
Abstract
Keywords
Introduction
According to the World Health Organization, diabetes mellitus and depression are two chronic non-communicable diseases that are significantly linked to the health of people in the world. Diabetes also causes other morbidities, which may be involved in the decompensation of the disease, the appearance of complications and the possibility of increased health expenses due to hospitalizations and the management of complications.1,2 Worldwide, the prevalence of diabetes is 8.5%, according to the International Diabetes Federation 3 , while in Colombia, the incidence is 3.7 per 1000 people; in Santander, a department in the southeast of this country, the adjusted incidence is 8.41 per 1000 people.4–6
Depression, on the other hand, is the mental illness that occupies the fourth place in disease burden and is recognized as the leading global cause of mental disability, involving more than 300 million people globally. 7
The combination of these two pathologies generates complications in multiple aspects, and the joint presence of depression or depressive symptoms and diabetes is considered a reasonably complex comorbidity. 8 Although the two diseases are recognized separately, the fact is that the presence of depression in diabetic patients is underdiagnosed, and many of the complications present may be associated with the comorbidity of depression.
There are several factors possibly related to the presence of depression in diabetic patients. A study carried out in people with type 1 diabetes in Malaga, Spain, demonstrated a prevalence of depression of 27.1%. In this study, it was concluded that both quality of life (p = 0.001) and glycemic control measured by glycosylated hemoglobin (HbA1c) (p = 0.035) were significant variables. Likewise, it was found that the variables of being a woman, unemployed, smoking, having complications from diabetes and not having the perception of support from family, friends or colleagues were also associated with the risk of depression. 9
In this sense, considering the social support perceived by people with chronic non-communicable diseases (NCDs), such as diabetes, as a factor related to the comorbid presence of depression can have a significant impact on the quality of life and well-being of sick people. Social support can facilitate the process of adaptation to chronic illness by allowing patients to interact with other individuals.
According to Cassel and Cobb, social support has a significant impact on the maintenance of health by facilitating adaptive behaviors in stressful situations, 10 thus favoring the process of adjustment to chronic illness, recovery, and treatment adherence, as well as reducing the occurrence of mental conditions such as depression. Therefore, the absence of social support results in low treatment adherence and increases the frequency of complications and healthcare spending. 11
In the literature, Castro et al. 10 and Wheaton 12 two models can be found that explain the association between social support and health. The first model, “direct effect,” is where social support is considered an antecedent or simultaneous variable and maintains that social support favors health levels, regardless of the individual’s stress levels. 13 The second theoretical model, the “buffer effect,” conceptualizes social support as an intervening variable in the stress-illness relationship.13,14
According to this perspective, social support protects individuals from the adverse effects of stressful events and acts as a “mediating” variable in the relationship between stress and illness. This is achieved by allowing individuals to redefine the stressful situation and cope with it through non-stressful strategies, 14 as well as inhibiting psychopathological processes that could be triggered in the absence of social support, l preventing individuals from perceiving a situation as stressful, given that the certainty of having sufficient material and emotional resources can prevent said situation from being perceived as stressful, even if other individuals would define it as such.10,15
Social support is considered a multidimensional construct, according to several authors. Hilbert 16 defines social support as “the diversity of natural helping behaviors of which individuals are recipients in social interactions, tangible help, intimate interaction, guidance, feedback, and positive social interaction.” On the other hand, Cohen and Wills 13 have defined social support as the degree to which an individual perceives that they have access to people and resources that can help them in times of need. It is also considered a system of formal and informal relationships from which the person receives instrumental and emotional help to cope with stressful situations. 17 The perception of the social support received significantly corresponds with the responses and adaptation of people to assume the experience of caring more easily for themselves or others, reducing negative perceptions of this.18,19 Some authors have identified three significant dimensions of social support: social integration, perceived social support and provided social support. 10
It is essential to highlight that according to various studies,20–22 the perception of social support can be altered in cases in which people belong to a low socioeconomic stratum, which limits their ability to access health services and receive quick diagnoses. And timely, added to this situation are other derived barriers, such as the difficulty in obtaining medications, mobility and transportation to medical centers, and the lack of clear and precise information about the care and management of the disease.
A study conducted in Australia found that perceived social support was positively associated with quality of life in people with type 2 diabetes. 23 Another study on chronic obstructive pulmonary disease found that perceived social support was related to better treatment adherence. 24
The evidence in the literature has concluded that studies are required that allow us to know the relationship between social support and the presence of depression in diabetic patients to contribute to the generation of public policy that favors the care and quality of life of people who suffer from this condition. The study’s objective was to establish social support in diabetic patients recently diagnosed and its correlation with depressive symptoms.
Methods
Quantitative, analytical, cross-sectional, correlation-type approach study nested in a cohort of 173 recently diagnosed diabetic patients (<6 months) in the metropolitan area of Bucaramanga, Colombia.
The inclusion criteria were patients over 18 who attended the outpatient service of an institution providing first-level health services between July 2021 and May 2022, with a diagnosis of diabetes of no older than 6 months. Patients with a history of a depressive episode or antidepressant use expressed by self-report at the time of recruitment were excluded.
The Spanish version of the Social Support Inventory in Chronic Illnesses16,25 was used to evaluate social support. This instrument measures the perceived satisfaction with each support behavior; it has high validity and reliability indices of the Spanish version, Cronbach’s α of 0.95. 25 The instrument has 38 items and five subscales: personal interaction, guidance, feedback, tangible assistance, and positive social interaction. The guidance domain corresponds to all the help that the person receives through education and information; personal interaction is represented in emotional support, which refers to the favorable coping of the different situations of the chronic illness, while the feedback domain represents the feelings about who provides support, agreeing with said people and also those who support their thoughts and actions. All items are evaluated with a six-point Likert scale, from “dissatisfied” to “very satisfied.” The total score ranges from a possible range between 38 and 228.
The PHQ-9 questionnaire evaluates depression symptomatology. It is made up of the nine symptoms of criterion A of Major Depressive Episode (MDE) of the DSM-IV, arranged in the form of an adjectival-type scale evaluating the presence of the symptom in the last 2 weeks (“ nothing at all,” “several days,” “more than half of the days,” and “almost every day”), each of the questions is scored from 0 to 3, ranges of a minimum score of 0 and a maximum 27, and can be self- or hetero-administered.26–28 Interpretation can be made algorithmically to make a probable diagnosis of a Major Depression Episode or as a continuous measure of scores and cut-off points of 5, 10, 15, and 20, representing levels of depressive symptoms as mild, moderate, moderately severe, and severe. 29 This instrument has been validated in multiple studies,29,30 reporting Cronbach’s α coefficients of 0.894.
Results
Sociodemographic and diabetes characteristics in patients
The sociodemographic characteristics can be seen in Table 1. It is highlighted that 77.5% of the participants were women, 83.8% were single, the average age was 62.6 years (SD 12.3), and 46% of the people stratum two jurisdictions, 44.4% were homemakers. The average weight was 68.8 kg (SD 14.2), blood glucose 146.4 (SD 65.5), and glycosylated hemoglobin 7.6 (SD 1.7).
Sociodemographic Characteristics.

chi2 test.
t-Student test.
Mean (IC95%).*Statistical significance p < 0,05.
Perceived social support
The social support instrument presented perfect internal consistency. Cronbach’s α coefficient for the general scale of the social support instrument was 0.9859, Bartlett test Chi2 = 9193.65; p < 0.05 and a KMO = 0.97. In each participant, 38 questions were evaluated, of which ten (10) items measured the personal interaction dimension, fourteen (14) guide/information/instruction, five (5) feedback, five (5) social interaction and four (4) tangible help. 31 Moreover, according to the Shapiro-Wilk test, the total social support score presented a normal distribution (p > 0.05). The data analysis demonstrated that the 173 caregivers obtained a mean in social support 168.5, with a standard deviation (SD) of 37.4, a minimum score of 38 and a maximum of 228. The correlation between domains was statistically significant.
Likewise, as shown in Table 2, the domain with the highest patient score was guidance, followed by personal interaction and feedback.
Average total score by social support domains.

Source: Adapted from Results Delgado-Galeano M.2023.
Note. The table shows the perceived social support scores classified by domains. The guidance domain corresponds to all the help that the person receives through education and information; personal interaction is represented in emotional support, which refers to the favorable coping of the different situations of the chronic illness, while the feedback domain represents the feelings about who provides support, agreeing with said people and also those who support their thoughts and actions.
On the other hand, the lowest domains were tangible help, which represents material help in physical tasks and tasks that involve the performance of their different roles, and social interaction, which is the support with which it is intended to stimulate the recovery of relationships with others who can help to respond to their needs.
Regarding sex, it was determined that there was no statistically significant difference between men and women. However, women scored higher in all domains and the total social support score (Table 3).
Domains of social support by gender.

Source: Adapted from Results Delgado-Galeano M. 2023.
Note. The table shows the perceived social support scores classified by domains. The guidance domain corresponds to all the help that the person receives through education and information; personal interaction is represented in emotional support, which refers to the favorable coping of the different situations of the chronic illness, while the feedback domain represents the feelings about who provides support, agreeing with said people and also those who support their thoughts and actions. c: p<.05.
On the other hand, it was established that all social support domains are significantly correlated with each other. Furthermore, the very strongly correlated domain was mainly guidance with feedback. Similarly, the domains of guide with personal and social interaction and feedback with social interaction and tangible help showed a strong correlation (Correlation Coefficient 0.70–0.89) (Table 4).
Correlations between domains.

The correlation is significant at the 0.01 level (two-sided).
To evaluate the presence of positive symptoms of depression, the PHQ-9 questionnaire was used, and the total score obtained by each participant was grouped into a dichotomous variable according to the cut-off point established in the literature and considering the morbidity of the participants. The score selected for the dichotomous variable was >5 (Table 5). The PHQ9 total score was significantly associated with the domains of Personal Interaction and Guide but did not significantly correlate with the total social support score.
Distribution of the variables according to the presence of depressive symptoms according to the PHQ-9 score.
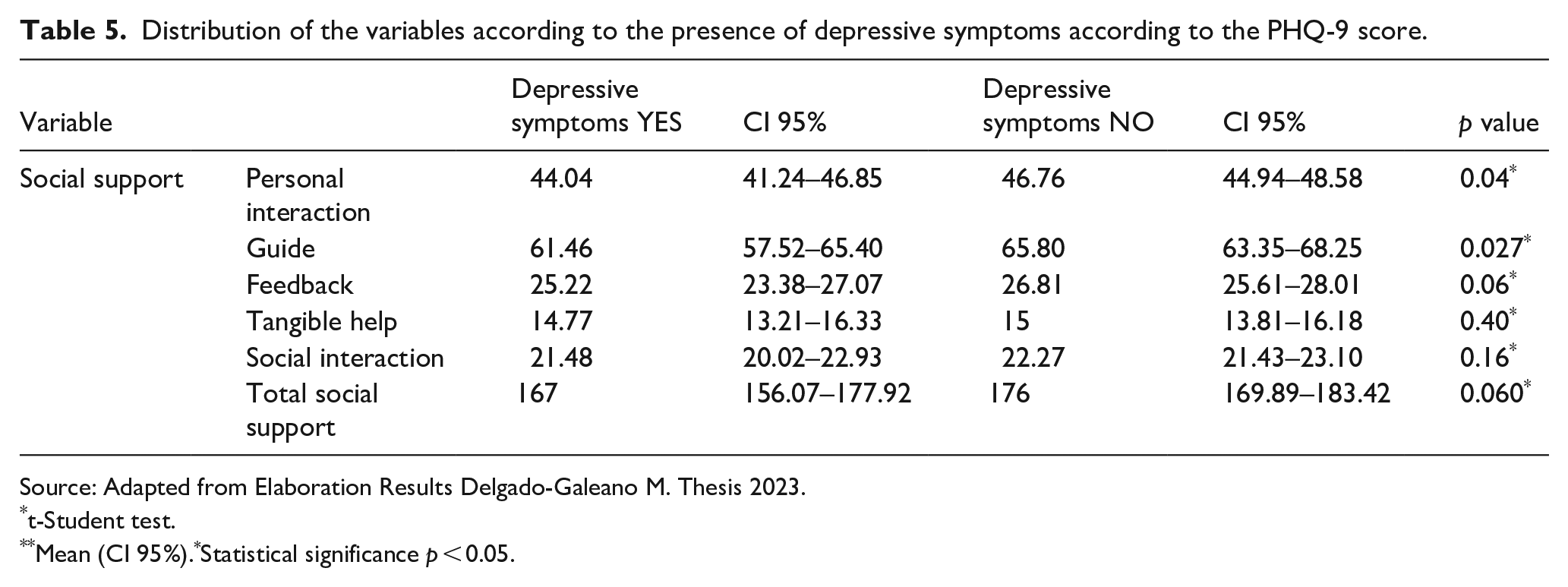
Source: Adapted from Elaboration Results Delgado-Galeano M. Thesis 2023.
t-Student test.
Mean (CI 95%).*Statistical significance p < 0.05.
Discussion
The objective of this study was to establish social support in diabetic patients recently diagnosed and its correlation with depressive symptoms. The findings allow us to see a correlation and that perceived social support is an essential factor that must be considered in the management and care of patients at the beginning of their diabetes diagnosis.
The relationship between perceived social support and the presence of depression in diabetic patients is a topic of great interest both in current scientific literature and for public health, given the high prevalence and persistent increase of diabetes in the world. Several studies have found evidence that perceived social support can significantly correlate with the onset and maintenance of depression in these patients.
Consistent with the findings of the present study, an inverse association between social support and depression in diabetic patients has been found in the literature, suggesting that those who perceive more excellent social support are less likely to present depressive symptoms.32–34
Diress Alen et al. 35 evaluated the relationship between perceived social support and the presence of depressive symptoms in type 2 diabetic patients. The results of these studies indicated that patients who reported a higher level of perceived social support presented a lower presence of depressive symptoms compared to those who said a lower level of perceived social support. The results of the meta-analysis conducted by Diress Alen et al. 35 showed that perceived social support had a significant mediating effect on the relationship between diabetes and depression, proposing that perceived social support may be a protective factor for depression in diabetic patients. These findings are consistent with the theory of the buffering effect of social support, which states that social support can reduce the adverse effects of stress and improve the adaptive capacity of individuals. 13
Social support can act as a protective factor against depression in diabetic patients, providing emotional and material resources to cope with the disease and its complications. Furthermore, social support can improve treatment adherence and quality of life of diabetic patients, which in turn can reduce the emotional burden of the disease and prevent the development of depressive symptoms.32–35
However, some studies have found that the relationship between perceived social support and depression in diabetic patients may be mediated by other factors, such as glycemic control and the presence of diabetic complications.35,36 That is, although social support can be beneficial for the mental health of diabetic patients, its effect can be modulated by other factors related to the disease.
In this context, although there is solid evidence suggesting that perceived social support may have a protective effect against depression in diabetic patients, more research is required to understand the exact nature of this relationship and to design effective interventions that promote social support and prevent depression in this population and at the same time address other risk factors for depression, such as glycemic control and the presence of diabetic complications. Such interventions may include strategies to strengthen patients’ social support networks, such as participation in support groups or intervention by health professionals to improve communication and the doctor-patient relationship22,37
The main limitation of the study was the sample size. However, when calculating the study’s power and significance of the study, it seemed that the study’s sample size allowed the relationship between social support and depression to be significantly identified. On the other hand, the study was conducted only in a population from a low socioeconomic stratum. Therefore, this variable was not considered for the evaluation. Despite these limitations, our study contributes to the existing knowledge on the association between diabetes and depression. It is recommended to include this socioeconomic variable in future studies to identify the impact of socioeconomic status on the association between social support and depression in diabetic patients at the time of their initial diagnosis.
Conclusions
Social support is essential to promote adherence to treating chronic non-communicable diseases. In the case of diabetes, it is necessary to consider the multidimensionality of this construct.
Social support interventions adapted to the contexts and settings in which users find themselves should be considered initiatives to strengthen the coping strategies of people with non-communicable chronic diseases.
Actions for people newly diagnosed with diabetes can focus on the dimensions of social support: guidance, information, and tangible help. In active coping, self-affirmation, distraction, and the dimension of information search in health professionals.
In conclusion, while the results of this study suggest that perceived social support may be an essential factor in the prevention and treatment of depression in diabetic patients, researchers and practioners alike are advised to exercise prudence when applying these findings to broader contexts.
It is desirable that health professionals consider the evaluation and strengthening of perceived social support as an effective strategy to improve the mental health of patients diagnosed with diabetes mellitus and, in this way, contribute to the minimization of depression as a comorbid condition in these patients. However, it is important to acknowledge the limitations of our research, particularly regarding the relatively small sample utilized in this study. Therefore, any generalizations drawn from these results should be made with caution. Future research that includes larger and more diverse samples would be beneficial to validate and extend these findings. It will be essential to gain a comprehensive understanding of this topic. Furthermore, diabetic patients may require social and care support if a new chronic disease is considered. Also, a comparative group of individuals with depression and diabetes, as well as those without depression, should be examined for future studies.
Footnotes
Acknowledgements
The research group acknowledges the ISABU for its cooperation and its lovely patients for enabling them to participate.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study had the ethics approval from the Universidad Industrial de Santander Committee (CEINCI-UIS). Number 4110. Act 6 of April 9, 2021; as well as the approval of the Ambulatory health facility (ISABU) June 10, 2021. All participants gave the informed consent before their participation.