
Abstract
Swasthya Rakshan Programme (SRP) provides health care services through Ayurveda, an initiative of the Government of India that aims to survey and create alertness of essential health appliances to ameliorate society from its grassroots level. The present study aimed to survey the prevailing health standards of residents in certain districts of India and to record the prevalence of diseases among them according to their living conditions, food habits, lifestyle, education, occupation and other socio-economic status. Data was collected through a community-based cross-sectional survey conducted from April 2018 to March 2019 in 22 Districts of 19 states in India. A stratified multi-stage sampling design was adopted for the survey. Documentation of demographic profile, food habits, lifestyle, hygiene status, and existing health conditions was assessed. A pre-designed semi-structured questionnaire was used for the collection of the data. Before initiating the programme, written consent was obtained. In this study, from 162 selected villages/colonies/areas, a total of 562,913 population and 81,651 households were surveyed. Sixty-nine thousand three hundred nineteen patients were cared for various ailments through health camps. The study found that the most prevalent disease in the concerned population was ‘Sandhivata’ (Osteo-arthritis), that is, 43.0%, followed by ‘Dourbalya’ (Debility), that is, 11.7%. The study includes insightful analyses of comprehensive demographic and health indicators classified by various socio-economic categories. The collected data regarding the prevalence of diseases with their sociodemographic correlations may provide a better understanding of the locality and thus may help in all future health endeavours.
Introduction
The science of Ayurveda is serving mankind through its novel healing approach to achieving complete health. Ayurveda’s Holistic approach still holds its strong position globally for primary healthcare needs.1,2 Being an over-densely inhabited nation, India has experienced a thespian-demographic transition in the past few years. Health affordability constraints, viz. confine in earnings, employment and assets, along with the limitations of financial shield offered for health expenditures in the Indian health system, are the critical challenges in the unprecedented burden of morbidity and mortality across the country. 3 Recognizing the need for scientific and reliable demographic information for strengthening healthcare delivery and improving health facilities, Swasthya Rakshan Programme (SRP) was an initiative of the Ministry of Ayush, Government of India, initiated in the year 2015.‘Swasth Bharat’ concerning ‘Sachh Bharat’ is the core project of the Ministry of Ayush, Govt. of India. Therefore, the purpose of SRP was also to educate the community about the importance of hygiene, cleanliness, sanitation and the Ayurvedic regime for preventing diseases, besides collecting vital statistical data of the selected locale through the scheduled health survey. The sociodemographic profile information related to dietary habits, lifestyle, and hygiene status were also documented during the study. Data about the nature and frequency of prevalent diseases were collected. Health awareness camps were conducted to expand health services. Door-to-door surveys were performed to build awareness among the general public about health and hygiene. Awareness about the cleanliness of household vicinity and environment, as well as propagation of knowledge for prevention of diseases, was also performed.
Methodology
Ethical consideration and method of data collection
A pre-designed semi-structured questionnaire was used for the collection of the data. Before initiating the programme, written consent was obtained from the local administrative authorities and the local people to participate in the programme, and the non-availability of health facilities, especially Ayurvedic dispensaries in the vicinity, was affirmed. The complete action plan for conducting the programme was presented before the local administrative authorities of the selected area concerning the aims and objectives of the programme to obtain consent. The team was trained to focus on the door-to-door survey for collecting demographic data, conducting health and sanitation/ hygiene awareness camps and providing health care services to people in need with subsequent follow-ups in those areas. During the SRP, a total of 4975 visits were made, and 411 educational institutes were covered in 162 villages/colonies/areas by 21 trained teams. Details are given in Figure 1.
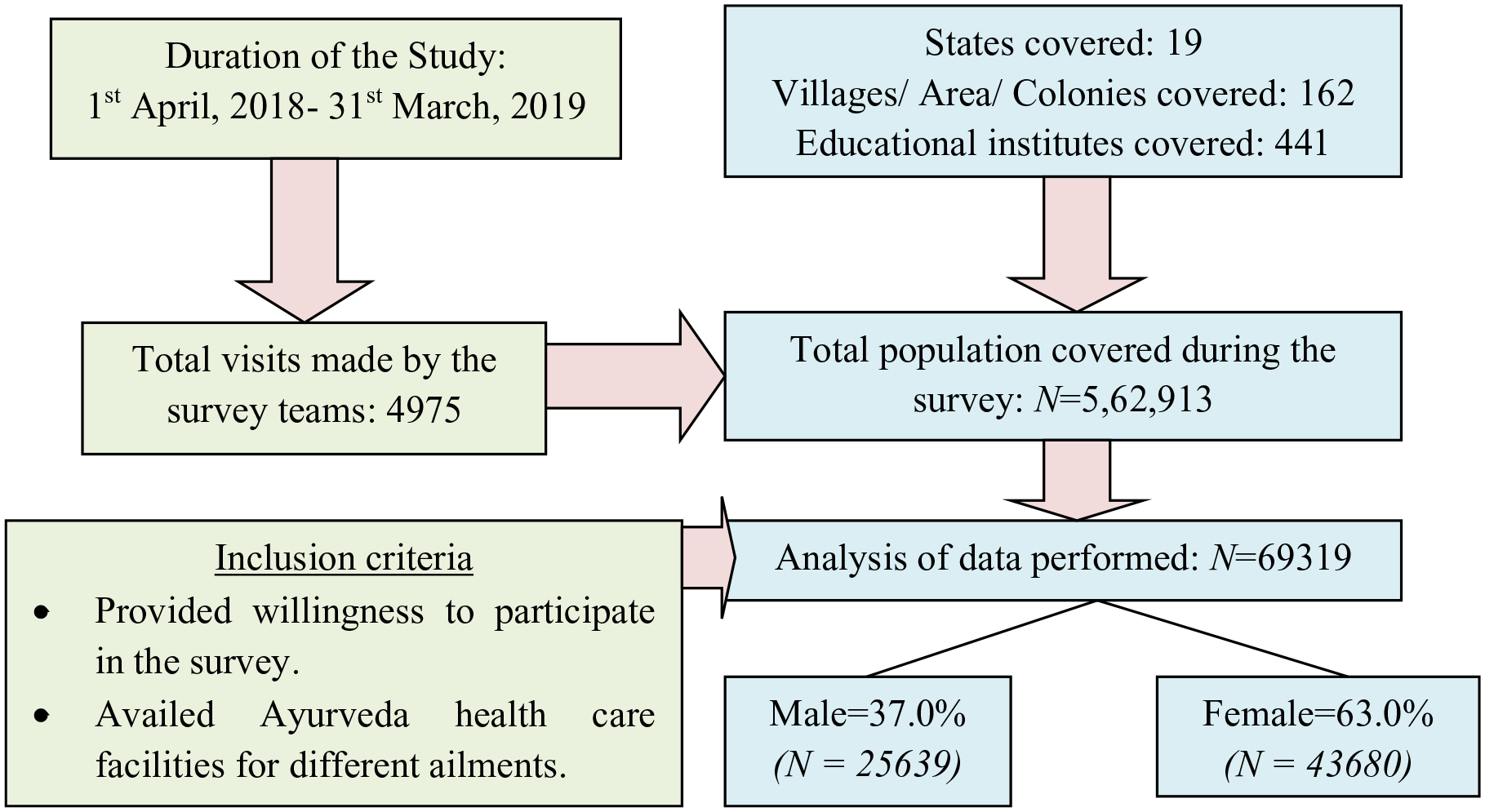
Flowchart of the participant’s recruitment process.
Observation and analysis
During the programme, a total of 562,913 people were surveyed, and 69,319 patients availed themselves of Ayurveda healthcare facilities for different ailments. Among them, 37.0% (N = 25,639) patients were males, and 63.0% (N = 43,680) were females. It was observed that a maximum of 81.1% (N = 56,248) patients were Hindus, followed by 8.0% (N = 5522) Muslims, and 4.9% (N = 3398) were Christians.
The cross-tabulation analysis of age with gender shows that 3.3% (N = 844) of male and 1.9% (N = 820) of female patients were aged Up to 5 years. 4.6% (N = 1192) of male and 302% (N = 1377) of female patients were aged 6–10 years (Figure 2).

Age with gender wise crosstabulation of patient.
Data shows that 18.6% (N = 12,871) of patients were educated at HSC and above, while 21.5% (N = 14,878) of patients were SSC. 16.9% (N = 11,723) of patients were in middle school education (Figure 3).

Education wise distribution of patient.
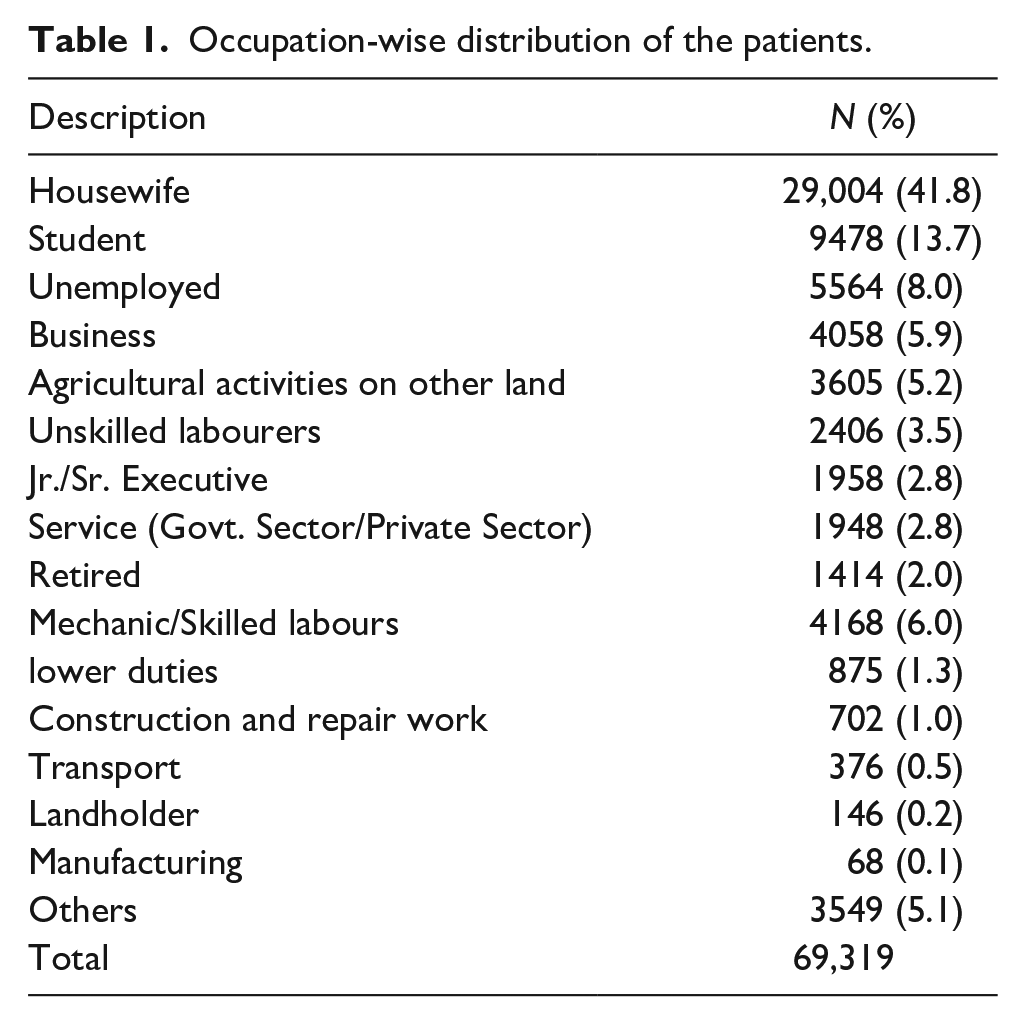
While analysing the occupation-wise distribution of patients, it was found that a maximum of 41.8% (N = 29,004) patients were housewives, followed by 13.7% (N = 9478) were students; 8.0% (N = 5564) were unemployed (Table 1). Analysis of income status indicates that 13.7% (N = 9469) were in the group of up to Rs 1000 income per month. 29.8% (N = 20,684) of patients were in the group of Rs 1000 to 2000 income per month, and 34.8% (N = 24,130) of patients were in the Rs 2000 to 5000 income per month (Figure 4).
Occupation-wise distribution of the patients.

Income wise distribution of patient.
Data on dietary habits revealed that 44.2% (N = 30,607) of patients were vegetarian.51.5% (N = 35,704) of patients were non-vegetarian (Figure 5). Cross tabulation of income with dietary choices/habits of patients showed that a maximum of 31.6% (N = 9665) of patients were vegetarian with Rs 2000 to 5000 monthly income. 34.4% (N = 13,728) of patients were non-vegetarian with Rs 2000 to 5000 monthly income (Table 2).

Dietary choices/habits wise distribution of patient.
Distribution of patients according to income per month and dietary choices/habits (preferential).
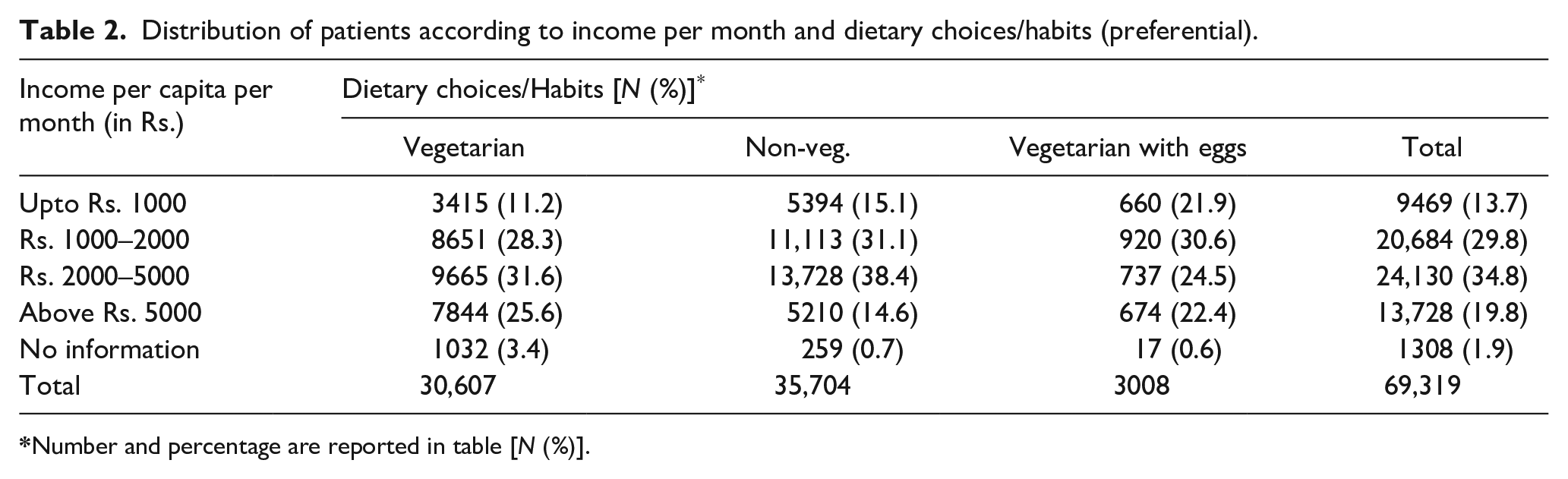
Number and percentage are reported in table [N (%)].
Food Choices/Habits-wise, the analysis of data shows that 47.2% (N = 32,688) preferred rice as their primary food, followed by 43.8% (N = 30,363) patients who preferred wheat (Table 3).
Food choices/habits wise distribution of patient.

Cross tabulation of income with food choices/habits of patients showed that 31.7% (N = 10,355) of patients who had Rs 1000 to 2000 of income per month preferred rice as their main food. Meanwhile, 40.8% (N = 12,397) of patients with Rs 2000 to 5000 monthly come from wheat as their primary food. 34.0% (N = 453) of patients who had above Rs 5000 of income per month preferred maize as their primary food (Table 4).
Distribution of patients according to income per month and food choices/habits (preferential).

Number and percentage are reported in table [N (%)].
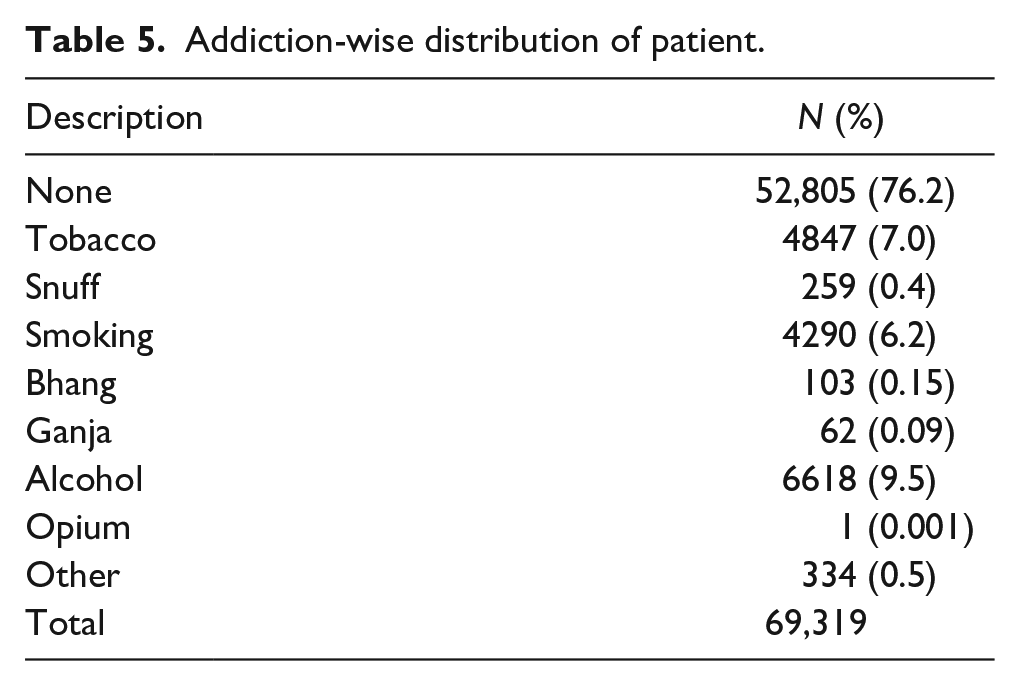
The study found that 76.2% (N = 52,805) of patients do not have any addiction. While 7.0% (N = 4847) patients were addicted to tobacco, and 6.2% (N = 4290) patients were addicted to smoking (Table 5). Cross tabulation of income with patients’ addictions showed that a maximum of 34.6% (N = 18,264) of patients who had Rs 2000 to 5000 of income per month were not addicted to anything (Table 6).
Addiction-wise distribution of patient.
Cross tabulation of Income per month with Addiction of Patient.
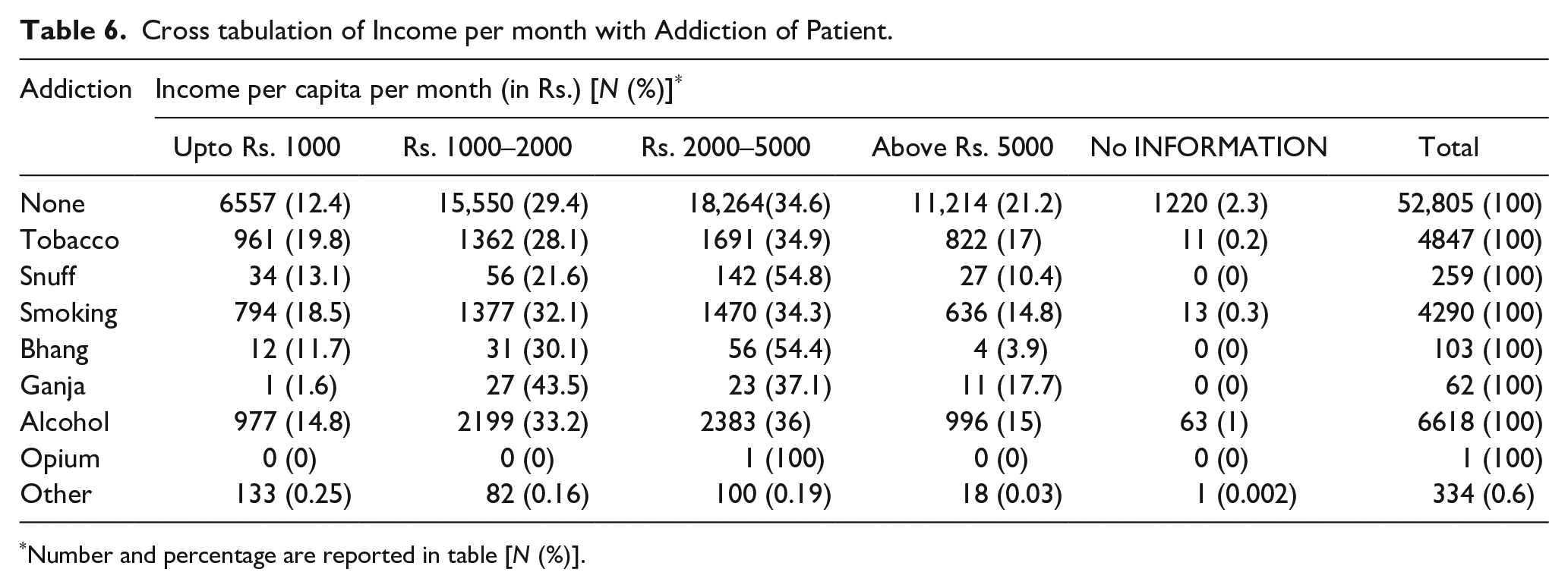
Number and percentage are reported in table [N (%)].
Disease-wise distribution of patient
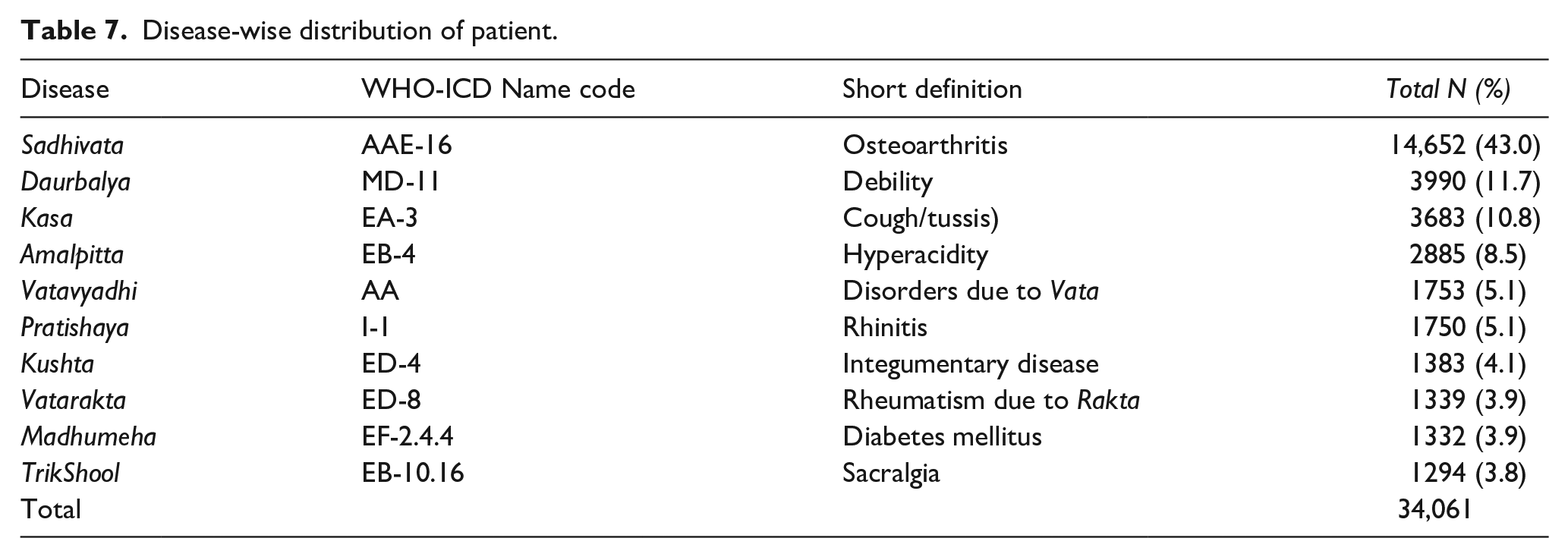
Various diseases were found in total patients who availed of Ayurveda treatment. Overall,73 types of different ailments were treated during the SRP; however, only the 10 most prevalent diseases were selected for the present analysis. A total of 34,061 patients were considered for the same. In the distribution, it was found that 43.0% (N = 14,652) patients had the disease Sadhivata (Osteo-arthritis); 11.7% (N = 3990) patients had the disease Daurbalya (Debility), while 3.9% (N = 1339) patients had disease Madhumeha (Diabetes mellitus) (Table 7).
Disease-wise distribution of patient.
Cross tabulation of diseases with gender of patient
Cross-tabulated data of the 10 most prevalent diseases and gender found in adults and children showed that 48.9% (N = 10,083) of patients with Sadhivata (Osteoarthritis) disease were prevalent in the adult females. 20.2% (N = 232) of patients with Daurbalya (Debility) disease were prevalent in female children. 43.9% (N = 565) of patients with Kasa (Cough/pertussis) disease was prevalent in male children. 11.1% (N = 1224) of patients with Amalpitta (Hyperacidity) disease were prevalent in adult females. 6.0% (N = 1244) of patients of Vatavyadhi (disorders due to Vata) disease were prevalent in adult females. 27.0% (N = 309) of patients with Pratishaya (Rhinitis) disease were prevalent in female children. 11.9% (N = 153) of Kushta (Integumentary disease) patients were prevalent in the male children group. 4.5% (N = 920) of patients of Vatarakta (Rheumatism due to Rakta) disease was prevalent in adult females. 6.0% (N = 656) of patients with Madhumeha (Diabetes mellitus) disease was prevalent in adult males. The remaining 4.9% (N = 1002) of patients with Trik Shool (Sacralgia) disease were dominant in adult females (Table 8).
Distribution of patients according to the 10 most prevalent diseases and gender found in adult & child.

Discussion
The present era’s major health concerns are the sedentary lifestyle, unhealthy food habits, poor nutrition, and improper hygiene conditions. In recent times, the world has gradually been attracted to the holistic approach of Ayurveda as it deals with preventing and managing lifestyle disorders.4,5 Therefore, the SRP was planned to reach the public, create health awareness, and prevent diseases through correct edification and appropriate intrusion in the course of Ayurveda. Turning out of a large number of patients in Ayurveda Health Camps and awareness programmes during the study reflected people’s faith in traditional medicines. Survey Data regarding literacy and accountability shows that the population (21.46%) have education up to the 10th level, and only 18.56% have higher school or technical education (Figure 3). Therefore, educating the populace about preventive health must be meticulously monitored and appraised. The source of the communiqué would be reasonably good for the concerned population for further clarity and feedback, as the data shows that 87.02% of the population are mobile phone users. The analysed data revealed that the most prevalent disease in the concerned population was ‘Sandhivata’ (Osteo-arthritis) followed by ‘Dourbalya’ (Debility) and ‘Kasa’ (Cough). The least prevalent disease was Grahani dosha (IBS). As per age group distribution, the maximum number of patients belongedtothe age group of 36–45 years, followed by the age group of 46–65. In the case of gender, females were more sufferers than males. In the surveyed area, affected people belonged to the middle age group, followed by the old-age group. This may be due to faulty lifestyles and dietary habits. The highest prevalence of such diseases was found in middle age group. The old age (above 60 years) is Vata Prakopa Kala (aggravation of Vata) and the beginning of the ageing process and degenerative changes. This leads to Kshaya (Depletion) of Shareera bala (physical strengths) and all the Dhatu, resulting in Vata Prakopa (aggravation of Vata). Thus, the prevalence of Sandhivata and Vatavyadhi enhanced in this senile age group as aggravated Vata acts as a discriminatory factor.6,7
The marital status-wise distribution shows that most patients were married. Still, it cannot be concluded that married persons are more prone to these diseases since, in this survey, most patients were above 18 years, which is the usual age for marriage. This area’s educational status shows that most patients had a primary level of education followed by a high school education level. These observations point out that education is indispensable for achieving a healthy life as education boosts wakefulness on healthy lifestyles, and the population with less education generally does not have the knowledge of maintaining sound health.8 –11 The report indicates that most patients were non-vegetarian and preferred rice, followed by wheat and pulses. Recent studies have also found a positive association between the intake of white rice and type 2 diabetes.10,11 In this survey, 2.56% of patients were known cases of type-2 diabetes.
The knowledge regarding the prevention of disease and promotion of health through the knowledge of Dinacharya (Daily regimen), Ritucharya (Seasonal regimen), and Sadvritta (Code and conduct) was given during the survey. Maximum patients were not addicted to any addiction, but some were addicted to tobacco, alcohol and smoking. The data was analysed to find the food habits, addiction, and diet habits concerning monthly income per capita, which measures the stability and wealth within an economy.12,13The data shows the maximum number of people with income per capita per month between 2000 and 5000, and the leading cases of addiction were also more in this salary group.
Reports concerning the disease’s aetiology indicate that lifestyle disorders contribute to most of the disease load. The grounds for these findings might be that more than half of the patients were housewives. In this modern era, excessive consumption of faulty dietary habits, faulty lifestyle, as well as unremitting stress plays a significant role in the causation of lifestyle disorders.14 –18 Furthermore, direct communication from published research reveals that their lifestyles regarding food intake, sleep and exercise are ridiculous.19,20Also, most of the patients were habituated to day sleep. The documented data on the percentage of relief from the symptoms reveal that more than 90% of patients were relieved by the treatment during the programme. The lab investigation viz. Hb assessment, ESR estimation, blood sugar analysis and urology were also performed. These parameters revealed the primary health status and helped to rule out the presence of certain common flaws. Socio-economic status and hygiene were also included in the survey because living conditions are directly related to health.21 –24 Underprivileged housing conditions are allied with different health circumstances, including respiratory infections, asthma, lead poisoning, injuries, and mental health.25 –27 Therefore, these parameters were also included in the SRP plan. Through SRP, researchers were directly able to convey certain elementary health issues, relevant health awareness tips, and practical preventive aspects of sanitation and hygiene. The importance of the Ayurveda Pathya-Apathya model was also conveyed to the concerned participants.2,28,29,30 This might help them get the appropriate health care at the needed time.
Conclusion
The report indicates that Ayurvedic therapies responded well to the most prevalent diseases. Through SRP, team members could convey certain essential health-related aspects, relevant health awareness tips, and practical preventive aspects based on sanitation and hygiene. The collected data regarding the prevalence of diseases with their sociodemographic correlations may provide a better understanding of the locality and thus may help in all future health endeavours.
Limitations and recommendations
There are various limitations to this present study that must be addressed. The present study was conducted under SRP, a health programme initiated by Govt. of India. For analysis, simple measures like frequency and percentage were used. Descriptive analyses were done as frequencies and percentages for demographic characteristics and other key variables. No statistical test was performed on the key categorical variables to determine their association. Therefore, we recommend a properly planned study with a viable design and statistical approach.
Supplemental Material
sj-docx-1-phj-10.1177_22799036241243272 – Supplemental material for Health and demographic indicators of selected districts of India: An impact of Swasthya Rakshan Programme (SRP)
Supplemental material, sj-docx-1-phj-10.1177_22799036241243272 for Health and demographic indicators of selected districts of India: An impact of Swasthya Rakshan Programme (SRP) by Vipin Kumar Sharma, Bidhan Mahajon, Avinash Kumar Jain, Renu Singh, Rakesh Rana, Pratap Makhija, Narayanam Srikanth and Kartar Singh Dhiman in Journal of Public Health Research
Footnotes
Acknowledgements
The authors are highly thankful to all the team members in different States for their sincere efforts in successfully implementing the programme, collecting data, and providing health care services.
Author’s contributions
VKS—Proposal writing and survey construction; BM—Manuscript writing and data analysis; RR—Statistical analysis; RS, AKJ, PM—Manuscript review and data analysis; NS, KSD—Proposal writing, Manuscript review, Study conception and Over all monitoring and guidance of the whole programme.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Central Council for Research in Ayurvedic Sciences, Ministry of Ayush, under outreach activities.
Significance for public health
The present study aims to survey the demographic and health indicators of certain districts of India and to provide basic health care services through Ayurveda under Swasthya Rakshan Programme (SRP) which is an initiative of the Government of India that aims to survey and create alertness of essential health appliances to ameliorate society from its grass root level. Data of the prevailing health practices of residents, the predominance of diseases amongst them according to their living conditions, lifestyle, food habits, education, occupation and other socioeconomic status were analysed. In this study, from 162 selected villages/colonies/areas, a total of 562,913 population and 81,651 households were surveyed. The collected data regarding the prevalence of diseases with their socio-demographic correlations may provide a better understanding of the locality and thus may help in all future health endeavours.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.