
Abstract
Background:
This paper primarily aims to construct a conceptual model of social determinants of health (SDoH), which will serve as a vital tool for identifying the feedback mechanisms that influence population health outcomes. Additionally, it seeks to simulate both the immediate and long-term effectiveness of proposed SDoH interventions on population health.
Design and methods:
We developed a system dynamics model of SDoH based on literature review and insights from community health experts. This model enables us to simulate the effectiveness of proposed interventions on population health, using CVD as a representative example of health outcomes.
Results:
The model results highlight a promising approach for enhancing population health. The neighborhood intervention stands out among the various interventions, demonstrating the most significant impact on health compared to other individual interventions. This finding underscores the potential of neighborhood-focused strategies in improving overall population health.
Conclusion:
This paper provides a clear explanation and causal framework for why investing in programs that enhance SDoH can improve population health. It introduces a powerful tool such as a causal map of SDoH, enabling policymakers and stakeholders to gain a more profound, dynamic understanding of the relationship between SDoH and health outcomes. This knowledge may help to make informed decisions and implement effective interventions.
Introduction
U.S. healthcare costs are projected to grow at an average rate of 5.5% per year from 2018 to 2027, reaching $6 trillion annually by 2027. 1 In response to this anticipated rise, policymakers and various stakeholders are exploring interventions to reduce healthcare expenditures and improve population health. Over recent decades, evidence has demonstrated that addressing social determinants of health (SDoH) enhances population health and equity2–7 and helps lower healthcare costs. Research indicates that clinical care—including access to and quality of care—contributes to approximately 20% of overall health outcomes. Social and economic factors and the physical environment account for about 50%. The remaining 30% is influenced by health behaviors such as alcohol consumption, diet and exercise, sexual activity, and tobacco use.8,9
Social determinants of health (SDoH) are social and environmental factors significantly influencing health outcomes. They encompass the conditions in which people are born, grow, live, work, and age, as well as the broader forces and systems that shape daily life, such as education, the physical and neighborhood environment, economic stability, access to nutritious food, community engagement, and the healthcare system. As their impact on health becomes increasingly evident, SDoH is gaining growing attention as a key target for intervention within the healthcare system.
A 2017 Kaiser Family Foundation survey of managed care organizations (MCOs) serving Medicaid beneficiaries revealed that many MCOs had implemented strategies to address social determinants of health (SDoH), focusing on housing, food and nutrition security, and non-emergency medical transportation. However, while the delivery of these SDoH services has increased, the impact on population health remains unclear. Furthermore, the causal pathways and mechanisms through which SDoH influence health outcomes, health disparities, and costs are still poorly understood or fully articulated. A study by Mahamoud et al. explored the interactions between SDoH and chronic disease outcomes, 10 while Braveman et al. examined the interconnections between macro- and micro-level SDoH. 4 Diderichsen and Hallqvist 11 outlined four key mechanisms—social stratification, differential exposure, differential susceptibility, and differential consequences—that contribute to health disparities addressed by SDoH. Despite this, much of the existing research on SDoH fails to recognize the synergies between these determinants, except for these studies12–16 that explore systems theory and SDoH. As a result, understanding the complex, synergistic relationships of SDoH remains largely theoretical for practitioners and policymakers, with limited insight into how these factors function, interact, and impact each other in a broader systemic context. This paper seeks to develop a conceptual model of SDoH factors, identify the feedback loops that influence population health outcomes, and simulate the short- and long-term effectiveness of hypothesized SDoH interventions on population health. This research is crucial for expanding the evidence base and providing a compelling rationale for investing in programs that enhance social determinants of health (SDoH) to reduce health disparities, improve population health outcomes, and lower healthcare costs.
The model developed herein will serve as a preliminary insight model that allows for a better understanding of the dynamic interrelationships among SDoH factors and the apparent effect of individual and combined SDoH interventions on population health outcomes.
Methods
A system dynamics model17–20 was developed through an extensive literature review and consultations with community health experts with significant expertise in population health. The qualitative literature review involved a systematic search across multiple databases, including PubMed, MEDLINE, EMBASE, Cochrane Library, and SCOPUS, using search terms such as: (“social determinants of health OR structural determinants of health OR socioeconomic factors OR social drivers of health”) AND (“health outcomes OR impact OR health OR wellbeing OR population health OR CVD”). The model simulated the short-term and long-term effects of hypothesized interventions on population health, using cardiovascular disease (CVD) as a proxy, given that CVD is the leading cause of mortality in the USA and many other countries.
The primary aim of this research was to develop a simulation model that sheds light on the interactions among SDoH factors and the feedback structures influencing population health outcomes, based on stylized inputs. System dynamics models offer a robust environment to simulate interventions and their combinations, which may be (a) costly, (b) result in unintended consequences, and (c) difficult to reverse once implemented.
The modeling process and insights generated facilitate active stakeholder engagement, enabling the sharing and refinement of mental models regarding complex public health issues. System dynamics models have increasingly been applied to tackle such complexities to improve population health.10,21–24,25,26 The development process involved creating a conceptual model of SDoH factors and their feedback loops, supported by evidence from the literature. The Appendix 1 includes a comprehensive list of references detailing the causal relationships within the model. Finally, the conceptual model was presented to community health experts to validate its structure and assumptions about causal relationships, ensuring its alignment with existing evidence. We employed Group Model Building (GMB)27,28 methods, a well-established participatory approach within system dynamics, to engage stakeholders in developing conceptual models for addressing complex issues, thereby enhancing understanding. A total of 10 community health experts, with expertise in medicine, population health, primary care, and system science, participated in a 2-h meeting to review the conceptual model structure. These experts brought valuable lived experience and an in-depth understanding of the social, economic, and environmental factors influencing individual behavior, risk, and health outcomes.
Using GMB techniques, including structured small group exercises called scripts, the conceptual model—developed from evidence in the literature—was reviewed for its realism, clarity, and ability to address key issues. For realism, the experts assessed whether the model’s structure aligned with existing knowledge of the system, specifically regarding social determinants of health and their impact on health outcomes. For clarity, they evaluated whether the proposed relationships between variables were supported by evidence. Lastly, to ensure the model captured the essential issues, they examined whether all relevant components of social determinants of health were included as identified in the literature.
The authors refined the SDoH model through an iterative process in collaboration with community health experts. After validation, the model was parameterized using synthetic data. Finally, base case and alternative scenarios were simulated to generate insights into the effects of SDoH interventions on population health.
Model structure
The model structure used herein represents the dynamic relationship of SDoH factors on population health. For simplicity, we described population health herein with two stocks: a healthy population and a post-CVD population. The healthy population is assumed to have no health issues or asymptomatic or stable symptomatic chronic diseases with no CVD history. In contrast, the post-CVD population is individuals who have survived CVD events. Because this is a simplified, stylized model mainly for insight generation, the healthy and post-CVD populations were not disaggregated by age, gender, race, and presence of hypertension, diabetes, cholesterol, and smoking, which are important risk factors in determining the risk of CVD events and mortality. Demographic factors and other sociocultural factors were excluded from the model to reduce detail complexity and focus on dynamic complexity (feedback mechanisms) and the broad impacts of SDoH interventions. Future model iterations will incorporate these demographic factors to improve model projection accuracy and nuanced understanding.
The healthy population increases via births and decreases by CVD incidence. Birth is determined by birth rate and healthy population herein because we assumed that most post-CVD populations would be over 50 years old. The healthy population, CVD incidence rate, and the proportion of the population with CVD risk factors determine CVD incidence.
Similarly, the post-CVD population increases due to CVD incidence and decreases due to CVD mortality. CVD mortality is assumed to be influenced by the post-CVD population and the CVD death rate, which is influenced by the utilization of healthcare services. As shown in Figure 1, the feedback mechanisms of SDoH factors influence population health in our simplified model through (a) CVD incidence by changing the proportion of the population with CVD risk factors and (b) CVD mortality by changing the CVD death rate through access to healthcare services.
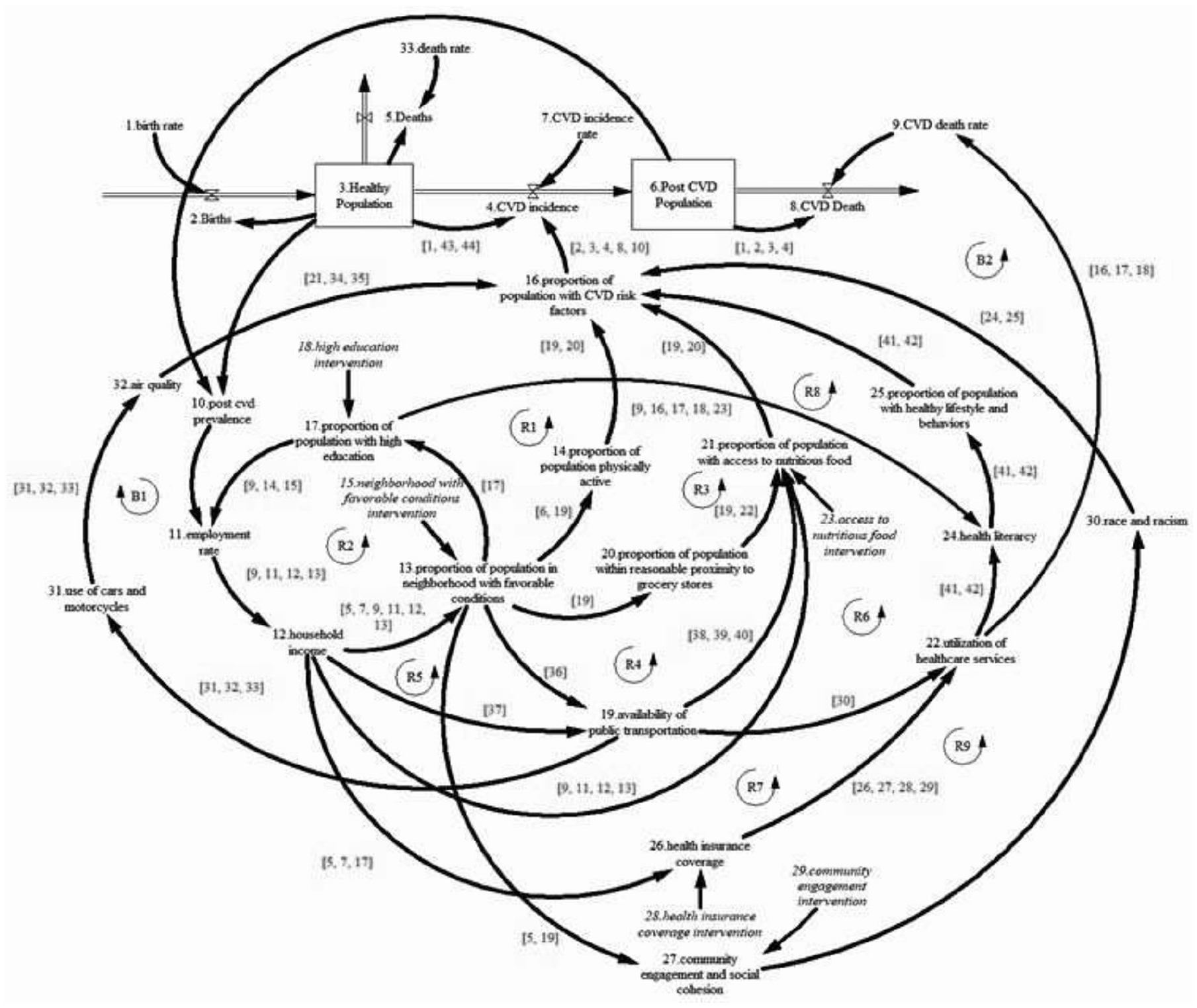
Conceptual model of social determinants of health.
Table 1 shows all the feedback loops of the conceptual model. Feedback loops R1 and R2 show the effects of education, employment/income, and favorable neighborhoods on the population with CVD risk factors. For this model, favorable neighborhoods are neighborhoods with access and proximity to grocery stores with healthy food, public transportation, green places that promote physical activities, and a community that supports social cohesion. For feedback loop R1, we hypothesize, based on an extensive literature review, that as population health improves, post-CVD prevalence will decrease, improving the population available for work and employment. As employment increases, household income increases, affecting families’ ability to rent or buy houses in favorable neighborhoods. As the proportion of the population living in favorable neighborhoods increases, access to neighborhoods with an environment that promotes physical activity will increase. This is assumed to increase the ratio of the physically active population. An increase in physical activity is believed to decrease the population with CVD risk factors, which in turn will diminish, all things being equal, the CVD incidence. For feedback loop R2, as the employment rate increases, household income is anticipated to increase, increasing the population living in neighborhoods with favorable conditions due to increased income. Living in a neighborhood with favorable conditions is presumed to increase access to quality education, which will, in turn, increase the likelihood of attaining a high degree (completing college), employment, and income to afford to live in a neighborhood with favorable conditions. Feedback loops R3, R4, and R5 account for the effect of access to healthy and nutritious food on CVD risk factors. As captured in feedback loop R3, living in a favorable neighborhood increases proximity to grocery stores with healthy food options. All things being equal, we presumed that access would increase healthy food consumption and decrease CVD risk factors. Likewise, as in feedback loop R4, favorable neighborhoods increase access to public transport and the distance and transportation cost associated with accessing grocery stores with healthy food options. As a result, healthy food consumption is assumed to increase and decrease CVD risk factors. Feedback loop R5 demonstrates that though proximity and availability of public transport are essential to access healthy food, household income, which determines the household’s ability to purchase healthy food, is vital. Thus, increasing household income increases purchasing power and availability of transportation options for healthy food, decreasing CVD risk factors and incidence of CVD.
SDoH conceptual model causal pathways.

The effects of health literacy, health insurance coverage, and social cohesion on population health are captured by feedback loops R6, R7, R8, and R9. For feedback loop R6, living in a favorable neighborhood increases access to public/private transport, impacting healthcare service utilization. As healthcare services use and interaction with the health system improve, health literacy will increase, leading to a healthy lifestyle and behaviors and decreasing CVD risk factors. On feedback loop R7, it is hypothesized that an increase in household income will increase the ability of the household to purchase health insurance coverage, which will increase the use of healthcare services. As healthcare service use increases, healthy lifestyles and behaviors are assumed to improve, decreasing CVD risk factors. Feedback loop R8 establishes that health literacy can improve as educational levels increase, impacting lifestyle changes and CVD risk factors. Likewise, feedback loop R9 shows that living in a favorable neighborhood increases community engagement and social cohesion among residents, improving race and racism-related issues and impacting risk factors for chronic diseases. As race and racism-related issues decrease, we presumed that CVD risk factors would improve.
Lastly, feedback loop B1 describes the negative impact of transportation (mainly the use of cars) on air quality and CVD risk factors. Also, feedback loop B2 shows how access to and utilization of healthcare services are hypothesized to decrease the CVD death rate and mortality, thus increasing the survival of the post-CVD population.
Assumptions
For this model, we assumed that only individuals in the healthy population could give birth and that all the healthy population could give birth. The “fraction of the population with CVD risk factors” describes all CVD risk factors. Also, CVD mortality is presumed to be influenced only by healthcare utilization. We assumed that a delay time of 15 years is required for educational interventions to impact the employment rate. Likewise, for community engagement and cohesion, health insurance coverage, and access to nutritious food, a delay time of 2 years was assumed. Lastly, we presumed that neighborhood interventions have a delay time of 5 years to influence a change in physical activities, proximity to grocery stores, and public transportation. The conceptual model discussed herein is for insight generation; hence, we excluded age, gender, and ethnicity to reduce complexity. We also assumed that the effect of air quality, transportation, income, health insurance coverage, healthy lifestyle, post-CVD, neighborhood, physical activity, nutritious food, education, proximity to groceries, and racism on outcomes of interest are the same, with an assumed value of 0.2. Table 2 shows the model parameters used to initialize the SDoH model.
Model input.

Steady-state
We used stylized numbers since the SDoH model generates insights and explores interventions. For transparency and seamless discerning of intervention impact, the model was initialized in a steady state, a hypothetical situation where the healthy and post-CVD populations are at an equilibrium. For a steady state equilibrium, the following assumptions were made: first, births, CVD incidence, and CVD deaths are considered the same and remain constant over the simulation time. Second, the characteristics of the population (i.e. education, access to nutritious food, proportion in the favorable neighborhood, community engagement, and access to health insurance coverage) remain unchanged over the simulation time. It is important to emphasize that the initialized steady state is a dynamic equilibrium, where the steady state is numerically sensitive to model parameters, but consequent model behavior is not.
Parameter sensitivity analysis
We performed a sensitivity analysis to explore how a change in selected model parameters will impact outcomes of interest. For a one-way sensitivity analysis, 20 the values of the chosen model parameters were varied by ±40%, and a uniform distribution for each parameter range was assumed. The model was run 500 times for each parameter change, and each run drew a parameter value from a uniform distribution.
Intervention experiments
Base case: The base case is the steady state where all model parameters remain unchanged over the simulation time. Education intervention: Under this intervention, the proportion of the population with high education is assumed to increase by 4.5% annually from time 20 to 100. Neighborhood intervention: The proportion of people in a neighborhood with favorable conditions is thought to increase by 4.5% annually from time 20 to 100. Access to nutritious food intervention: The proportion of the population with access to nutritious food is assumed to increase by 4.5% from 20 to 100 annually. Community engagement intervention: Under this intervention, community engagement and cohesion are presumed to increase by 4.5% per annum from time 20 to 100. Health insurance intervention: The proportion of the population with health insurance coverage is assumed to increase by 4.5% annually from time 20 to 100. Combined intervention: For the combined interventions, the education, neighborhood, access to nutritious food, community engagement, and health insurance interventions are implemented simultaneously over the simulation time. We assumed an equal annual increase for all the interventions to ensure that simulation outcomes are due to the strength of the feedback mechanisms generated by the interventions, not the magnitude of the intervention change.
Results
The results, as shown in Figure 2, show the base case (steady state) and the impact of different SDoH interventions on the outcomes of interest: total population, healthy population, the proportion of people with CVD risk factors, post-CVD population, CVD incidence, and CVD death. Based on the stylized numbers used, under the base case (steady state), the total population is presumed to be 2 million and remain unchanged over the simulation time, while the healthy population is assumed to be 1 million and remains unchanged. Likewise, CVD incidence, deaths, and post-CVD population are presumed to be 5000, 5000, and 1 million individuals, respectively. The fraction of people with CVD risk factors is estimated to be 35% over the simulation time. Alternatively, the implementation of the education interventions shows that at the end of the simulation (by time 100), the total population will increase by 4.5% compared to the base case. In comparison, the healthy population is 7.1%, and the post-CVD population is 2%. However, the fraction of people with CVD risk factors is projected to decrease by 5% by time 100 compared to the base case, while CVD incidence is projected to increase by 2%, and CVD deaths remain unchanged. For the neighborhood interventions, the total population is expected to increase by 23.4%, the healthy population by 38.9%, and the post-CVD population by 8%. Also, the CVD incidence and deaths will increase by 14% and 4%, respectively. However, the fraction of people with CVD risk factors is expected to decrease by 18% compared to the base case at the end of the simulation. For the access to nutritious food and community engagement interventions, the total population is projected to increase under each intervention by 8.6%, the healthy population by 13.8%, and the post-CVD population by 3%, respectively. CVD incidence and deaths are projected to increase by 6% and 3%, respectively, compared to the base case. However, the fraction of the population with CVD risk factors is expected to decrease by 6%. The health insurance coverage intervention is expected to increase the total, healthy, and post-CVD populations by 2.4%, 0.1%, and 5%, respectively. While no change is anticipated for CVD incidence and the fraction of people with CVD risk factors, CVD deaths are projected to decrease by 1% at the end of the simulation. Lastly, under the combined intervention, the total, healthy, and post-CVD populations are expected to increase by 51.4%, 83.6%, and 19%, respectively. CVD incidence and deaths are projected to increase by 26% and 6%, respectively. In comparison, the fraction of the population with CVD risk factors is projected to decrease by 32% at the end of the simulation.
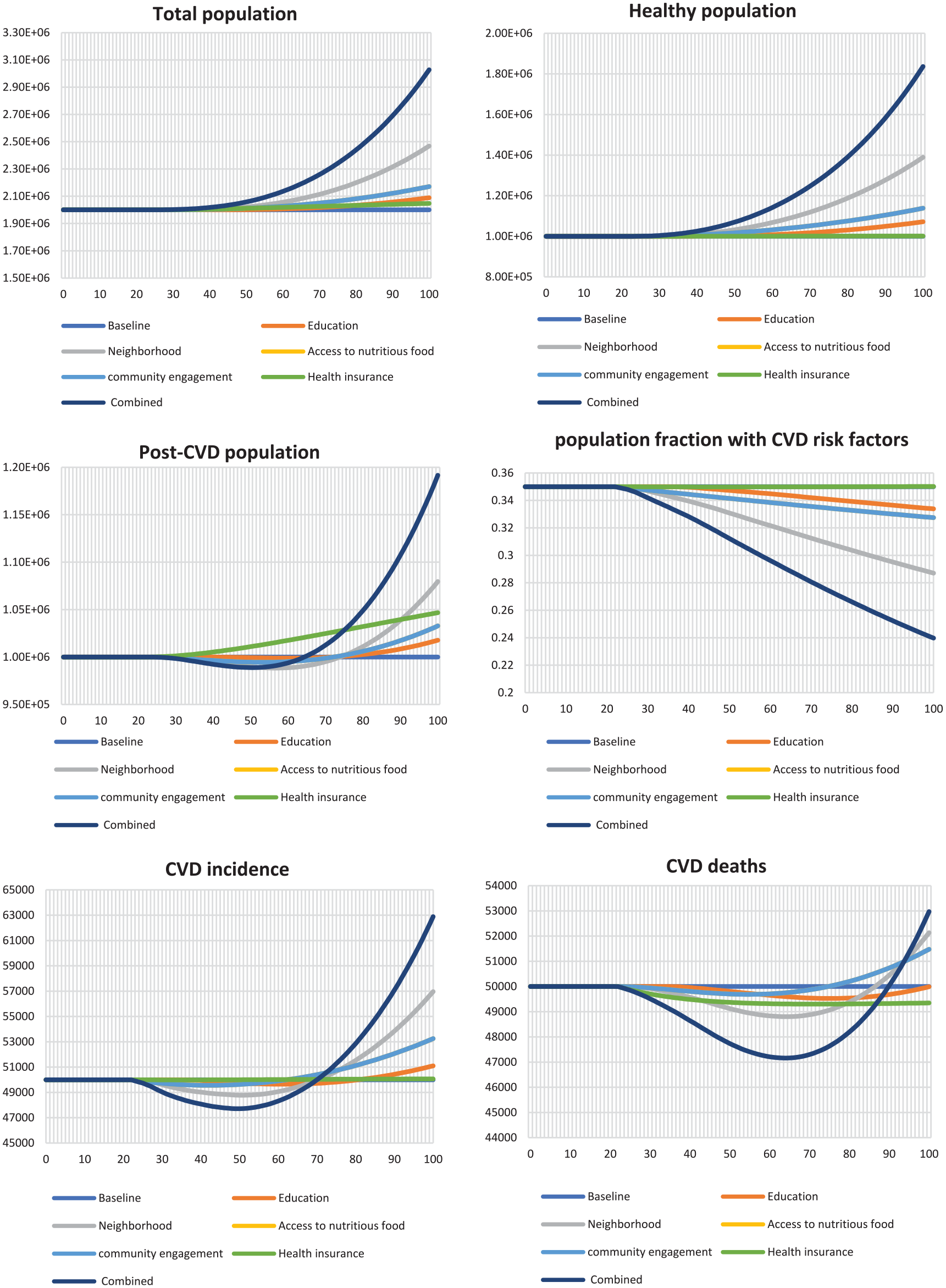
Impact of social determinants of health interventions on cardiovascular disease outcomes.
In the short, medium, and long term, implementing the SDoH interventions will increase the total and healthy populations while decreasing the number of people with CVD risk factors. In contrast, the post-CVD population, CVD incidence, and CVD deaths show a decreasing trend in the short to medium term and an increasing trend in the long term. In the short-term to long-term (i.e. 50 years on average), investment in SDOH is expected to decrease CVD incidence, post-CVD population, and deaths, except for the health insurance intervention that increases post-CVD population as CVD deaths decline without a corresponding reduction in incidence. Counterintuitively, the successful nature of the SDOH interventions suggests that more people are expected to survive CVD incidence, leading to an increased number of people with post-CVD. Thus, in the longer term (i.e. >50 years), as the healthy population increases, the number of people with CVD incidence increases more than the deaths, causing the post-CVD population to increase over time. As the post-CVD population increases, CVD deaths begin to grow as well.
Discussion
The results from the stylized model suggest that investing in programs that enhance social determinants of health (SDoH) can significantly improve overall health, reduce the risk of cardiovascular disease (CVD), and strengthen population well-being.
Among all the interventions, the neighborhood intervention had the most significant impact on population health compared to any single intervention. This was evident in a substantial increase in the healthy population and a notable reduction in the proportion of individuals with cardiovascular disease (CVD) risk factors. In the short to medium term (approximately 50 years), the neighborhood intervention decreased the post-CVD population, CVD incidence, and CVD-related deaths. However, in the long term (beyond 50 years), demographic dynamics and the lasting impact of the intervention are expected to result in an increase in the post-CVD population, CVD incidence, and CVD deaths. The neighborhood intervention promoted greater community engagement, better access to high-performing schools and colleges, sidewalks, green spaces, local grocery stores, and public transportation. These improvements enabled individuals to (a) obtain a high-quality education that opened better employment opportunities, (b) engage in physical activity in open spaces, (c) access healthier food, (d) receive healthcare services, and (e) participate more actively in community life. Insights from this simplified SDoH simulation model support findings by Dwyer-Lindgren et al. 29 that zip code matters more than genetic code regarding health outcomes. This reinforces that social, economic, and environmental factors play a much more significant role in determining population health than clinical care alone. Our results suggest that neighborhood interventions can significantly reduce CVD risk and improve survival rates, preventing many avoidable CVD deaths. However, as anticipated, a comprehensive intervention addressing all SDoH factors simultaneously will significantly improve population health and reduce health disparities. This underscores the importance of addressing all SDoH collectively for meaningful health improvements.
Community engagement and access to nutritious food interventions had an immediate and significant impact on the outcomes of interest. In contrast, the education intervention demonstrated a considerable delay before its effects were shown. However, it is crucial to highlight the importance of education intervention, as quality education enhances employment opportunities and promotes settlements in neighborhoods with better conditions.
Compared to the base case, the post-CVD population increase reflects avoidable CVD deaths resulting from implementing SDoH interventions. Given the model’s simplified structure, these interventions significantly reduce the risk of CVD, decreasing CVD incidence. Reducing CVD incidence increases the healthy population, boosting births and population size. In the long term (over 50 years), the incidence of CVD is projected to rise relative to the base-case scenario due to a larger healthy population, which leads to a higher number of CVD cases and deaths.
There are several limitations in the model. First, it assumes a uniform effect size for all SDoH interventions. Still, the impact of education, neighborhood improvements, nutritious food access, community engagement, and health insurance on population health may vary. Evidence from studies designed to assess these interventions’ specific effects is needed. Second, the model does not account for key risk factors such as age, gender, race, hypertension, diabetes, and smoking, all of which are significant determinants of CVD risk and mortality. A more tailored model, which includes these factors, would better reflect real-world dynamics and improve its applicability, something the authors are actively working on. Third, certain direct links between SDoH factors and CVD—such as the impact of racism—may operate through intermediate variables that were not captured in the conceptual model. Developing a more detailed model that includes these intermediaries would offer more profound insight into the pathways through which they affect population health. Fourth, we assumed that all births result in healthy infants. Although babies can be born with cardiovascular disease, it’s typically referred to as congenital heart disease (CHD) rather than cardiovascular disease (CVD), which is more commonly used to describe conditions that develop later in life (like heart attacks or strokes). Lastly, using stylized data means the model is primarily designed to generate insights into the feedback mechanisms driving the relationship between SDoH and population health. Despite these limitations, the model can be a valuable tool for policymakers, activists, and organizations advocating for SDoH interventions to address health disparities, especially in disadvantaged communities. This model can enhance mental models and generate insights to guide effective communication.
To move beyond these limitations, future studies should use available data to estimate the distinct effect sizes of various SDoH factors, such as education, neighborhood conditions, access to healthy food, community engagement, and health insurance. Such estimations are essential for informing policy decisions regarding interventions. Current risk prediction tools, like the Framingham risk equation, UKDPS risk engine, and Pooled Cohort risk estimator, account for traditional risk factors (age, gender, race, hypertension, diabetes, cholesterol, smoking) but exclude SDoH factors. Future research should also conduct sub-analyses to explore how SDoH interventions impact different demographic groups. This would include examining how combinations of factors, such as age, gender, and race, influence health outcomes. Longitudinal datasets will be crucial for understanding the long-term and differential impacts of SDoH on population health.
Conclusion
This paper offers a clear explanation and causal framework for how investing in programs that enhance SDoH can improve population health. This is crucial because when policymakers and stakeholders prioritize population health, understanding how SDoH factors interact and influence health outcomes will help ensure that effective interventions are identified, supported, and funded for implementation.
In light of these findings, policymakers and stakeholders must recognize that improving a single social determinant of health (SDoH) in isolation is unlikely to yield meaningful improvements in population health. A comprehensive, coordinated approach that addresses all dimensions of SDoH is essential. Since no single organization can tackle these challenges alone, collaboration across sectors and institutions is critical. The stylized simulation model can serve as a valuable tool to engage diverse stakeholders and align them around a shared roadmap for advancing population health and promoting health equity.
Footnotes
Appendix 1
Acknowledgements
We thank our community health experts for reviewing the simulation model and providing valuable feedback. We are also grateful for the Pilot grant received from the ACHIEVE GREATER trial (P50 MD017351; Levy, PI).
Ethical considerations
The Case Western Reserve University institutional review board approved this study. This study did not involve human participants and used only publicly available data. Therefore, informed consent was not required. The research protocol was reviewed and determined to be exempt from institutional ethics review by the Case Western Reserve University Institutional Review Board.
Author contributions
J.P. Ansah and R. Salazar designed and conducted the study. Together, they developed the simulation model, engaged with experts, and conducted the model analysis. J.P. Ansah, R. Salazar, and A. Elamin collaboratively wrote the manuscript, with A. Elamin also reviewing it and contributing content expertise.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received a pilot grant from the “Addressing Cardiometabolic Health Inequities by Early PreVEntion in the GREAT Lakes Region” (ACHIEVE GREATER) trial (P50 MD017351; Levy, PI) for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data sets used or analyzed for the study are available upon reasonable request.