etc., but I still say - I don’t agree with their opinion and I made a right decision not to vaccinate.”(P5) “They told us, informed us…and when the time comes, the nurse calls and informs that it is time for vaccination.”(P6)
Most of the study participants were satisfied with care provided by their pediatricians in the primary health care centers, describing generally positive and supportive relationships with them and citing qualities such as compassion, responsiveness, and empathy.
“Our pediatrician is always very pleasant, kind-hearted, they are ready to accept us at any time at every visit they ask if I have no regrets regarding my vaccination choice, and I say no. If something changes for me, I will contact you.”(P3)
Participants reported many other sources of information related to vaccination, including social media platforms such as Facebook groups, YouTube videos, and blogs written by unknown individuals. According to the mothers’ reports, these platforms mostly have anti-vaccination content, which they seemed to trust and base their decisions on. Furthermore, several mothers reported significant trust in Soviet medical literature and professionals, suggesting that their healthcare beliefs of natural immunity were shaped by those senior professionals in the field. Notably, the participants did not trust the WHO and held certain conspiracy beliefs.
“Let me tell you something, there is a Facebook group called “Smart Mom” …that group gives a lot of information about vaccines and there are specific links to websites, American/European websites where everything is mentioned. Even the instructions from the vaccine boxes are translated into Armenian and posted there. For example, once read that there is a certain amount of mercury in vaccines which is toxic for the body. Parents also share issues they had with their vaccinated children with many examples. After seeing all that information, I decided not to vaccinate.”(P3) “Usually, I Google search and the Facebook groups where mothers share their comments on vaccine experiences. I do not trust and follow WHO recommendations because they have a plan to reduce the size of population, kill children. They do huge business on vaccinations.”(P5) “I absolutely do not trust the website of the WHO, absolutely. I have done some research, read different comments and reports about side effects of vaccines in Google and Facebook; also I am looking for some information from Soviet books as well.”(P6) “I’ve watched YouTube videos of well-known pediatricians, mostly Russian…they say that most of the diseases have already faded, are worn out, and there is no need to establish immunity in unnatural, synthetic way.”(P8)
Social norms
The participants highlighted the essential role of immediate family members in their vaccination-related decisions. They highlighted support and agreement with their decision not to vaccinate among spouses, parents, and in-laws. The parents of five out of eight participants had chosen not to vaccinate their children, and not being vaccinated themselves had a significant influence on the participants’ decision-making processes, inspiring and confirming their own decision to refuse immunization for their children. Aside from the family influence, most mothers stated that they do not consider external viewpoints and are opposed to outside interference from friends or other networks in their vaccination decisions.
“My husband and his parents share the same opinion about vaccinations.”(P1) “My parents accept, my mother accepts that I don’t vaccinate (the child) …, I am not vaccinated myself and I never get sick frequently.”(P2) “My parents share my opinion, that I am doing the right thing by not vaccinating. They are also concerned about side effects of the vaccines, like Autism.”(P5)
However, most interviewees said they felt pressured to vaccinate their children by pediatricians, friends, and extended family members. This external pressure complicated their decision-making process, sometimes resulting in conflict or discomfort.
“…for example, my relative always says “Oh, how could you not vaccinate the child, you are crazy, that’s not right”…And we say that we are the child’s parents and we have decided that the child will not be vaccinated…..”(P2) “One time, our pediatrician spoke in an unpleasant manner, saying that if I do not vaccinate my child, she will die. She repeated it three times. I was in a bad psychological state; I had just given birth to my child, and I didn’t expect so much pressure, so I struggled a lot when I got home. But with the support of my family, I overcame. No one has the right to force me to vaccinate my child. The only decision is mine.”(P4) “On one occasion my friend accused me …that because of me the incidence of this disease is growing(laughing) …because I don’t vaccinate my child.”(P6)
Discussion
Guided by the HBM and TPB frameworks, this study explored beliefs related to measles and measles vaccination among vaccine-hesitant mothers of 13-36-month-old children in Yerevan, Armenia.
Our study showed that most mothers were familiar with measles signs, symptoms, and progression. This supports earlier findings in Southeast Europe which demonstrated that mothers often have a thorough awareness of vaccine-preventable diseases like measles. 28 However, it has been shown that knowledge alone has no substantial impact on adopting protective behaviours,while beliefs are strongly associated with the practice of preventive actions. 29
While most mothers thought that the possibility of getting measles was rather high, they also believed that since their children were overall healthy and had no accompanying illnesses, their immune systems were robust enough to protect them against the infection. Their beliefs in “inherent immunity” substantially influenced their perceptions of the necessity of vaccination. This notable finding is in line with other studies which have shown that many parents’ risk perceptions related to childhood infections are based on the personalized assessments of their child’s health and susceptibility rather than evidence-based epidemiologic perspectives. 30
There appears to be a notable difference between Armenian mothers’ assessments of the severity of measles and those of parents of unvaccinated children reported in previous studies28,31 with Armenian mothers seemingly having a better understanding of the disease severity. For example, in our study, many mothers cited serious consequences for health in case of a severe course of disease and acknowledged the need for hospitalization and isolation for children diagnosed with the disease, which, according to them, was also associated with substantial psychological and logistical burden. However, like the susceptibility beliefs, these perceptions did not translate into decision to vaccinate their children, presumably because of their conflicting beliefs about the importance of general health status and the notion of immunological resilience as a mechanism of protection from the severe consequences of the disease.
According to the HBM, perceptions of threat are important for considering a protective behavior, but the specific action taken is greatly determined by beliefs regarding the available behavioral options to reduce the threat, and the adoption of a particular behavior occurs when its perceived benefits outweigh its perceived barriers. 32 This is supported by our findings, which reveal a lack of confidence in the MMR vaccine with most believing that vaccines cannot completely protect their children and are largely ineffective. Similar findings were observed in other studies, where mothers generally lacked belief in the effectiveness of childhood immunizations.33,34 It is also noteworthy that among some of the participants, their misperceptions and assumptions regarding the effectiveness of the COVID-19 vaccines impacted their beliefs related to measles vaccination. This raises concerns about the possible impact of misinformation during the COVID-19 pandemic on participants’ beliefs in the benefits of vaccinations in general, and their intentions to vaccinate their children. A significant decline in in the acceptance of children immunizations during the COVID-19 pandemic has been reported in several recent studies; 35,36 in certain countries, this decrease has reached 44 percentage points. 37
The beliefs about the ineffectiveness of the vaccines were, at least in some part, influenced by the mothers’ perceptions about the superiority of natural immunity over vaccinations. These perceptions were quite deep-seated and referred to not only vaccination against measles, but also vaccinations in general. Some of the mothers stressed that they would prefer that their children get infected with measles and build “natural immunity for life”. Several authors have claimed that some vaccine-hesitant individuals have a set of beliefs about health which include preference for natural immunity or think that the immune system is an individual characteristic and needs a tailored approach.9,30,38 Also, in line with other studies, our study participants hold the belief that vaccines weaken the immune system, despite scientific evidence indicating otherwise. 39
Interestingly, while in this particular study the participants’ perceptions of the robust immunity status of their children and fears of compromising this immunity with vaccination seemed to lead to vaccine hesitancy, in other studies, underlying health conditions and fragile health status of children generated parental concerns about their ability to tolerate the shots and their vulnerability to unfavorable vaccination outcomes.40,41 These findings highlight that there is a variety of widespread misconceptions among parents regarding vaccinations and their impact on child’s health, ultimately circling back to the notion that vaccination weakens immunity. Our results together with other observations in the literature, emphasize the necessity of focused and context-appropriate initiatives to dispel myths and promote well-informed vaccination decisions.
The reports from mothers in this study highlighted a deep confusion about vaccination safety, generated by anecdotal evidence and personal encounters with what they perceived as negative consequences. These findings align with those revealed in other studies, where similar negative outcomes were described by parents, including the links between MMR vaccination and disorders like autism and other developmental delays in children.9,31,42
While vaccine safety concerns influenced parental decision-making, practical challenges like cost or accessibility did not appear to restrict vaccination uptake in our sample. This contrasts with studies in other countries where parents experience logistical difficulties when vaccinating their children.43,44 Additionally, Armenian mothers have not perceived any healthcare services-related barriers to their children’s immunization. All participants were happy with the primary healthcare services for their children, positively evaluating their quality. Good patient-doctor relationships were cited by almost all participants, and apparently, these relationships have not served as an obstacle to vaccination. Mothers also expressed satisfaction with the amount and quality of information they received from healthcare providers who utilized diverse strategies to educate and encourage vaccination among parents. This finding contrasts international literature, where multiple evidence has been published on poor relationship between vaccine-hesitant mothers and healthcare providers or insufficient information provided by pediatricians.42,45,46
Interestingly, in some instances mothers experienced repeated appeals to vaccinate their children by the healthcare providers. Other authors have also described pressure from healthcare providers regarding parents’ vaccination decisions. 45 However, our analysis suggests that despite having a good relationship with healthcare practitioners and their attempts to promote vaccination, mothers resisted vaccinations. This demonstrates the challenges pediatricians face in vaccine-related communication with mothers and the persistence of vaccination hesitancy which may be largely impacted by strongly held beliefs and attitudes.
This study provided an insight into alternative sources used to obtain information about vaccination besides interactions with pediatricians. Social media platforms with anti-vaccine ads and testimonies discouraging vaccination were the main source for interviewed mothers. This finding is in line with existing literature, which confirms that information gained from these sources frequently reinforces anti-vaccine beliefs.47,48 Notably, mothers in our study expressed distrust of credible health organizations such as WHO, believing that their primary objective is to encourage vaccination and conceal any negative aspects of it. Similar views were reported in other studies where mothers thought that there is a pro-vaccine bias in the “officially endorsed information”. 49 The erosion of trust becomes an important factor in today’s vaccination-related decision-making30,47 and should be further explored in vaccine hesitancy research.
Our study confirms the significance of social norms in shaping mothers’ vaccination decision mostly conveyed by spouses, in-laws, and parents. For example, for most of the mothers having a vaccine-hesitant family created an expectation to not vaccinate their child, which mirrors findings from other studies reported in the literature.49,50 Conversely, friends or acquaintances did not seem to have an influence on vaccination-related decisions among our study participants, while several authors claimed that parental decisions to refuse their children’s vaccinations are heavily impacted by their peers. An article from 2021 investigating parents’ attitudes towards childhood vaccinations found that social influence or depending on peers when making vaccination decisions is related to mothers’ educational level; parents who have university degrees typically have lower levels of trust in networks than parents who do not. 51 Additionally, the study discovered that parents of an only child had a higher level of peer trust than parents of several children. children. Indeed, results were similar to our study participants who had university degrees and more than one child and were less influenced by peer-pressure.
Study limitations
This study has several limitations. First, the study was carried out exclusively in the capital city, which limited the diversity of backgrounds and experiences in our sample. Also, socioeconomic and educational levels were uniformly high, which may have further restricted the transferability of the results to other populations. Moreover, although saturation was reached on the most important themes relevant to the study’s objectives, a relatively small sample size of eight participants might have precluded the investigation of auxiliary topics and questions at sufficient depth. At the same time, the existing literature suggests that thematic saturation can be achieved with a smaller number of participants in focused qualitative studies. 52 We think that this study still provides valuable insights into prevailing attitudes and behaviors related to a critical issue of vaccine hesitancy in an urban educated population and may reflect broader trends or challenges in similar contexts.
Conclusion
The study found that despite the mothers’ relatively adequate knowledge of the measles transmissibility and severity, many of them believed that their children’s robust natural immunity may protect them from the measles infection and mitigate the consequences if infected. Participants expressed doubts about the effectiveness and safety of the measles vaccine as well as other routine childhood immunizations. Despite having no structural or financial barriers to accessing healthcare and reporting full trust in their individual healthcare providers, they continued to refuse vaccination. This contradiction appears to stem from broader mistrust in local and international public health institutions Social media played a significant role in shaping their views serving as a key source of misinformation and anti-vaccine narratives. Additionally, family norms and intergenerational beliefs had a stronger impact on vaccination decisions than peer or community opinions. These findings highlight the complex interplay between personal beliefs, social influence, and institutional trust in shaping vaccine decision-making. .
Implications for research and practice
Quantitative studies should further investigate the links between vaccine hesitancy and the HBM and TPB constructs, as well as explore the influence of socio-demographic factors on mothers’ decision-making in various socio-cultural contexts. Helping mothers distinguish between false and accurate information about vaccination is crucial, particularly on social media. Sharing stories of people affected by measles because of overreliance on natural immunity could be particularly useful for conveying the importance of vaccination. Additionally, initiatives to boost mothers’ confidence in health institutions like WHO and MOH are essential.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251376852 – Supplemental material for Measles vaccine hesitancy among mothers in Yerevan, Armenia: A qualitative study
Supplemental material, sj-docx-1-phj-10.1177_22799036251376852 for Measles vaccine hesitancy among mothers in Yerevan, Armenia: A qualitative study by Tamara Sedrakyan, Zhanna Sargsyan and Tsovinar Harutyunyan in Journal of Public Health Research
Footnotes
Appendix
National Immunization Calendar.
| Vaccine Name | Vaccine dosage | Date | Diseases |
|---|---|---|---|
| Hepatitis B vaccine | 1 | After birth: within the 0–24 h | Hepatitis B |
| BCG vaccine | 1 | After birth: within the 0–48 h | Tuberculosis |
| (DTaP/HepB/Hib/IPV) | 1 | 6 weeks | Diphtheria, pertussis, pertussis, viral hepatitis B, Haemophilus influenzae type B infection, inactivated poliomyelitis (allowed also, of a given age in combination with other antigens) |
| Rotavirus vaccine | Rotavirus | ||
| PCV13 | Pneumococcal infection | ||
| (DTaP/HepB/Hib/IPV) | 2 | 12 weeks | Diphtheria, pertussis, pertussis, viral hepatitis B, Haemophilus influenzae type B infection, inactivated poliomyelitis (allowed also of a given age in combination with other antigens) |
| Rotavirus vaccine | Rotavirus v | ||
| PCV13 | Pneumococcal infection | ||
| (DTaP/HepB/Hib/IPV) | 3 | 18 weeks | Diphtheria, pertussis, pertussis, viral hepatitis B, Haemophilus influenzae type B infection, inactivated poliomyelitis (allowed also, of a given age in combination with other antigens) |
| PCV13 | Pneumococcal infection | ||
| MMR | 1 | 12 months | Measles, Mumps, Rubella |
| Varicella (starting from 2024) | 1 | 12 months | Chicken pox |
| DTaP/IPV | 1 | 18 months | Diphtheria, whooping cough, pertussis, inactivated poliomyelitis (also allowed in combination with other antigens for the given age: viral hepatitis B, hemophilus influenza type B infection (HIV/VHB) |
| DTaP/IPV | 2 | 6 years | Pertussis (non-cellular), diphtheria, laminitis, inactivated poliomyelitis (also allowed with other antigens for a given age combined) |
| MMR | 2 | 4–6 years | Measles, Mumps, Rubella |
| Varicella (starting from 2027) |
2 | 4–6 years | Chicken pox |
| HPV | 1 | 13 years | Vaccine against human papillomavirus infection |
| 2 | 6 months after the first dose | ||
| Tdap | 2 | 15–16 years | Diphtheria, Tetanus, and Whooping Cough Vaccination |
| Meningococcal vaccine | 1 | 15–16 years | Meningococcal tetravalent conjugate |
| PCV13 | 1 | Pneumococcal infection | |
| MMR | In case of absence of second dose | Measles, Mumps, Rubella | |
| Varicella (starting from 2024) | 1 | 15–16 years | Chicken pox |
| 2 | 4 weeks after first dose | ||
| Hepatitis A | 1 | 15–16 years | Hepatitis A virus |
| Vaccine against Tularemia | 1 | 17 years | Tularemia |
| DTaP | 1 | 26–30 years | Diphtheria, tetanus - combined |
| 2 | 36–40 years | ||
| 3 | 46–50 years | ||
| 4 | 56–60 years | ||
| Flu vaccine | According to the instruction | Vulnerable groups | Influenza |
| Hepatitis B vaccine | Hepatitis B virus | ||
| COVID-19 | Coronavirus | ||
| Rabies vaccine | Epidemiologically indicated | Rabies |
Acknowledgements
Authors thank to all the participants in this study for their contributions to advancing knowledge in this field.
Consent to participate
All participants provided verbal informed consent prior to participation. The requirement for written consent was waived and study was approved by the Institutional Review Board (IRB) of the American University of Armenia (AUA) under protocol number AUA-2024-001.
Author contributions
All authors contributed to the idea, research design, implementation, data collection, data analysis, interpretation, and revision of the article, with the final manuscript reviewed and approved by all.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data sets are available from the corresponding author on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.