
Abstract
Background:
Cardiovascular diseases (CVD) are the leading cause of mortality and disability-adjusted life years (DALYs) worldwide. This study aimed to evaluate the association between low knowledge about cardiovascular disease, the absence of lifestyle changes after the COVID-19 pandemic, and cardiovascular risk among Peruvian resident.
Design and methods:
Analytical and cross-sectional study. The sample consisted of 371 participants. The Knowledge about Cardiovascular Diseases questionnaire, the Pocket Guide for estimating and managing cardiovascular risk, and the Changes in lifestyle during the quarantine period scale were used. Moreover, to establish independent associations of the variables of interest, the PRc and PRa of each factor were determined through Poisson regression models with robust variance.
Results:
About 60.4% of participants had changes in lifestyle after the pandemic, 69.8% had a low level of knowledge about the risk of cardiovascular disease, and 18.6% had a moderate-high cardiovascular risk. The bivariate analysis found that the population that did not change their lifestyles after the pandemic had a significantly higher cardiovascular risk than those who did make changes. Likewise, low knowledge about cardiovascular risk and disease was associated with a higher level of cardiovascular risk. The multivariate model showed that participants who did not have changes in lifestyle after the pandemic were 3.34 times more likely to have a higher level of cardiovascular risk (95% CI 2.09–5.34).
Conclusions:
Residents who did not have changes in lifestyle after the COVID-19 pandemic and expressed low knowledge about cardiovascular disease have a higher cardiovascular risk.
Introduction
Cardiovascular diseases (CVD) encompass disorders that affect the heart, coronary, and/or peripheral blood vessels. 1 Globally, they represent the leading cause of death and disability-adjusted life years (DALYs). By 2017, they were responsible for approximately 17.8 million deaths, more than 80% occurring in low- and middle-income countries (LMICs).1,2 According to the World Health Organization (WHO), it is projected that by 2030, they will cause 23.6 million deaths, with strokes and coronary heart diseases being the main contributors. 3
A significant burden of these deaths occurs in low- and middle-income countries, including Peru, where CVD rates are exacerbated by the presence of modifiable risk factors such as smoking, unhealthy diets, physical inactivity, obesity, and complications related to COVID-19 infection.3–5 Furthermore, the poor response of health systems, with great emphasis on the first level of care, in terms of close control and compliance with the treatment of people with CVD, may increase their mortality in the future. 6
During the COVID-19 pandemic, different health confinement strategies were implemented to avoid infection, giving disastrous results for healthy lifestyles such as physical activity and diet, as demonstrated by various studies.7,8 Furthermore, uncertainty, stress, social isolation, and less exposure to sunlight worsened sleep quality and altered lifestyle habits, seriously affecting health outcomes, quality of life, and healthy practices. 9
Additionally, it is known that the Peruvian health system has responded poorly to the challenges of the pandemic, which is why Peru is one of the countries with the highest number of deaths per number of infected people: for every 30 infected people, one died as of March 31, 2021. 10 Despite existing evidence, the impact of the COVID-19 pandemic has created additional challenges for the lifestyles of Peruvian families. The worry, fear, and anxiety associated with the disease may have decreased the population’s lifestyle practices, generating greater health vulnerability, which could increase the risk of suffering from CVD. 11
Given the importance of lifestyle behaviors in the prevention and control of CVD, it is critical to understand the factors that influence such behaviors. One key factor is knowledge about cardiovascular disease and its risk factors. A crucial step toward reducing cardiovascular diseases and improving cardiovascular health requires a public understanding of these factors.12,13 Studies have shown that knowledge of CVD and its risk factors can lead to success in its prevention and control by influencing individual attitudes and practices toward a healthy lifestyle, better treatment compliance, and decreased risk of disease complications. However, according to health behavior theories, knowledge alone may not always lead to behavior change.14,15
To frame this study, we adopted the Health Belief Model (HBM) as the theoretical framework. The HBM establish that health behaviors are influenced by individuals’ perceptions of their susceptibility to a disease, the severity of the disease, the benefits of taking preventive action, and the barriers to taking such action. It also highlights the role of cues to action and self-efficacy. 16 According to the HBM, knowledge about health behavior is a solid modifying factor for a healthy lifestyle. However, it must be combined with other factors such as good perceptions, positive attitudes toward health, and many other conditions such as socioeconomic factors. 17 Previous studies have also revealed that knowledge of specific risk factors is associated with healthy behavior. However, knowledge alone does not motivate behavior change. 18 Therefore, it is necessary not only to assess knowledge but also to observe actual lifestyle modifications after disruptive events like the COVID-19 pandemic.
Therefore, given that there are limited reports in Peru on knowledge of CV risk factors and lifestyle habits after confinement due to the pandemic. The objective of this study was to determine the association of low knowledge about cardiovascular disease and the lack of lifestyle changes after the COVID-19 pandemic with an increased cardiovascular risk among Peruvian residents.
Methods
Study design and setting
This was analytical cross-sectional study, conducted in a population center located in the Lima East region of Peru. The cross-sectional design allowed for the evaluation of associations between knowledge about cardiovascular disease, lifestyle changes after the COVID-19 pandemic, and cardiovascular risk at a single point in time.
Population and sample
The study population included residents aged 18 years or older living in the selected community. A sample size of 371 participants was determined using a sampling formula for proportions, assuming a 95% confidence level, a 5% margin of error, and an estimated prevalence of cardiovascular risk factors based on prior studies. A non-probabilistic convenience sampling method was used to recruit participants for this study. Inclusion criteria were: adults aged 18 years or older of both sexes, who voluntarily agreed to participate in the study. Those with a diagnosed history of high blood pressure, peripheral arterial disease, or other cardiovascular diseases, current use of lipid-lowering or antihypertensive medications, were excluded.
Data collection procedures
Data collection was carried out in person by trained personnel. Participants were approached in public spaces and invited to participate. After providing informed consent, participants completed a structured questionnaire, and their blood pressure was measured on-site following standardized procedures. The following sociodemographic data were collected: Age (young, adult, and older adult; 18–29, 30–59, 60+, respectively), marital status (married, cohabiting, divorced, single, widowed), sex, educational level, region of origin (coast, mountains, and jungle), religion, smoking status (yes/no), history of diabetes mellitus (yes/no). Systolic blood pressure (SBP) was measured using calibrated sphygmomanometers.
Variables and instruments
Knowledge about Cardiovascular Disease and Risk Factors was assessed using the validated Knowledge about Cardiovascular Diseases questionnaire by Muñoz et al. 19 It comprises 10 multiple-choice items that evaluate people’s knowledge about CVREF and CVD. It is one-dimensional and evaluates each correct question with 1 point and incorrect with 0 points. The final scoring scale considers a low level of knowledge with a score of less than 6 points, a regular level of 6–8 points, and a good level of more than 8 points. The questionnaire has good reliability (Cronbach’s Alpha of 0.72).
For the variable lifestyle changes after the COVID-19 pandemic, the questionnaire created by Vera and collaborators in Lima-Peru in 2020 was used, with adequate reliability (Cronbach’s Alpha of 0.80). It is made up of 25 items divided into 6 dimensions: Meat consumption (1–3), Cereal consumption (4–10), Fried food consumption (11, 17–19), Carbohydrate consumption (12–16), Harmful habits (20, 21), Physical activity (22), and Media (23–25). It has Likert-type response alternatives: (2) Increased, (1) Decreased, (0) Did not change, and (0) Does not consume/does not make/does not use. The final scoring scale classifies changes in lifestyles as there was a change (50–100 points), and there was no change (0–50 points). 20
The “Pocket Guide for the Estimation and Management of Cardiovascular Risk” created by the WHO in 2008 was used. 18 This study used the AMR D group tables for contexts where blood cholesterol cannot be measured. These tables allow us to measure the risk of suffering a cardiovascular event, fatal or not, for 10 years, according to sex, age, systolic blood pressure, tobacco consumption, and the presence or absence of diabetes mellitus. The final scoring scale classifies cardiovascular risk as low risk <10%, moderate risk 10%–20%, high risk 21%–30%, and very high risk >30%.
Statistical analysis
Data analysis was done using the R programing language version 4.0.2 (R Foundation for Statistical Computing, Austria. Depending on the categorical or numerical nature, the variables were described as absolute and relative frequencies (%), mean and standard deviation (SD), or median and interquartile range [IQR], respectively. For the comparative analysis, the Chi-square or Mann-Whitney U test was used depending on the nature of the variables and after a normality analysis through the Kolmogorov-Smirnov test. Poisson regression models with robust variance were used to establish independent associations of the factors of interest. These regression models provided the PRc (crude prevalence ratio) and PRa (adjusted prevalence ratio) of each factor, with their respective 95% confidence intervals (95% CI). A p < 0.05 was considered statistically significant in all analyses.
Ethical considerations
This study complied with the international ethical standards established in the Declaration of Helsinki (2000), and all procedures involving human subjects were approved by the Ethics Committee of the Faculty of Health Sciences of the Universidad Peruana Unión (Resolution N° 1784-2021/UPEU-FCS-CF). Participation was voluntary, and all participants provided written informed consent prior to enrollment. Confidentiality and anonymity of participant information were ensured throughout the study.
Results
The sample was made up of 371 people; the highest percentage were adults between the ages of 30 and 59 (58.2%), female (55.5%), single (36.4%), with completed secondary education (39.4%), coming from the Peruvian coast (57.7%) and who profess the Adventist religion (32.9%). The average of blood pressure was 130 mmHg, 23.7% are diabetic, 32.6% are smokers (Table 1).
General characteristics of the study population.
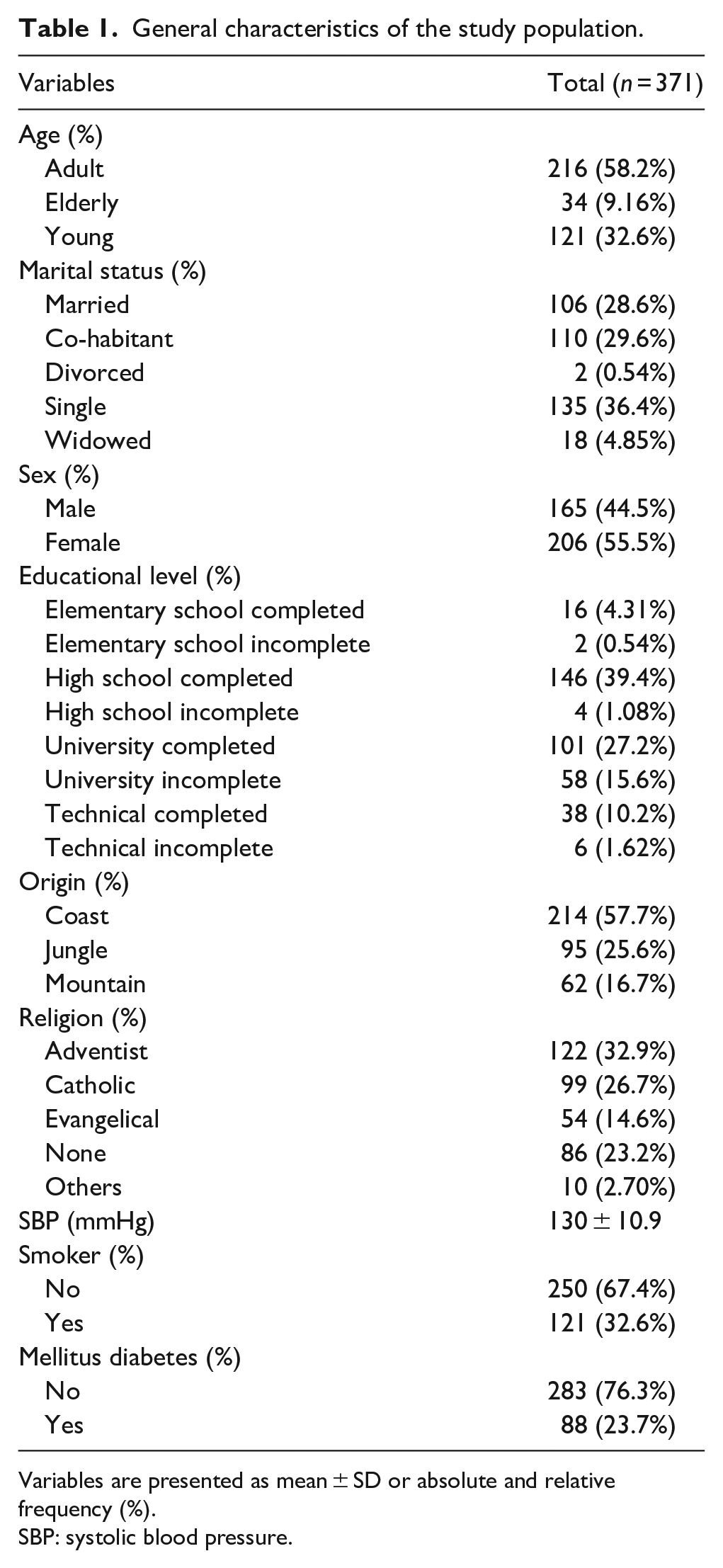
Variables are presented as mean ± SD or absolute and relative frequency (%).
SBP: systolic blood pressure.
Regarding the study variables, 60.4% had changes in lifestyle after the COVID-19 pandemic, 69.8% have a low level of knowledge about the risk of cardiovascular disease, and 18.6% present moderate-high cardiovascular risk (Table 2).
Characteristics of the study variables.

Variables are presented as absolute and relative frequency (%). To determine CVR and lifestyle changes, the Pocket Guide for the Estimation and Management of Cardiovascular Risk (AMR D group tables for contexts where blood cholesterol cannot be measured) and the Lifestyle changes during quarantine Scale were used, respectively.
CVR: cardiovascular risk.
Table 3 analyzes the characteristics of the population concerning cardiovascular risk. It was found that the population that did not change their lifestyles after the COVID-19 pandemic had a higher cardiovascular risk (36.1%) compared to those who did change their lifestyles, who presented a much lower level of risk (7.14%). Likewise, low knowledge about cardiovascular risk and disease was associated with a higher level of cardiovascular risk (26.6%). On the other hand, it was observed that older, married adults from the mountains and who profess the Catholic religion have a higher level of cardiovascular risk.
Comparison of variables according to cardiovascular risk.

Variables are presented as median [interquartile range] or absolute and relative frequency (%).
p < 0.05, statistically significant by Mann Whitney U or Chi-square.
The association between lifestyle changes after the COVID-19 pandemic and cardiovascular risk was evaluated through Poisson regression. It is observed that participants who did not have changes in lifestyle after the COVID-19 pandemic are 3.34 times more likely to have a higher level of cardiovascular risk (p-value < 0.001; Table 4).
Poisson regression models between lifestyle changes during the COVID-19 pandemic and moderate-high cardiovascular risk.

Poisson regression models with a multivariate approach are adjusted by marital status, origin, and religion.
PRc: the crude prevalence ratio; PRa: is the adjusted prevalence ratio.
p < 0.01, statistically significant by Poisson regression.
Discussion
The purpose of this research was to evaluate the association between knowledge about cardiovascular disease and changes in lifestyle after the COVID-19 pandemic with cardiovascular risk in residents of the Lima East region. It was found that the population that did not change their lifestyles after the COVID-19 pandemic had a higher cardiovascular risk compared to those who did make changes.
The main result of this research indicates that not having made changes in lifestyle after the COVID-19 pandemic increases the probability of having a 3.34 times greater cardiovascular risk. This result agrees with what was described by Illamola et al., who found that patients who previously had a moderate-high cardiovascular risk showed a decrease in the level of risk when subjected to changes in lifestyle. 21 Likewise, an intervention on lifestyles where the participants’ diet was based on the Mediterranean diet with significant energy restrictions and an excellent physical activity routine demonstrated decreased cardiovascular risk, with notable improvements in waist circumference, cholesterol, and triglyceride levels.22,23 In another similar intervention, CVR decreased, and improvements occurred mainly in fasting blood glucose and systolic blood pressure. 24 Therefore, maintaining correct adherence to healthy lifestyles is key to reducing the risk of CVD.
The literature indicates that the most significant lifestyle factor that favors the reduction of cardiovascular risk is the improvement in frequency and duration of physical activity. 25 The specific action on the cardiovascular system indicates an inverse relationship between habitual physical activity and the risk of coronary heart disease, cardiac events, and death. 26 In addition, physical activity has beneficial effects on lipid profile, body composition, aerobic capacity, and hemostasis, thereby reducing the risk of thrombosis. 27 A study after the pandemic in Peru showed that 41% of its participants never did physical activity, and 44% only did it between 1 and 2 times a week. 8 It is important to improve the practice of physical activity and lifestyles in this population that has been hit hard by the pandemic and thus reduce the risk of developing CVD.
In this research, it was also found that having a low level of knowledge about risk and cardiovascular disease is associated with higher CVR. This suggests that insufficient awareness or understanding of cardiovascular disease may contribute to behaviors or conditions that elevate cardiovascular risk. Although multiple variables were significantly associated with cardiovascular risk, the bivariate association between knowledge level and cardiovascular risk was particularly strong and consistent. This is similar to what has been reported in various studies, where they conclude that people who have adequate knowledge about cardiovascular risk factors have a lower cardiovascular risk.28,29 Likewise, another study reported that the majority of hypertensive patients who have good knowledge about cardiovascular factors and disease have more possibilities of reducing cardiovascular risk compared to hypertensive patients who have low knowledge on the subject. 30 These results indicate that knowledge is an essential and necessary factor to adopt appropriate actions to maintain good health, so it is necessary to implement strategies that not only raise the level of knowledge of the Peruvian population but also effectively motivate the adoption of a lifestyle associated with the reduction of cardiovascular risk factors and self-care of health.
Other significant results are the confirmation that being an older adult, smoking, and being hypertensive are associated with greater cardiovascular risk, as confirmed by various investigations that consider them among the main risk factors for cardiovascular disease.31,32 On the other hand, among the sociodemographic aspects, it was found that not professing any religion or being Catholic is associated with a higher level of cardiovascular risk compared to those who stated they belonged to the Adventist church. Some studies show that this religious community showed low levels of CVD risk factors associated with certain lifestyle practices, such as vegetarian diets and non-consumption of alcohol and tobacco.33–35
This findings highlights that behavior change is an essential component in cardiovascular prevention and supports the idea that knowledge alone may not be sufficient unless it translates into positive health behaviors. Taken together, our results suggest that promoting knowledge about cardiovascular disease, along with facilitating healthy lifestyle changes, could be important strategies in reducing cardiovascular risk at the population level. Public health interventions should focus not only on increasing awareness but also on enabling behavioral changes that are sustainable even during disruptive events such as pandemics.
This study has some limitations, the main one being that the participants were from Lima East region, which, added to the non-probabilistic sampling, limits the results’ ability to be generalized and extrapolated to a national context. Most information was collected through a self-reported survey, so social desirability or recall bias is likely, especially for the post-pandemic lifestyle changes variable. More objective measures of knowledge and comprehension could strengthen future analyses. Additionally, the cross-sectional design of the study precludes the establishment of causal relationships between knowledge level and cardiovascular risk. While a significant association was observed, it is not possible to determine whether low knowledge directly leads to higher risk or whether individuals at higher risk have inherently lower knowledge. Longitudinal studies would be necessary to better understand these causal pathways. Despite these limitations, we consider the study’s relevance due to the scarcity of information on knowledge of CV risk factors and lifestyle habits after confinement due to the pandemic in the Peruvian population. Likewise, the results prove the need to carry out interventions and programs based on pro-health habits to contribute to mitigating the high rates of cardiovascular diseases.
In conclusion, having low knowledge about cardiovascular disease and not presenting changes in lifestyle after the COVID-19 pandemic is associated with a greater cardiovascular risk, which is why intervention strategies must be implemented to improve knowledge, and lifestyles to reduce cardiovascular risk in the population.
Footnotes
Author contribution
Conceptualization, A.M.B.-V., B.M.G.-C., and E.E.N.-N.; methodology and formal analysis, E.E.N.N. and S.H.-V.; investigation, A.M.B-V. and B.M.G-C.; writing—original draft preparation, A.M.B-V., B.M.G-C., and E.E.N.-N.; writing—review and editing, S.H.-V.; supervision, S.H-V. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.