
Abstract
Subarachnoid hemorrhage is a neurological emergency in which arterial blood accumulates in the subarachnoid space with cerebral aneurysmal rupture being the most common cause. Subarachnoid hemorrhage is often misdiagnosed in the emergency department and mortality rates range from 8% to 67%. It may be the manifestation of the chronicity of the migraine. The difference in severity or quality compared to previous headaches, and other symptoms, particularly neck stiffness, but also seizure, syncope, focal neurological deficit, and vomiting are the key factors differentiating subarachnoid hemorrhage from the migraine. We report a case of a 37-year-old female with a previous history of migraines who presented with acute onset of excruciating headaches in the occiput associated with nausea, vomiting, and photophobia in whom a non-contrast computed tomography scan of the head showed hyper-densities involving the bilateral cerebral cortical sulcus and Sylvian fissure and the cerebral angiography showed a complex aneurysm in anterior communicating artery.
Introduction
Subarachnoid hemorrhage (SAH) is a phenomenon in which arterial blood accumulates in the subarachnoid space with cerebral aneurysmal rupture being the most common cause. 1 SAH is a neurological emergency, with mortality rates ranging from 8% to 67%. 2 It typically presents with a sudden onset, severe headache and with patients textually describing it as “the worse headache of their life.” 3 One percent of all emergency department (ED) headaches are secondary to SAH; however, approximately 5.4% of patients diagnosed with SAH were initially misdiagnosed in ED.3–5 Studies report the range of total misdiagnosis of SAH from 12% to 51%. 3 Migraine, or recurrent headache, is among the most common nervous disorders that result due to escalating excitability of the central nervous system (CNS). It can be extremely painful and disabling, associated independently or in combination with neurological, autonomic, and gastrointestinal alteration. 6 Women are more prone to develop migraine, with an incidence of 18% compared to 6% incidence among men. 7
We report a case of a 37-year-old female with a history of migraine who presented with excruciating headaches without aura and was diagnosed as spontaneous SAH. Later on, cerebral angiography showed a complex aneurysm in the anterior communicating artery (ACOm). Our case report aims to highlight the caution about the change in the pattern of headaches in hypertensive patients with a history of chronic migraine, which could be an even more serious pathology, probably SAH due to aneurysmal rupture. This case report has been reported in line with Surgical CAse REport criteria 2020 (SCARE). 8
Case presentation
A 37-year-old female with a history of migraine and newly diagnosed hypertension presented to the emergency with excruciating pain located in the occiput. The pain was acute in onset, radiating toward the forehead associated with nausea, vomiting, and photophobia. There was no history of loss of consciousness or altered consciousness and neurological deficits. She had a history of mild and dull headaches for 1 week for she had taken over-the-counter medications with some relief. The pain suddenly increased over the day and was not relieved with the usual medication she used to take for migraine before she presented to the hospital. There was an absence of aura which she used to experience before, during her migraine attack. She had a history of smoking 4–5 cigarettes/day for the last 10 years.
At the time of presentation to the hospital, she had blood pressure, oxygen saturation, heart rate, and temperature of 180/90 mm of Hg, 97% under room air 74 times/min and 98°F, respectively. Upon examination, both pupils were round, regular, and reactive, neck rigidity absent, with plantar reflex upgoing on the right. Other systemic examinations were unremarkable. The electrocardiogram showed normal sinus rhythm. The echocardiogram and bilateral carotid Doppler ultrasound were unremarkable. A non-contrast computed tomography (NCCT) scan of the head showed hyper-densities involving the bilateral cerebral cortical sulcus, and Sylvian fissure suggesting a subarachnoid hemorrhage (as in Figure 1). The patient underwent a computed tomography angiogram (CTA) which demonstrated a complex ACOm aneurysm (as in Figure 2). Further 3D construction arteriogram sequence demonstrating large lobulated saccular aneurysm noted at the ACOm (as in Figure 3).
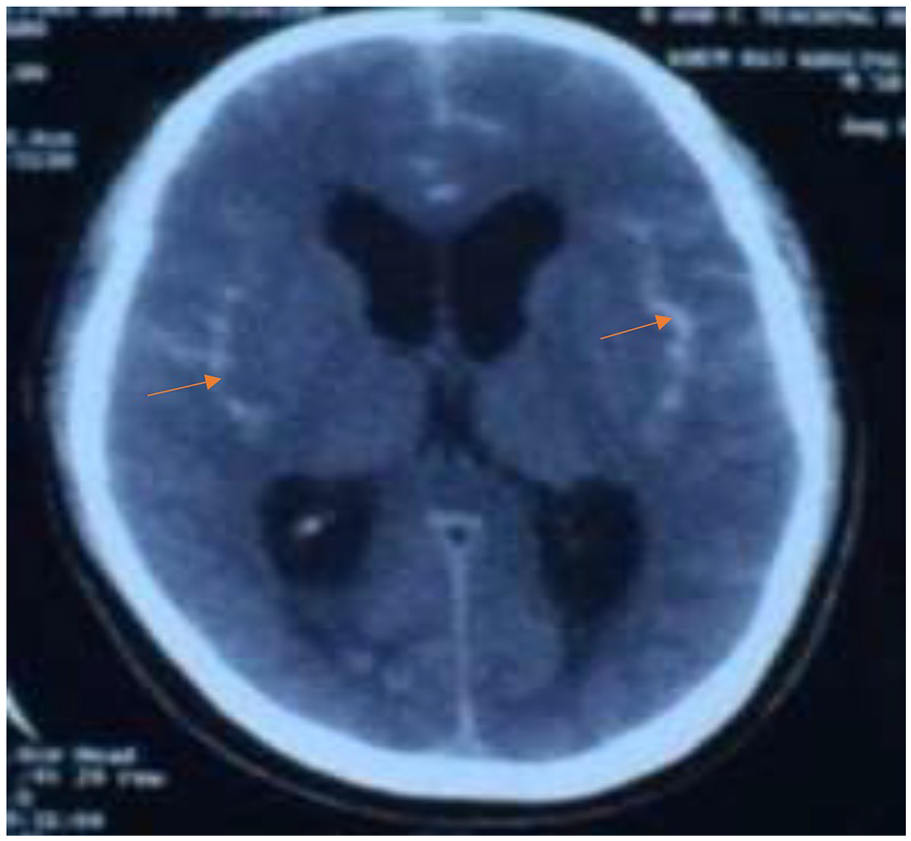
Axial computed tomography scan shows hyper-densities involving the bilateral cerebral cortical sulcus, and Sylvian fissure suggesting subarachnoid hemorrhage.

Computed tomography angiogram (sagittal image) shows a complex anterior communicating artery aneurysm.

3D construction arteriogram sequence shows a large lobulated saccular aneurysm at the anterior communicating artery.
She was admitted to the ICU, stabilized symptomatically, and treated with a reduced dose of mannitol along with labetalol. Tranexamic acid 1 g was given intravenously to prevent the risk of rebleeding along with nimodipine 60 mg per oral 4 hourly to prevent vasospasm. Endovascular along with neurosurgical intervention was done with hemicraniectomy followed by coiling and clipping of the ruptured aneurysm. The patient stayed in the hospital ward under observation for a week and was discharged with full recovery. On follow-up 1 month later, the patient had no complaints and was doing well.
Discussion
Migraine is a neurological disorder that is characterized by recurrent episodes of headache moderate-to-severe, with unilateral predominance, photophobia or phonophobia, nausea or vomiting, and exaggeration of physical activities. 9 Migraines result from escalating excitability of the CNS, which can be extremely painful and disabling, associated independently or in combination with neurological, autonomic, and gastrointestinal alteration. 6 When there is any somatosensory symptom present before the migraine attack, this is called a migraine with aura. 9 In our patient, there was an absence of aura which she used to experience before, during her previously diagnosed migraine attack. A migraine attack followed by a stroke is called a complicated migraine. 9 Women are more prone to develop migraine, with an incidence of 18% compared to 6% incidence among men. 7 Our case described a 37-year-old female with newly diagnosed hypertension. Most patients with SAH experience abrupt onset headache that reaches maximal intensity within 1 min. 10 There are some key historical features of SAH which include sudden onset, the difference in severity or quality compared to previous headaches, and other symptoms, particularly neck stiffness, but also seizure, syncope, focal neurological deficit, and vomiting. 11 Our patient presented with acute onset, excruciating pain located in the occiput, radiating to the forehead, and associated with nausea, vomiting, and photophobia. The pain suddenly increased over the day and was not relieved with the usual medication that she used to take for migraine before she presented to the hospital. It is important to distinguish migraine from SAH for which physical examination plays a great role. Carpenter et al. showed that neck stiffness significantly increased the likelihood of SAH. 4 In addition, the presence of photophobia and phonophobia in these patients is also not specific to migraines since SAH with arterio-venous malformations (AVM) could have similar symptoms. 1 However, there was no abnormality on the physical examination like neck stiffness in our patient, which may be based on slowly progressive SAH due to an aneurysm. A relatively common sentinel headache is caused by partial rupture (minor leak) of the aneurysm. Several studies have reported that approximately 40% of SAH patients have a minor leak. 12 Sentinel headaches are similar to SAH headaches, which may occur days to weeks prior to aneurysm rupture. The incidence appears in 10%–43% of patients with subsequent aneurysmal SAH. 13 A sentinel headache has no obvious signs as a headache caused by a major rupture, and it may be misdiagnosed as a result of other causes. 14 The patient had a subarachnoid hemorrhage due to an intracranial aneurysmal rupture a few days after the pattern of the previously diagnosed chronic migraine changed. It is well known that a sentinel headache occurs before an aneurysmal SAH. However, there is only one previous case report that reported a case of SAH after a change in the existing migraine pattern without any other clinical signs of SAH. 15 Migraine itself is known to be a risk factor for cerebral aneurysm rupture. In a study of 456 patients with cerebral aneurysms, migraine was a risk factor for cerebral aneurysm rupture. 16 In a meta-analysis of 11,264 patients, migraine was also identified as a risk factor for hemorrhagic stroke. 17 The same too was the scenario in our case as she was diagnosed with migraine before and was under the usual medications for migraine. Calcitonin gene-related peptide (CGRP) released from the trigeminal sensory ganglions during the migraine attack exacerbates the neurogenic inflammation and regulates the transmission of pain to the brain. 18 The use of CGRP modulators in the future can prevent the acute attack of migraine and the subsequent formation of the cerebral aneurysm in the patient. Laboratory investigations are important to diagnose SAH and differentiate it from migraine. The study of Karabulut et al. 19 showed that an increase in the neutrophils/lymphocytes ratio was associated with migraines. However, in our patient, the neutrophils/lymphocytes ratio was in the normal range and thus did not support the diagnosis of migraine. Söderholm et al. 20 found that leukocytosis was associated with an increased incidence of SAH. Leukocytosis was absent in laboratory investigations of our patient. When SAH is suspected, computed tomography of the head (CTH) is the initial diagnostic measure. At the onset of bleeding, a CTH can visualize blood more easily. However, it is difficult to appreciate blood on a CT after red blood cells begin to degrade. 21 The American Stroke Association suggests the sensitivity of a CTH within the first 3 days of insult remains approximately 100%. The rate of negative CTHs increases over the next 3–7 days, necessitating a lumbar puncture (LP). 22 CTH was done in our case too, which showed hyper-densities involving the bilateral cerebral cortical sulcus, and Sylvian fissure suggesting a subarachnoid hemorrhage. Classically, if history and symptoms contribute to increased clinical suspicion for SAH after a negative non-contrast CTH, an LP should be performed. 23 Many studies have considered replacing an LP for a CT angiography (CTA) of the brain in SAH diagnosis. A CTA is beneficial because it can diagnose other causes of acute headaches such as venous thrombosis, stroke, or arteriovenous malformation. 24 LP was not performed in our case as the CT finding shows SAH. However, CTA was done which demonstrated a complex ACOm aneurysm. After the diagnosis of SAH is made, it needs urgent treatment to prevent complications. Rebleeding is considered to be the first and most dreaded complication of SAH. More than 40% of patients with SAH in the ED have a systolic blood pressure (SBP) ⩾185 which will increase the risk of rebleeding as a result of a ruptured aneurysmal SAH. 25 A meta-analysis reported patients with SBP >160 mmHg in the ED were more likely to suffer from early rebleeding than those with an SBP >140 mmHg. Therefore, prompt BP reduction and management are suggested, especially in patients with suspected unsecured aneurysms. The Neurocritical Care Society states that it is recommended to reduce the SBP to less than 160 or mean arterial pressure to less than 110 for an unsecured aneurysm. 23 According to class I, level B recommendation by stroke guidelines blood pressure control is needed in patients with SAH and unsecured aneurysm with a titratable agent (i.e., nicardipine, clevidipine, labetalol) to balance the risk of hypertension-related bleeding and risk of stroke with sudden hypotension, and for maintenance of cerebral perfusion pressure. 22 Urgent blood pressure control was also done in our case with a titratable dose of labetalol as our patient had recently diagnosed a case of hypertension and had a BP of 180/90 mm of Hg. Another recognized complication of SAH is vasospasm. Even with adequate medical management, vasospasm increases the risk of ischemic injury, doubling the mortality risk in SAH. 23 Nimodipine was used in our case to prevent vasospasm. Additional medical management strategies include addressing pain and nausea to avoid the Valsalva effect and to control blood pressure control concomitantly. Antiepileptics should be considered in patients diagnosed with SAH. 23 Pain management was done in our case with analgesics. The inflammatory responses to blood breakdown products following aneurysmal SAH lead to increased permeability of blood–brain barriers, and increased exposure to the CNS to peripheral immune cells. Subsequently, activated glial cells release the pro-inflammatory cytokines IL-1β, IL-2, IL-5, IL-6, IL-8, IL-10, IFN-α, IFN-γ, and TNF-α, among which IL-2, IL-6, IL-8, IL-10, and IFN-α were associated with the severity of headache due to aneurysmal SAH and may be effective therapeutic targets in the future. 26 No medication was used to prevent nausea. Antiepileptic was also not used. The Neurocritical Care Society does suggest that tranexamic acid and aminocaproic acid can reduce aneurysmal re-rupture. 27 Tranexamic acid was used in our case to prevent the risk of rebleeding. Endovascular coiling and open surgical clipping are two primary approaches to aneurysmal SAH. The choice of intervention is determined by several variables, including the patient’s complications and aneurysm anatomy, and the availability of surgical expertise. 23 In our case, endovascular along with neurosurgical intervention was done with hemicraniectomy followed by coiling and clipping of the ruptured aneurysm.
The different reported cases of SAH with an unusual presentation are shown in Table 1.
Comparison of the different cases of SAH presenting with different symptoms.

CT: computed tomography; CTA: computed tomography angiogram; NCCT: non-contrast computed tomography; SAH: subarachnoid hemorrhage.
Conclusion
SAH is a neurological emergency and has a good prognosis if treated early and if an unruptured aneurysm is found early. Though the neck stiffness and the leukocytosis are not present in the patient, a sudden change in the pattern of headache in a previously diagnosed chronic migraine with hypertension should prompt consideration of a minor leak from cerebral aneurysm rupture at the back of the treating physician’s mind. Investigations for the diagnosis of SAH should be undertaken, as mortality due to SAH is high if misdiagnosed.
Footnotes
Acknowledgements
None.
Author contributions
H.B.B. and A.B. have written the original manuscript. G.B., B.B., S.G., S.K., M.U., B.A., R.P., and S.K. have reviewed and made the necessary corrections.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Provenance and peer review
Not commissioned, externally peer-reviewed.