
Abstract
Background:
Unintended pregnancy is a public health problem that can lead to negative health outcomes for both the mother and children, and its prevalence remains a major health problem in Ethiopia. Globally, an estimated 44% of pregnancies and 23% of births are unintended, and the problem is especially high in sub-Saharan Africa, including in Ethiopia.
Design and methods:
A community-based cross-sectional study was conducted on 508 study participants from July 1, 2020, to August 31, 2020. The required sample size was allocated proportionally to the randomly selected subdistricts, and simple random sampling technique was used to select participants. A validated London Measure of Unplanned Pregnancy (LMUP) is used to assess unintended pregnancy. Data were collected through face-to-face interviews and finally analyzed using SPSS 21. Bivariate and multivariate analyses were employed to assess factors associated with unintended pregnancy. Finally, a p value of <0.05 was used as a cutoff point for statistical significance.
Results:
The prevalence of unintended pregnancy was 34.1%. Out of which, 78.6% were mistimed and 21.4% were unwanted during pregnancy. This study revealed that the rural residence (AOR = 2.95), multi parity (AOR = 3.03, 95%), age at first pregnancy, <20 years (AOR = 4.4), history of abortion (AOR = 5.4), lack of contraception awareness (AOR = 2.45) and no discussion about family planning with husband (AOR = 2.63) were significantly associated with unintended pregnancy.
Conclusions:
The prevalence of unintended pregnancies was high, the majority of which were mistimed.Proper postpartum family planning counseling is required to reduce unintended pregnancy.
Introduction
Unintended pregnancy is defined as a pregnancy that is either unwanted or untimely because no children or fewer children were desired or occurred earlier than desired. 1 Globally, an estimated 44% of pregnancies and 23% of births are unintended. In Africa, about 39% of all pregnancies and 27% of births are unintended. 2 Unintended pregnancy is 36% higher in developing countries compared to developed countries. 3 The global maternal mortality rate is 211 per 100,000 live births, with Sub-Saharan Africa and Southern Asia accounting for approximately 86% of global maternal deaths, with Sub-Saharan African countries accounting for 66% (196,000) of all maternal deaths in 2017. Moreover, in Ethiopia, the maternal mortality rate was 401 per 100,000 live births. 4
Unmet family planning needs contribute to a high rate of unintended pregnancy and poor reproductive health outcomes, including a risk of maternal morbidity and mortality. 5 More than 65.0% of women with unintended pregnancy in 36 low- and middle-income countries were either non-users or using traditional family planning methods. 6 The types of contraceptive method used, failure of the chosen method with couples, not using contraceptive methods, lower income, and husband refusal are the major contributing factors for unintended pregnancy. 7
Despite improvements in contraception use and a decline in Ethiopia’s total fertility rate to 4.6 children per woman in 2016, the wanted fertility rate is 3.6 children, indicating that women in Ethiopia are burdened with having one child more than they want, and approximately 25% of pregnancy was reported as unintended. 8 In Ethiopia, 24.7 and 42% of unintended pregnancies were caused by contraceptive failure and not using contraceptive methods, respectively. 9 In 2016, the unmet need for family planning in the Oromia region was the highest of all regions in Ethiopia (28.9%), 17.1% was mistimed, and 18.8% was unwanted.
Preventing unintended pregnancies is closely linked to lowering maternal mortality. 1 Moreover, preventing unintended pregnancy through effective family planning could avert about 30% of maternal deaths. 10 Moreover, in Ethiopia, implementing effective family planning interventions could avert an estimated nearly 15 million unintended pregnancies and more than 30,000 maternal deaths between 2015 and 2020. 11 However, the modern family planning utilization rate was very low (35%) in Ethiopia. 8 To alleviate the problem, the Ethiopian government has prepared a national reproductive health strategy that focuses on reducing unintended pregnancy by increasing access, creating demand, and improving the utilization of quality family planning services, with performance targets of increasing contraceptive prevalence rates to 55%, reducing total fertility rates to 3, and reducing the unmet need for modern contraceptive methods to 10% by 2020. 12 The issue of unintended pregnancies has received minimal attention from Ethiopian researchers priorly during this research, despite recent metanalysis by different researcher and little has been said about its associated factors, especially in rural semi pastoralist areas. Furthermore, efforts to reduce the number of unplanned pregnancies were quite flimsy. Even though some studies have been done on the prevalence and associated factors of unintended pregnancy in Ethiopia and study area, but there is no community-based study conducted at the study area with semi pastoralist to make representative for country wide yet. Therefore, this study was aimed at determining the proportion and the factors associated with unintended pregnancy among pregnant mothers at Mi’eso district, West Hararghe, Oromia region, Ethiopia.
Materials and methods
Study area and period
The study was conducted in Mi’eso district, which is found in West Hararghe Zone, Oromia Regional State, Eastern Ethiopia. The district is located 300 km from Addis Ababa, Ethiopia’s capital city, and 25 km from Chiro Town, the zonal town. The district has one hospital, three health centers, six lower private clinics, and 33 health posts. The total population of the district in 2019 is estimated to be 139,186, with an estimated 4830 pregnant women and 30,802 women of reproductive age (15–49 years), respectively. The district has 33 subdistricts, two urban and 31 rural, 13 and the study was conducted in eight randomly selected subdistrict from July 1, 2020, to August 31, 2020.
Study population and design
A community based cross-sectional study was used to assess the prevalence of unintended pregnancy and associated factors. The pregnant women living in Mi’eso district, West Hararghe were the study population.
Inclusion and exclusion criteria
All pregnant women residing for at least 6 months in Mi’eso district were included in the current study, while those who were seriously ill at the time of data collection and were unable to participate were excluded from the current study.
Sample size determination
Sample size was determined by using a single population proportion formula based on the assumption of unintended pregnancy (41.5%), 14 95% confidence interval, 5% margin of error, and 10% of non-response rate .

n = sample size
P = proportion of unintended pregnancy
d = desired degree of precision (5%)
Z = is the standard normal value at 95% confidence level
After considering 10% for non-response rate, the total sample size was 410 study participants.
Furthermore, in order to take the largest sample size, we have calculated it for the factors associated with unintended pregnancy among pregnant women using 95% CI and 5% for the margin of error, 1 for the ratio of unexposed to exposed, and 80% power using Epi Info version 7 and finally we got 508 study participants (Supplemental File I).
Sampling procedures and techniques
The study participants were stratified into rural (n = 31) and urban (n = 2) subdistricts. Then, one subdistrict from the urban area and seven subdistrict from the rural area were randomly selected. Then, samples were proportionally allocated to each kebele based on the number of pregnant women they had. Finally, using the health extension worker maternal registration book as a sampling frame, eligible women in each subdistrict were selected using simple random sampling.
Data collection methods
A structured questionnaire adapted from previous studies was used to collect data via a face-to-face interview at household level. A validated London Measure of Unplanned Pregnancy (LMUP) ; multidimensional scale that evaluates pregnancy intention using six domains, such as contraceptive use, timing, and feelings toward pregnancy is used to assess unintended pregnancy. The questionnaire contains variables on socio-demographic conditions, reproductive health characteristics, and the nature of pregnancy. The questionnaire was prepared in English, translated into the local language (Afan Oromo), and translated back to English by different researchers with good command of both languages. Six (nurse) midwives were recruited to collect data under the supervision of three supervisors. Two days of training were given for data collectors and supervisors on the data collection process: interviewing, respecting women’s rights, maintaining privacy and confidentiality, and the overall study objectives. Each questionnaire was checked for completeness and consistency daily.
Variables
Dependent variable: Unintended pregnancy among the women
Independent variables: ○ Socio demographic factors (age, income, occupation, marital status, educational level, religion, and residence). ○ Reproductive and contraceptive factors (awareness and knowledge about contraceptive, use of contraceptive, type of contraceptive used, autonomy of women to use contraceptive, discussion with husband about contraceptive, age at first pregnancy, desired number of children, gravidity, parity, and history of abortion). ○ Access to health information/service (travel time or distance, community health workers visit and exposure to mass media).
Operational definitions
Unintended pregnancy: is a pregnancy, which is either unwanted or mistimed at a time of contraception. 1 The mother was asked about contraceptive usage and agreement with her husband, timing of pregnancy, intention to became pregnant, desire, and preparation for becoming pregnant and then dichotomized and finally the scored less than three was considered as unintended pregnancy.
Unwanted pregnancy: The pregnancy occurred when no more children in the future or at present were desired. 1
Mistimed pregnancy: The pregnancy occurred earlier than desired. 1
Data quality control
Initially, the questionnaire was prepared in English and translated into the local language, Afan Oromo, and again back to English by another expert to check for its consistency. The questionnaire was pretested with 5% of the sample size in Asabot urban subdistrict. Two days of training were given for data collectors and supervisors regarding the basic principles of data collection procedures and techniques. The principal investigator and supervisors did day-to-day supervision during the data collection. At the end of each day, the questionnaire was reviewed and checked for completeness, accuracy, and consistency. Every questionnaire was checked before data entry by the principal investigator.
Data processing and analysis
All collected data was checked for completeness, clarity, and consistency. The data was coded, entered using Epi Data version 3.1, and exported to SPSS 21 for analysis. For univariate analysis, descriptive statistics such as frequency, percentages, measures of central tendency, and measures of dispersion were performed for analysis. For univariate analysis, descriptive statistics such as frequency, percentages, measures of central tendency, and measures of dispersion were performed. For univariate analysis, descriptive statistics such as frequency, percentages, measures of central tendency, and measures of dispersion were performed.
Binary logistic regression was used to test the association between independent variables and unintended pregnancy. All variables with p-value < 0.25 were entered into a multivariable logistic regression model to control the potential confounders. Associations were described using an adjusted odds ratio along with a 95% confidence interval, and a p-value of less than 0.05 in the multiple logistic regression was considered statistically significant. Model goodness of fit was checked using Hosmer Lemeshow test.
Results
Socio demographic characteristics
All 508 pregnant women approached responded, consented for the study and were included. Majority of participants were 18–35 years old, 431 (84.8%) with the mean age of 27.7 (±6.5) years. Majority of respondents were married, 484 (95.3%), rural residents 315 (62%), house wives 340 (66.9%), and Muslim 408 (80.3%; Table 1).
Socio demographic characteristics of pregnant women in Mi’eso district, West Hararghe, 2020 (n = 508).

Contraceptive and reproductive characteristics
Most of the women, 435 (85.6%), were aware of contraception, and 433 (85.2%) knew about contraceptive pills. More than half, 275 (54.1%) of them had ever used contraceptives. In addition, 159 (57.8%) women decided the type of contraceptive they used without discussion with their couples. More than half, 275 (54.1%) of them got first pregnant at the age of <20 years (Table 2).
Reproductive characteristics and contraceptive history of pregnant women in Mi’eso district, 2020 (n = 508).

Contraceptive use* :is a practice of using any of modern contraceptive methods to prevent pregnancy.
Access to health information
Almost half, 236 (46.5%) of the respondents were living at a walking distance of <30 min from the nearest health facility and were visited by health workers at their home 275 (54.1%). Almost two-thirds of the respondents, 322 (63.4%) reported having Television or Radio at home (Table 3)
Access to health information/services among pregnant women in Mi’eso district, 2020 (n = 508).

Descriptive analysis of unintended pregnancy and its associated factors
One hundred seventy-three (34.1%; 95% CI = 29.9–38.4) of the women reported that their index pregnancies were unintended: 136 (78.6%) mistimed and 37 (21.4%) unwanted. The most common reasons for failure to prevent the unintended pregnancy were not considering oneself as fertile, 51 (29.5%) and lack of knowledge about contraception, 39 (22.5%; Figure 1)

Reported reason for unintended pregnancy in Mi’eso district, West Hararghe Zone, 2020.
Bivariate analysis of factors associated with unintended pregnancy
In the bivariate analyses, age, educational status, residence, parity, age at first pregnancy, number of alive children, number of desired children, history of abortion, awareness about contraception, ever use of contraceptives, discussion about family planning with the husband, distance to the nearest health facility, visited by health workers at home and having TV/Radio in a home were the factors associated with unintended pregnancy (Supplemental File II).
In the multiple logistic regression, women who resided in rural areas were nearly three times more likely to experience an unintended pregnancy than those who resided in urban areas (AOR = 2.95, 95% CI: 1.7–5.12). A woman who had parity > 5 were three times more likely reported their pregnancy was unintended than whose parity one (AOR = 3.03, 95% CI: 1.5–6.02). In addition, women who got the first pregnancy at an age < 20 were 4.4 times more likely to have an unintended pregnancy when compared to the counterpart (AOR = 4.41, 95% CI: 2.6–7.4). The odds of an unintended pregnancy among women who had a history of abortion were 5.4 (AOR = 5.4, 95% CI: 3.1–9.5).
The odds of unintended pregnancy among women who had no awareness of contraception were 2.4 (AOR = 2.45, 95% CI: 1.2–5.2), and women who had no discussion about family planning with their husbands were 2.6 times more likely to experience unintended pregnancy than those who had a discussion with their husbands about contraception (AOR = 2.63, 95% CI: 1.5–4.5; Table 4).
Multivariate analysis of factors associated with unintended pregnancy among pregnant women in Mi’eso district, West Hararghe Zone, 2020.
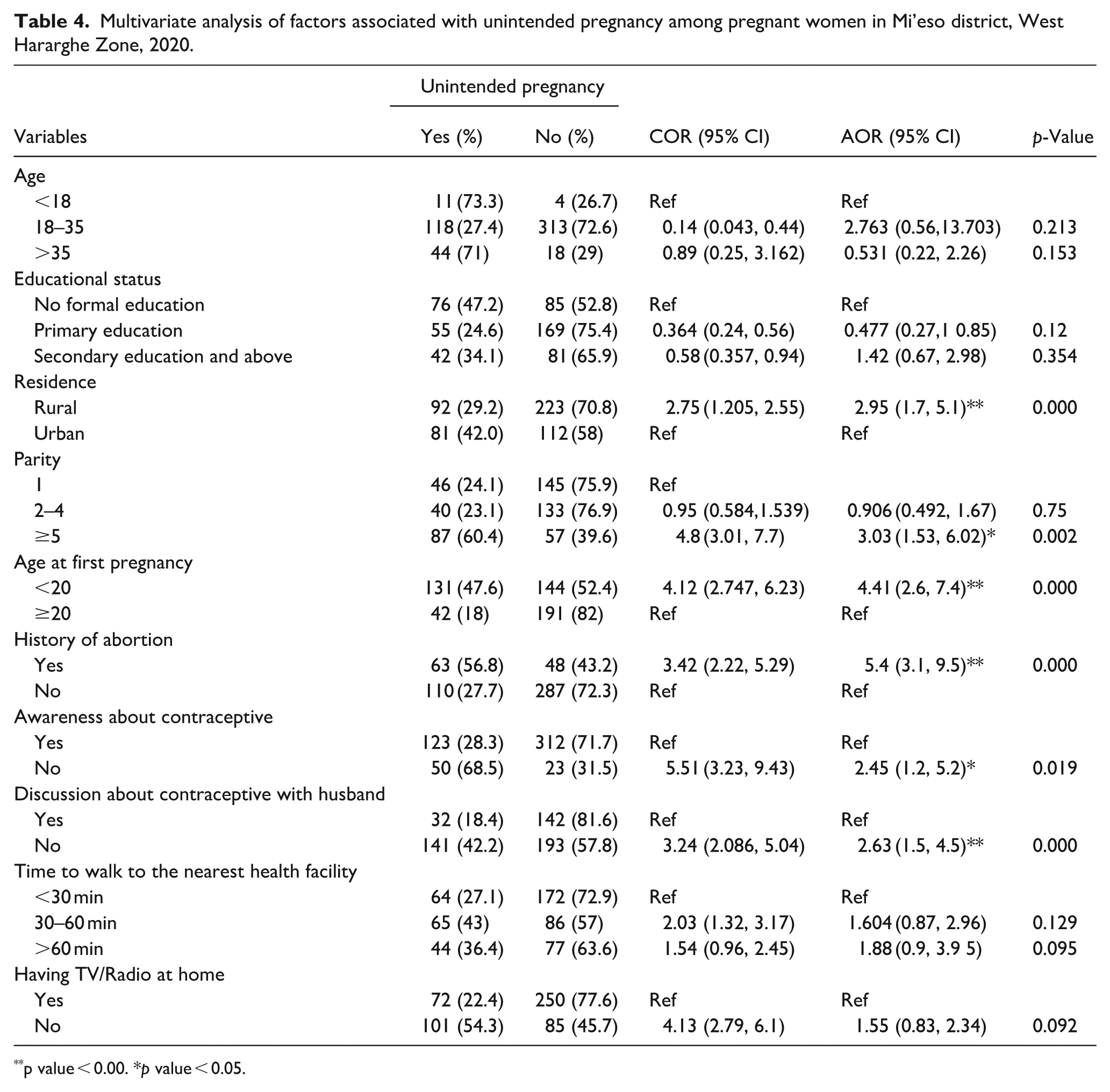
p value < 0.00. *p value < 0.05.
Discussion
This study was conducted to assess the magnitude of unintended pregnancy and its associated factors in Mi’eso district, West Hararghe Zone, Eastern Ethiopia. Almost three in ten pregnancies in the district were reported to be unintended, the majority of which were mistimed. Residence, abortion history, parity, age at first pregnancy, awareness about contraception, and discussion with the husband about contraception were associated with unintended pregnancy.
The prevalence of unintended pregnancy in this study is comparable with the studies conducted in Hadiya Zone (36.2%), Addis Ababa (36.4%), and Jimma Town (36.5%).7,15,16 It is, however, lower than reports from Ghana (40%), South Africa (64.3%), and Arsi Negele (41.5%).17–19 This might be due to the socio-demographic, sampling method, study design, and sample size differences between the studies. For instance, studies in Ghana were conducted nationally, while the convenience sampling method was used in South African studies and a large sample size was used in the Arsi Negele study.
But, compared to other studies in Ethiopia, our finding is higher: Welkaite (26.1%), Debre Birhan (23.5%), and Gelemso (27.1%).9,20,21 This difference may be due to differences in the availability, accessibility, and coverage of maternal health services, socio-cultural differences, and demographic differences between the current study and the previous studies. For instance, in this study area most of their life style was livestock and mobile from site to site. This may affect the accessibility and coverage of maternal health services in this study area. In addition, the difference may be due to the study setting with Gelemso 21 studies and sampling technique difference between the other studies which they used cluster rather than simple random sampling with after stratification in this study.9,20–23
The most common reasons for failure to prevent an unintended pregnancy were not considering oneself as fertile, a similar finding reported from a study done in Jimma. 7 This shows the existence of persistent gaps of information for creating awareness among reproductive-age women regarding the fertility period and appropriate use of contraceptives. It also matter on the time of decision for the time of contraceptive use.
The odds of unintended pregnancy among women who resided in rural was 2.9. This finding is supported by a study done in Addis Zemen, South Gonder North Ethiopia, which shows that women from rural areas were 2.6 times more likely to face an unintended pregnancy. 24 The association of residence may be due to the fact that women who are from rural areas may not easily access information regarding contraceptive methods.
The odds of unintended pregnancy among multiparous women were 3.03, which is consistent with the studies conducted in Gelemso (AOR = 4.76, 95% CI: 2.4–9.65), Addis Ababa (AOR = 2.8, 95% CI: 2.6–9.7), and West Wollega (AOR = 3.03, 95% CI: 1.13–8.08).20,24,25 Moreover, the reported association that an increased risk of unintended pregnancy with increased parity14,26 supports this finding. This is due to the fact that a high-parity woman might already have adequate children and have a lower fertility preference. In addition, it may be because a woman with high parity has attained her desired number of children and regards any additional child as unintended.
Women who got their first pregnancy at <20 years were 4.4 times more likely to have unintended pregnancy when compared to the counterpart. This might be the fact that awareness and level of decision-making increases with age and those who got their first pregnancy in teenagers may have low level of reproductive health knowledge and access to family planning services, and shamed to come the health facility to get reproductive health care. In addition, it might be that those who got pregnant at an early age would be less likely to attend and complete formal education, which may lead to a lower level of knowledge about family planning and the reproductive health system and contribute to a higher rate of unintended pregnancy.
The odds of unintended pregnancy among women who had a history of abortion were 5.38, which is comparable with studies conducted in Jimma (AOR = 2.6, 95% CI: 1.68–4.15) and Pakistan (AOR = 1.8, 95% CI: 1.2–2.1).17,27 This might be due to the fact that a woman who had a history of abortion might have believed that abortion was the consequence of an unintended pregnancy, as supported by the evidence that the frequent consequence of an unintended pregnancy was abortion 2 and the odds of an unintended pregnancy were higher among women who had a history of unintended pregnancy. 16 However, in contrast to the study conducted in Arsi Negele, which reported higher odds of unintended pregnancy among women who had no history of abortion than those who had a history of abortion (AOR = 1.962, 95% CI: 1.025–3.755). 14 The contrast may be due to the sampling technique and sample size, as the study done in Arsi Negele used a multistage sampling technique and a large sample size.
Women who have no or less awareness of contraception have higher odds of having an unintended pregnancy, which is consistent with findings reported in Ethiopia and different African countries.20,21,28,29 This is due to the fact that those women who had no awareness of contraception may not have used contraception, which led them to have an unintended pregnancy.
Women who had no discussion about family planning with their husbands were more likely to have unintended pregnancies. The women who had no discussion about contraceptive use with her husband had 2.63 time more likely to have unintended pregnancy. This finding is supported by studies conducted in Addis Ababa, Tigray, West Oromia, and multilevel analysis studies in Ethiopia.16,20,30,31 This implies that communication between couples regarding family planning helps women use contraceptive methods to prevent unintended pregnancy.
Limitation of study
This study didn’t cover variables like history of GBV and age difference between couples which may be important variables for assessment of unintended pregnancy. Furthermore, there might be social desirability bias as some women may be reluctant to admit a pregnancy was unwanted due to stigma or cultural norms. Moreover, dichotomizing intended pregnancy may not show the clear cut off unintended pregnancy.
Conclusion
The prevalence of unintended pregnancies in the study area was high as compared to other studies in Ethiopian. This indicates unintended pregnancy is one of the reproductive health problems that needs emphasis in the study area. Place of residence, parity, age at first pregnancy, history of abortion, awareness about contraception, and discussion about family planning with the husband were associated with unintended pregnancy. Common reasons given by women for not avoiding unintended pregnancy were not considering themselves fertile, lack of knowledge about contraceptives, forgetting contraceptives at the right time, fear of contraceptive side effects, and husband refusal.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251373007 – Supplemental material for Unintended pregnancy and its associated factors in Mi’eso Woreda, West Hararghe Zone, Oromia Regional State, Eastern Ethiopia
Supplemental material, sj-docx-1-phj-10.1177_22799036251373007 for Unintended pregnancy and its associated factors in Mi’eso Woreda, West Hararghe Zone, Oromia Regional State, Eastern Ethiopia by Kedir Hassen, Tadesse Dufera, Dechasa Adare Mengistu, Negga Baraki and Abera Kenay Tura in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251373007 – Supplemental material for Unintended pregnancy and its associated factors in Mi’eso Woreda, West Hararghe Zone, Oromia Regional State, Eastern Ethiopia
Supplemental material, sj-docx-2-phj-10.1177_22799036251373007 for Unintended pregnancy and its associated factors in Mi’eso Woreda, West Hararghe Zone, Oromia Regional State, Eastern Ethiopia by Kedir Hassen, Tadesse Dufera, Dechasa Adare Mengistu, Negga Baraki and Abera Kenay Tura in Journal of Public Health Research
Footnotes
Acknowledgements
We would like to thank Haramaya University, College of Health and Medical Sciences, School of Graduate Studies for allowing us to do this research. Moreover, we would like to thank the participants of this study, data collectors, and supervisors.
Ethical considerations
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences, Haramaya University (Ref No: IHRERC/161/2020). A Permission letter was obtained from the Woreda Health Office and the respective kebeles. Informed written and signed consent was obtained from the study participants. Confidentiality was kept by using anonymous codes, de-identified study participants’ identifiers, and keeping the data in a secured place.
Author contributions
K.H., A.K.T, and N.B. were all involved in the research concept, design, data collection, analysis, and interpretation. T.D and DAM wrote and revised the draft manuscript. All authors reviewed and contributed intellectual content to the draft manuscript. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All most all data are included in this manuscript. However, supporting information will be accessed from the corresponding author on the reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.