
Abstract
Background:
DSM-5 separates bipolar (BD) from depressive disorders, but some experts consider BD as part of a spectrum of mood disorders. The interpretation of numerous false positives of BD screened by the Mood Disorders Questionnaire (MDQ) is part of this debate. Recent study results suggest that the worsening of health-related quality of life (H-Qol) associated with MDQ positivity does not depend solely on mood disorders. This study aims to clarify whether the impairment may be due to other concomitant disorders, unrelated to mood disorders, leading to a worsening of H-Qol. Additionally, the study aims to explore if MDQ positivity itself observe clinical significance.
Design and methods:
The study involved pairs of cases (MDQ+) and controls (MDQ−) matched for sex, age, and absence of DSM-IV psychiatric comorbidity. The impact of MDQ positivity on the quality of life in a sample of MDQ+ comorbid with MDD was measured and compared to impact of MDD in other chronic disorders.
Results:
The H-Qol was significantly worse in MDQ+ than in controls (both groups without any psychiatric co-morbidity). The worsening was similar to severe chronic disorders The burden of worsening quality of life due to MDD was mild in another sample of MDQ positives with comorbid MDD.
Conclusion:
The study hypothesizes that MDQ positivity may be related to hyperactivation and dysregulation of rhythms typical of stress disorders. In fact, MDQ+ was found strongly related to sleep disturbances. Future studies could verify if a “Dysregulation of Mood, Energy, and Social Rhythms Syndrome” (DYMERS), causes worsening the H-Qol in MDQ+.
Introduction
The last classification of the American Psychiatric Association, DSM-5, has restricted the field of bipolar disorders by separating them from depressive disorders. 1 This classification contrasts with the neo-Kraepelinian concept of a spectrum of mood disorders that includes both bipolar disorders (as more severe forms) and depressive disorders. The characterizing element of the spectrum is mania and hypomania, which, even with subthreshold manifestations, would have preceded depressive episodes often misdiagnosed as major depression. This arguing view of bipolar disorder characterized the debate following the discovery of the low accuracy of the bipolar disorder screener paper and pencil tests. 2 Indeed, some tools, particularly the Mood Disorder Questionnaire (MDQ), were found to identify a greater number of false positives compared to diagnoses of Bipolar Disorder conducted in clinical settings.3,4 The low specificity was attributed to false identification, as episodes of hypomania were confounded with non-specific episodes of hyperstimulation observed in various other disorders (e.g. personality disorders, posttraumatic stress disorder, anxiety disorders, alcohol and drug use disorders, impulse control disorder, eating disorders, and attention deficit disorder). These hyperstimulation episodes were prevalent among MDQ positives even in the absence of a concurrent diagnosis of BD. 5
This interpretation has generated several concerns among neo-Kraepelinian supporters. This is because the disorders observed among the false positives are well-established to have a strong association with bipolar disorder,6,7 a condition that typically manifests years before anxiety and personality disorders.7,8
If the neo-Kraepelinian perspective is accurate, the clinical consequences and impact on the quality of life related to MDQ positivity should resemble those of a “sub-threshold” disorder. Consequently, there would likely be a significant impact, even if not equivalent to that of a “full” disorder. Additionally, the impairment in quality of life would be exacerbated by the coexistence of a Major Depressive Disorder (MDD) diagnosis. As a similar condition could represent an undiagnosed “full” Bipolar II Disorder, which considerably impairs health-related quality of life. 9 Consistent with the existing literature, it is also expected that cases of unrecognized bipolar disorder or the “conversion” of subthreshold Bipolar Disorder into “unrecognized full Bipolar Disorder” (i.e. MDQ positivity plus Major Depressive Disorder MDD) would occur at a later age compared to individuals with only MDQ positivity without full mood disorders. According to this hypothesis, the onset of a depressive episode and diagnosis of MDD would precede the onset of manic episodes (detected through MDQ positivity). 10
On the other hand, if the “malaise” captured by MDQ positivity were the result of an association with frequent diagnoses of non-bipolar psychiatric disorders resulting in “false positives,” the impairment in health-related quality of life associated with MDQ positivity would be attributed to the concomitant non-bipolar disorders. However, recent research evidence challenges this assumption. 11
A direct link between genetic risk of bipolar disorder and MDQ scores has not been found. However, the genetics of bipolar disorder are intricate and involve multiple interactive risk factors. The absence of a direct linear relationship between genetic risk and MDQ scores does not eliminate the possibility of an association, particularly when genetic factors interact with other co-factors. Some traits of bipolar disorder, such as hyperactivity, can manifest themselves in individuals without the disorder under specific circumstances. While the presence of the “at-risk variant” in non-at-risk individuals does not rule out a potential relationship with bipolar disorder, it certainly defies a simple linear correlation. Overall, the study underscores the intricate interplay of genetic and environmental factors in bipolar disorder and related conditions, challenging straightforward diagnostic correlations and emphasizing the need for comprehensive understanding.
The purpose of this study is to investigate the clinical burden associated with MDQ positivity in terms of its impact on health-related quality of life in individuals without other psychiatric diagnoses. The hypothesis posits that if the MDQ identifies a clinically relevant and disabling condition on its own, the attributable burden will be higher. Additionally, the study aims to assess the extent to which the burden on health-related quality of life worsens in cases of comorbidity between a lifetime diagnosis of Major Depressive Disorder (MDD) and MDQ positivity.
Design and methods
Design
This is a case-control study on a database of a previous community survey. The results are then compared with similar results drawn from the same database for cases and controls or with case-control studies of non-psychiatric conditions whose controls were drawn from the same national database.
Study sample
The database of the community survey, from which was drawn the study sample, was selected after stratification by age and sex from the adult population records of urban and rural municipalities of six different Italian regions (balanced by geographical distribution and average income compared to the total of the 20 Italian regions). A detailed description of the community survey and of the 4999 selected individuals was already published. 12 For the purpose of this study we selected all individuals scoring positive on the MDQ (cases), and we excluded all the individuals who had in association a diagnosis of a psychiatric disorder. For each MDQ-positive individual selected, all MDQ-negative individuals of the same age and gender and without psychiatric DSM-IV co-morbidity. The exclusion criteria for the control sample was also to have an MDQ score of 6 or 7. For each MDQ-positive a block with all eligible controls was built and a control for each block (each case). was randomly drawn.
Study instruments
The data selected for the study refer to the following instruments: Ad-hoc form for assessing basic demographic variables; “The Advanced Neuropsychiatric Tools and Assessment Schedule” (ANTAS), 13 a previously validated semi-structured clinical interview allowing, if administered by clinical expert interview, psychiatric diagnosis according to the DSM-IVR diagnostic system; The Mood Disorder Questionnaire (MDQ) in the Italian version 14 was used, during the national survey with the purpose to assess lifetime hypomanic episodes or episodes of augmentation of energy, 15 however, the present study hypothesizes that positivity of MDQ can identify a dysregulation syndrome; The Health Survey Short Form 12 item (SF−12) was used to assess the health-related quality of life according to different dimensions such as physical health and functioning, physical pain, vitality, social functioning, emotional condition, and psychosocial disability. 16 The assessment period is 1 month. The higher the score on the SF-12, the better is the perception of the health-related quality of life.
Ethics
The protocol of the late National community survey was evaluated and approved by the ethical committee of the Italian National Health Institute (Rome). 12 The possibility of conducting case-control studies on the database to investigate subsequent hypotheses was foreseen in the approved protocol. Informed consent was signed by each candidate.
Statistics
The comparison between the means and standard deviations of the total scores of SF-12 in cases and controls was carried out by means of ANOVA 1 way. As mentioned in previously published articles,17,18 the “Attributable Burden in Worsening QoL” of a given condition (in this case MDQ+) is the difference between the mean and standard deviation of a SF-12 control sample without the condition and the score of an age- and sex-matched sample with that given disorder . In this case we carried out a comparison of “Attributable Burden in Worsening QoL” of the MDQ positives with a series of impairing health and mental health condition conducted in studies on psychiatric conditions that had drawn their cases and controls from the same data and in studies on non-psychiatric condition that used the same database for controls.17,18
Results
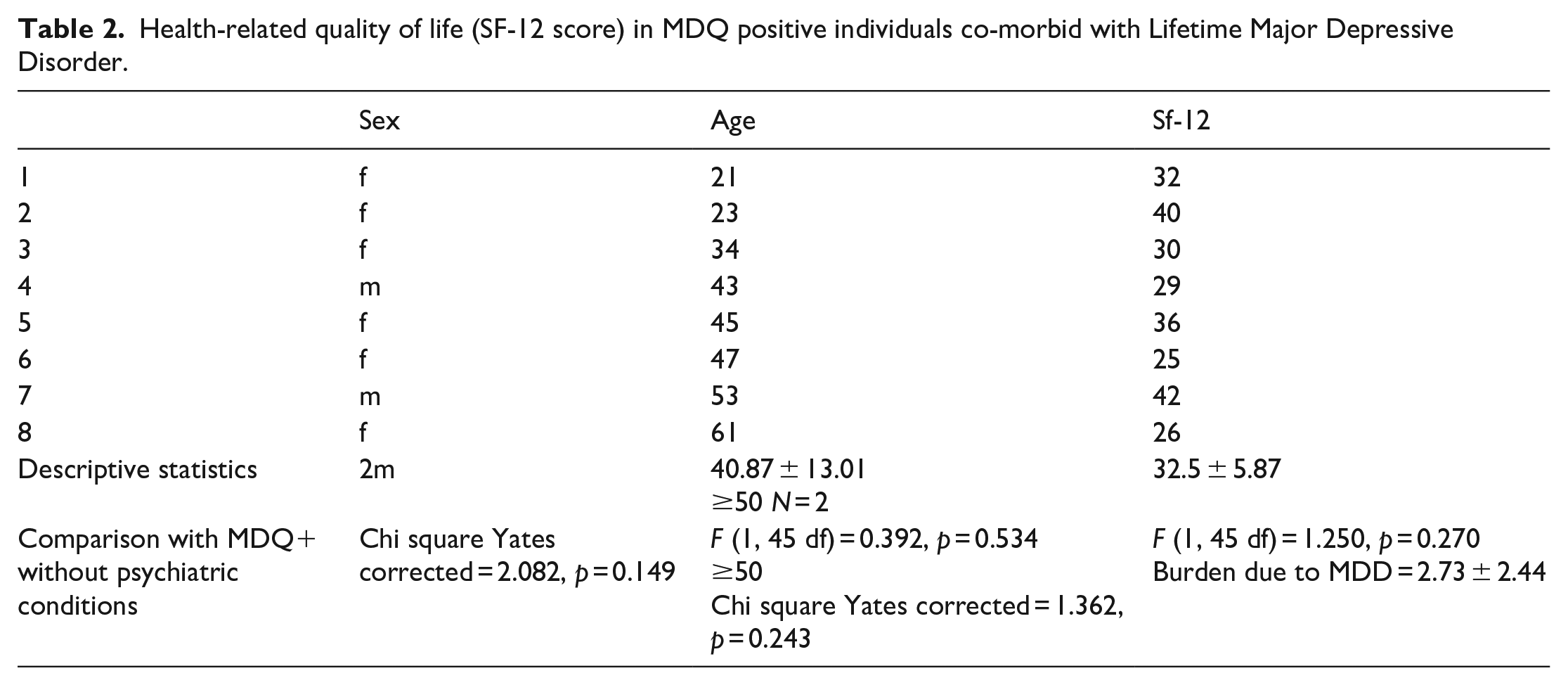
The study sample includes 38 pairs of cases (MDQ+) and controls (MDQ−) matched for sex (23 males), age (44.26 ± 14.08), both groups did not have DSM-IV psychiatric comorbidity diagnoses. The total score on the SF-12 scale, measuring the health-related quality of life, was higher in controls [41.65 ± 3.39vs 35.23 ± 6.35, F (1, 75 df) = 30.337, p < 0.0001]. The mean of SF-12 overall score in MDQ positives without concomitant other psychiatric conditions was similar to that of chronic mental health and non-mental health diseases (Table 1) as Wilson’s Disease, 19 Carotid Atherosclerosis, 20 Major Depressive Disorder, 21 Eating Disorders, 15 Obsessive Compulsive Disorder, 22 Post-Traumatic Stress Disorder, 23 Agoraphobia, 24 Solid Tumor, 25 and Onco-hematological tumors. 26 The perception of the health-related quality of life in MDQ positives without any psychiatric disorder was even worse than that observed in Celiac Disease, 17 Panic Disorders, 27 and Simple Phobia. 28 Only Multiple Sclerosis 18 and Fibromyalgia 29 were associated with a worse health-related quality of life than the MDQ positive condition free of other psychiatric disorders. Table 2 shows the demographic characteristics and the health-related quality of life (as a score of SF-12) in the eight individuals found in the database reporting MDQ positives with comorbidity with Lifetime Major Depressive Disorder. In this sample, there is a higher frequency of women than in the sample of people with MDQ positivity without diagnosis (75%vs 39.5%) and younger age (40.87 ± 13.01vs 44.26 ± 14.08; ≥50 25% vs 44.7%), however, as shown in the Table 2, the differences in all these values do not reach any statistical significance. The difference in the SF-12 score is worse in the group with concomitant diagnosis of MDD of a mean of 2.73 ± 2.44 points in the score (this measure is the attributable burden due to MDD), however even in this case, the difference between the two samples does not reach statistical significance. Table 3 shows the attributable Burden to Major Depressive Disorder in MDQ positives (as the difference in the score of health-related quality of life scale SF-12 in people with MDQ positivity without MDD and in people with MDQ positivity and MDD) and the comparison with similar measures carried out in studies using the same database for psychiatric chronic disease or case-control studies in non-psychiatric chronic disorders using the same database for the choice of controls. The impact of MDD in worsening the health-related quality of life of people with MDQ positivity tends to be the lowest compared to impact of MDD in the chronic disorders considered, however, no statistically significant differences are found except with solid tumors where the impact of comorbidity with MDD is much more impacting on the quality of life.
Health-related quality of life (SF-12 score) in people MDQ positives without diagnosis with other psychiatric conditions in comparison with Health-related quality of life in other chronic diseases.

Health-related quality of life (SF-12 score) in MDQ positive individuals co-morbid with Lifetime Major Depressive Disorder.
Attributable Burden to Major Depressive Disorder in MDQ positives and comparison with other psychiatric and non-psychiatric chronic disorders.

Discussion
The study shows that individuals living in the community who test positive for the MDQ screening test, even in the absence of any psychiatric diagnosis, exhibit a significantly lower health-related quality of life compared to a sample of the general population with the same age and gender but negative for the MDQ. The impact of MDQ positivity (in the absence of other disorders) on worsening the quality of life was surprisingly similar to the impact seen with similar methodology and data from the same database for severe chronic disorders and diseases.19–27 Only Multiple Sclerosis 18 and Fibromyalgia 29 were found to have more impact on health-related quality of life than MDQ positivity even with comorbid psychiatric disorders.
This data supports the hypothesis that MDQ positivity, by itself, identifies a condition of clinical interest regardless of comorbidity with other disorders. The dimensions explored by the SF-12 (albeit from a subjective perspective) include physical health and functioning, physical pain, vitality, social functioning, emotional condition, and psychosocial disability. Therefore, these elements are not negligible on a clinical level.
Another pertinent aspect is the mean difference in SF-12 score between individuals with co-morbid MDD and positive MDQ (Mood Disorder Questionnaire) and those with positive MDQ without concomitant MDD (“attributable burden due to MDD”). This difference is not greater than that observed in most chronic psychiatric or non-psychiatric disorders when calculating the attributable burden of MDD for these conditions. Only in solid tumors is there a greater impact (“attributable burden”) of MDD on the quality of life.
It should be considered that if we accept the hypothesis that the MDQ identifies hypomania episodes, individuals diagnosed with MDD and positive MDQ could represent unrecognized cases of bipolar II disorder. The literature shows that bipolar II disorder severely compromises the quality of life even to a greater extent than bipolar I disorder. 9
Additionally, according to the literature, 10 we would expect the presence of MDD to be more common in adult/older individuals, while the trend is reversed.
However, new research evidence may suggest a new interpretation of clinical means of MDQ false positives. A recent study has determined that based on genetic profiling, MDQ “false positives” were closely associated with anxiety disorders and PTSD genetic determinants, and that there wasn’t a linear correlation between the genetic risk of bipolar disorder and the MDQ score. 30 The same research also demonstrated a close association between MDQ positivity and insomnia. 30
However, the genetics of bipolar disorder are complex, and the concomitance of different interactive genetic risk factors cannot be excluded. 31 The absence of a linear relationship cannot exclude an association that could exist but be mild if this genetic factor interacts with concomitant co-factors. In fact, some elements, such as the attitude of hyperactivity, typical of bipolar disorder, can be found in people who do not suffer from this disorder in specific conditions of conflict or social danger, 32 and a high frequency of a genetic variant (the allele RS1006737 of the CACNA1C gene considered a risk factor for bipolar disorder) was found in elderly people with hyperactivity/novelty-seeking traits but who are perfectly socially integrated and without any psychiatric diagnosis.33–35
In this framework, even admitting that the presence of the “at-risk variant” may be found also in the not-at-risk subgroup, this cannot cancel a possible BD-genetic variant association relationship but certainly cannot justify a linear correlation. An indirect confirmation of a possible interaction between other risk factors than the genetic variant RS1006737 of the CACNA1C gene comes from a study that had to compare the score of MDQ and the presence of the above-cited genetic variant as screeners of BD, against a diagnosis of bipolar disorder carried out by clinicians as the Gold Standard. 36
Both screeners exhibited a certain accuracy against the Gold Standard, albeit insufficient for practical use (excellent specificity for the MDQ, good sensitivity for gene testing). However, the unexpected and apparently contradictory finding was that the two screeners showed very low reliability between them, measured independently of the Gold Standard. 36
Considering the close association of sleep disturbances with MDQ positivity, 30 it was hypothesized that the hyperactivation identified by the MDQ could be related not only to a manic/hypomanic episode but also to the hyperactivation typical of certain stress disorders known to be linked to sleep disorders. 37 A similar hypothesis made the phenomenon of moderate accuracy of the MDQ and gene test plausible (which, we reiterate, was identified even in healthy hyper-exploratory elderly individuals) regarding bipolar disorder, as well as the low reliability between the two tests (MDQ and gene). In other words, if the activation identified by the MDQ was a trigger (not exclusive to BD) and gene positivity a predisposition (non-pathogenic in itself), a similar hypothesis made plausible the phenomenon of moderate accuracy for both the MDQ and the gene test in diagnosing bipolar disorder, along with low reliability between the two tests (as if the MDQ and gene could identify two different components).
On the other hand, a subsequent study demonstrated that the presence of MDQ positivity significantly worsened the quality of life, regardless of the presence of a bipolar episode or comorbidity with a bipolar diagnosis. This was evident by comparing the scores on the SF-12 scale of health-related quality of life from a sample of positive MDQs from a database of the general population (excluding those with comorbidity for bipolar disorder) and a sample matched by gender, age, and the co-presence of psychiatric disorders other than mood disorders. Furthermore, the difference between the two samples remained substantial even after the age of 50, when a late diagnosis of bipolar disorder became increasingly unlikely, thus reducing the risk of false negatives.
Considering the clinical consistency of the condition (i.e. the significant deterioration in associated quality of life), the co-occurrence of sleep disturbances, and the possibility that the hyperactivation investigated by the questionnaire could potentially identify not only manic episodes but also stress-induced hyperactivation, the “heuristic” hypothesis emerged that MDQ positivity could identify a “Dysregulation of Mood, Energy, and Social Rhythms Syndrome” (DYMERS). This syndrome appears to play a crucial role in the worsening of chronic conditions and represents a specific picture related to stress, as well as the relevance of social rhythms in stress prevention. Discussions have started concerning stress during the Covid pandemic and specifically during the lockdown periods.38–40
In conclusion, the results suggest the hypothesis that the positivity of the MDQ may have captured a hyperactivity syndrome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was carried out as part of the resource-funded research project: P.O.R. SARDEGNA F.S.E. 2014-2020 - Asse III “Istruzione e Formazione, Obiettivo Tematico: 10, Obiettivo Specifico: 10.5, Azione dell’accordo di Partenariato:10.5.12 “Avviso di chiamata per il finanziamento di Progetti di ricerca – Anno 2017, and Fondazione di Sardegna, Italy.