
Abstract
Background:
Respiratory diseases rank second in global morbidity and mortality. By 2020, mortality from these conditions surged by 39.8% due to increased incidence and COVID-19-related deaths.
Objectives:
This study aimed to identify preventable mortality and total mortality from respiratory diseases in Kazakhstan from 2011 to 2021.
Design and methods:
Data from the National Statistics Agency of the Republic of Kazakhstan were analyzed. Preventable mortality rates were calculated across 5-year age groups (i.e. 0, 1–4, 5–9, . . ., 74+) and by gender using respiratory disease mortality data from 2011 to 2021. In addition, 95% confidence intervals (95% CI) for the age group of 0–74 years and gender factors were calculated to ensure statistical reliability.
Results:
Preventable mortality levels have more than doubled by 2021, reaching 156.19 per 100,000 population, with a significant increase in 2020. Preventable mortality among men was consistently three or more times higher than among women. The average annual percentage change increased by 7.5% (95% CI: 3.1; 12.2), from 2011 to 2021, where the rate was higher among women 9.2% (95% CI: 4.8; 13.9), compared to men (6.6% [95% CI: 0.9; 12.7]). Our findings strongly indicate that mortality rates will continue to rise by 2026, underscoring the urgent need for the scientific community and governments to collaborate in preventing further escalations of respiratory diseases.
Conclusions:
The study seeks to project the future prognosis of respiratory disease-related mortality and to highlight the need for targeted health strategies to reduce avoidable deaths through targeted health strategies with cooperative measures.
Introduction
The average life expectancy in Kazakhstan is 73.89 years in 2023, significantly lower than in the top 30 developed countries, where the average life expectancy exceeds 80 years. 1 Non-communicable diseases (NCDs) remain the leading causes of death in Kazakhstan, reflecting substantial health challenges in the region. Kazakhstan’s health policy aligns with the Sustainable Development Goals (SDGs) to reduce non-communicable disease (NCD) mortality by 2030, combat risk factors, and ensure universal access to quality primary healthcare.
Respiratory diseases are a major contributor to global morbidity and mortality, ranking second after cardiovascular diseases. More than 545 million people (7.4% of the world’s population) suffer from chronic respiratory diseases, including asthma, chronic obstructive pulmonary disease (COPD), interstitial lung diseases, pneumoconiosis, and other conditions, contributing significantly to premature morbidity and mortality worldwide. 2 The mortality rate from respiratory diseases has steadily decreased in recent years, reaching 87.9 per 100,000 people by 2019, compared to 105.0 per 100,000 people in 2015. Following the emergence of COVID-19, mortality rates due to respiratory diseases increased by 39.8% in the population. The mortality rate is decreased in 2021 to 108.8 per 100,000 people, which constituted 11.4% of all mortality. 3
Rutstein et al. 4 proposed using the indicator of avoidable mortality to assess healthcare quality. Later, Papanicolas et al. 5 suggested the use of preventable mortality as an indicator to evaluate the achievement of public health activities and some SDG indicators, since a comparison between countries, the collection of data for calculating this indicator is convenient and unified, in comparison with others such as alcohol consumption or smoking.
The World Health Organization (WHO) defined premature mortality as the probability of dying between the ages of 30 and 70 from cardiovascular diseases, diabetes, cancer, or chronic respiratory diseases. In Kazakhstan, the premature mortality rate from major non-communicable diseases showed a slight downward trend, decreasing from 20.84% in 2016 to 20.48% in 2020. 6 However, this means that over one in five individuals in Kazakhstan is at risk of dying prematurely before the age of 70, underscoring the need for effective public health interventions. High rates of premature mortality from specific conditions can indicate deficiencies in the timeliness and adequacy of medical care.
Avoidable mortality includes deaths that could have been prevented or effectively treated through improved public health policies. Preventable mortality is defined as deaths that could have been prevented, and treatable mortality refers to deaths that could have been prevented through effective medical interventions and timely treatment. These key indicators play a crucial role in assessing the effectiveness of the healthcare system. By examining preventable mortality rates, healthcare policymakers and providers can identify areas where the healthcare system may fall short and target these areas for improvement. 7
This study aimed to identify preventable mortality and total mortality from respiratory diseases in Kazakhstan from 2011 to 2021.
Methods
Data source
Data analysis was extracted from the National Statistics of the Agency of the Republic of Kazakhstan (https://stat.gov.kz). Then, we calculated Crude mortality as the number of deaths in a population during a specific period divided by the total population at risk during the same period. To calculate avoidable mortality by age categories in the Republic of Kazakhstan, mortality rates due to respiratory diseases were analyzed from 2011 to 2021. The data was disaggregated by gender and age groups, with age intervals of 5 years (0, 1–4, 5–9, 10–14,. . ., 74+). The raw deaths and population size data were obtained directly from the statistical database. Calculations for age-specific and gender-specific avoidable mortality rates were performed using this data. The retrieved data already contained gender- and age-specific mortality figures. We calculated avoidable mortality rates using this data by applying predefined criteria for preventable deaths.
The concept of avoidable mortality is used by the Organisation for Economic Co-operation and Development (OECD)/Eurostat in their lists of preventable and treatable causes of death (January 2022 version). 7 For this research, we used the definition of avoidable mortality given by the United Kingdom Office of National Statistics. 8 Based on the methodology, avoidable mortality consists of two components: the sum of preventable and treatable mortality. In the group of respiratory diseases, the following diseases are identified as 8 :
- preventable mortality– J09-J11 (influenza); J13-J14 (pneumonia due to Streptococcus pneumoniae or Haemophilus influenzae); J40-J44 (chronic lower respiratory diseases); J60-J64, J66-J70, J82, J92 (lung diseases due to external agents);
- treatable mortality– J00-J06, J30-J39 (upper respiratory infections); J12, J15, J16- J18 (pneumonia, not elsewhere classified or organism unspecified); J20-J22 (acute lower respiratory infections); J45-J47 (asthma and bronchiectasis); J80 (adult respiratory distress syndrome); J81 (pulmonary edema); J85, J86 (abscess of lung and mediastinum pyothorax); J90, J93, J94 (other pleural disorders); U07 (Coronavirus infection COVID-19). 9
Statistical analysis
The age-standardized mortality rates were obtained from the WHO’s comprehensive global health data. 6 Additionally, the corresponding 95% confidence intervals (95% CIs) were calculated for the age group of 0–74 years and by gender. This age group is used and individuals aged 75 years and over are excluded, following established methodological approaches by the OECD and the WHO, which is most amenable to medical and public health interventions. To calculate avoidable mortality, it sums the standardized mortality rate (tst) by age group, including the causes of death. The standardized death rate was calculated using the following formula:

where “n” is the number of age groups considered for adjustment;
Joint point regression (Joinpoint Regression Program 4.9.1.0 software), which calculates confidence intervals for estimated slopes and joinpoints using frequentist methods, was employed. It calculated the average annual percentage change (AAPC) and identified changes in the avoidable mortality rate between 2011 and 2021 for every age and sex group. 10 One breakpoint was identified, indicating a significant change in trend over the study period (2011–2021), mainly reflecting the sharp increase in mortality rates in 2020 due to the COVID-19 pandemic. Crude mortality rates were calculated per 100,000 population using a statistical trend function. Thus, it made it possible to calculate a linear trend line based on a given linear data set, where the predicted values of the year for the given values of the array number of deaths were applied. Before this, the regression model and the underlying assumptions of linear regression (linearity, independence, normality of residuals, and homoscedasticity) were checked. Statistical analyses were performed using Microsoft Excel due to its availability, ease of use, and widespread adoption, which allowed for efficient data processing and visualization without requiring specialized software.
Results
Crude mortality trends from respiratory diseases
The number of deaths from respiratory diseases fluctuated between 2011 and 2019, followed by a sharp increase to 13,864 per 100,000 people in 2020 and a subsequent decrease to 11,602 per 100,000 in 2021. The incidence was approximately twice as high among males as among females (Figure 1). Projections indicate that the mortality rate is expected to increase by 2026 for both genders over the next 5 years (Figure 1).
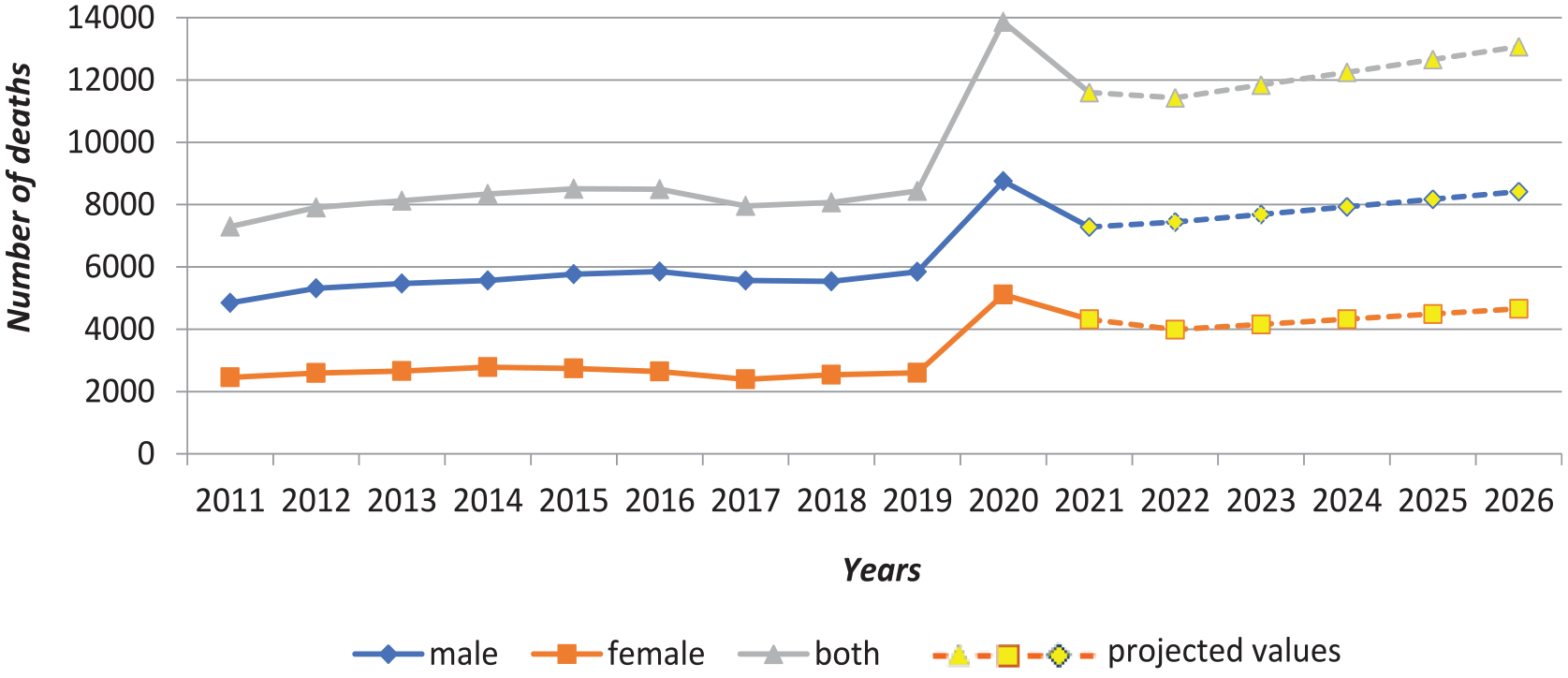
Mortality trends from respiratory diseases.
Avoidable mortality trends from respiratory diseases
From 2011 to 2019, the avoidable mortality from respiratory diseases per 100,000 people fluctuated between 65.94 and 65.15, with a peak of 80.56 in 2015. However, since 2019, avoidable mortality has more than doubled, reaching 156.19 per 100,000 people by 2021.
The preventable mortality rose from 43.45 to 56.42 between 2011 and 2014, then declined to 42.77 in 2019. For 2020–2021, it increased significantly to 92.98 per 100,000 people. Treatable mortality rates fluctuated between 22.49 and 20.51 from 2011 to 2019, followed by a threefold increase to 63.21 in 2021 (Table 1).
Avoidable mortality for respiratory disease.

The avoidable mortality (including preventable and treatable) for males was consistently three or more times higher than for females across all years within the investigation period.
AAPC increased by 7.5% (95% CI: 3.1; 12.2) between 2011 and 2021, with a higher increase observed among females (9.2% [95% CI: 4.8; 13.9]) compared to males (6.6% [95% CI: 0.9; 12.7]; Table 2). This shows that the mortality rate would have roughly doubled over the 10 years under the observed AAPC.
Average annual percentage changes of the avoidable mortality for respiratory disease.

A significant escalation in the AAPC was noted from 2015 to 2021, reaching 16.9% (95% CI: 8.4; 26.0), indicating a higher risk among females – 20.0% (95% CI: 11.6; 29.0) compared to males – 15.9% (95% CI: 4.9; 28.1).
The assumptions for the linear regression were carefully assessed, with particular attention to potential autocorrelation in the residuals, a common problem in time series data. No significant violations were found, confirming that the regression model’s assumptions were adequately met.
Discussion
The observed increase in mortality rates from respiratory diseases, especially from 2020 to 2021, coincides with the global COVID-19 pandemic. During this period, several problems emerged in the pulmonology service. There was a shortage of qualified medical personnel and insufficient hospital beds. 11 In addition, the development of intensive pulmonology and pulmonary rehabilitation was poor, and the distribution of various departments, such as pulmonology, thoracic surgery, phthisiology, and rehabilitation, was disorganized. This generally contributes to challenges in treating patients with severe respiratory diseases. 12
Although preventable and treatable mortality are defined separately, there is substantial overlap between them. Many deaths can be classified as either, indicating that the same risk factors and health system deficiencies are at play. This is necessary to better understand the interactions of factors that influence mortality and to develop integrated public health strategies.
Mortality rates and annual dynamics of mortality rates from chronic respiratory diseases vary significantly among 195 countries. 13 Data from the 2017 Global Burden of Disease Study show 14 that regions with higher sociodemographic indicators, such as better urbanization and health infrastructure, have lower respiratory mortality rates.15,16 Similarly, results from China 17 and Japan 18 point to the combined effects of respiratory infections and environmental exposures, which are also relevant for Kazakhstan. These studies suggest that early-life ecological exposures, including urban living conditions, can have long-term consequences for respiratory health, particularly in men.
Our study found persistent inequalities in respiratory mortality between the sexes, with men experiencing significantly higher mortality rates than women throughout the study period. This is consistent with existing research that links higher mortality among men to greater exposure to risk factors such as smoking, occupational risks, and poorer health behaviors. 19 Smoking, in particular, is a major contributor to respiratory disease and is more prevalent among men in Kazakhstan, further exacerbating gender differences in mortality. The estimated contribution of risk factors to mortality and disability-adjusted life years (DALYs) underscores the need for urgent action to mitigate these impacts.
A key finding of this study is the higher AAPC for women compared to men (9.2% vs 7.5%, respectively), particularly from 2015 to 2021, when the AAPC for women was notably higher at 20.0%. This increasing trend among women is concerning and may be due to several potential factors. Increasing exposure to air pollution and changes in socioeconomic and occupational roles may have led to greater exposure to respiratory risks among women. In urbanized regions with more prevalent industrialization and air pollution, women may face greater exposure to environmental pollutants, contributing to higher mortality rates. Underdiagnosis or improper treatment of respiratory diseases such as COPD or asthma can also worsen outcomes for women.
The study’s limitations include reliance on secondary data, which may suffer from cause-of-death bias or underreporting, particularly in regions with weak health information systems. Furthermore, the lack of stratification by socioeconomic status or ethnicity hinders our understanding of the underlying determinants of health outcomes. The study does not include sample size calculations specific to subgroup analysis because the study relied on data from the entire population. While this provides comprehensive coverage, it may limit the generalizability of the results to specific smaller subpopulations or rare conditions. Future studies should consider including sample size calculations to improve the robustness of subgroup analyses.
The study uses a comprehensive analysis of national mortality data, providing a broad overview of respiratory mortality trends across both sexes over a long period. Identifying key strengths, such as large-scale data and focusing on gender inequalities, provides a solid foundation for future public health research and interventions. However, addressing the identified limitations, such as more detailed data and a deeper understanding of occupational and gender factors, will be critical to advancing knowledge and designing more effective strategies to reduce respiratory mortality in Kazakhstan.
Our study did not directly analyze occupational factors; the known association between such activities and respiratory mortality provides an essential context for interpreting gender inequalities in respiratory mortality. In Kazakhstan, where men are predominantly employed in high-risk industries, the higher mortality rates among men observed in our study may be partly attributed to occupational hazards. This association calls for further analysis of the impact of occupational exposure on respiratory health in Kazakhstan, which may lead to more targeted public health interventions aimed at improving worker safety and reducing exposure to harmful substances.
In conclusion, the results highlight the urgent need for targeted public health interventions. Improving health literacy, promoting healthier lifestyles, and addressing air quality issues are vital to reducing the burden of respiratory diseases. Stricter tobacco control measures and policies aimed at reducing industrial pollution are important steps toward mitigating the impact of respiratory diseases in Kazakhstan. The study advocates for a multifaceted approach that involves collaboration among the government, healthcare providers, and the public to reduce mortality and enhance population health.
Conclusion
The study seeks to project the future prognosis of respiratory disease-related mortality and to highlight the need for targeted health strategies to reduce avoidable deaths through targeted health strategies. The avoidable mortality rate for males was consistently higher than that for females across all years of investigation. This study on avoidable mortality and crude mortality from respiratory diseases indicates an expected increase in the mortality rate by 2026. It highlights significant concerns and promotes scientific exploration.
Footnotes
Ethical considerations
The Local Ethics Committee approved the study (IRB00011496, protocol №3(126) from 30.03.2022) of Asfendiyarov Kazakh National Medical University, Almaty, Kazakhstan.
Consent for publication
Not applicable.
Author contributions
All authors substantively contributed to the data processing and writing. They agreed to be fully accountable for the integrity of all aspects of the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting this study are openly available from http://www.healthdata.org/gbd/data-visualizations and ![]()
This author takes responsibility for all aspects of the reliability and freedom from bias of the data presented and its discussed interpretation.