
Abstract
Background:
One of the indicators to determine the success of TB treatment is the conversion of sputum from smear positive to negative. However, several factors can lead to this failure of sputum conversion.
Objectives:
To investigate the risk factors for delayed sputum conversion from the person-in-charge (PIC) of the TB program’s perspective.
Design and methods:
This qualitative case study was conducted on September 7th, 2022. Thirty-one PICs of the TB program from 31 public health centers (Puskesmas) in Bandar Lampung, Indonesia, were recruited purposively. All participants were grouped into three FGDs. Developed semi-structured interview questions were used for data collection. Thematic analysis was used to synthesize and cross-reference emerging topics.
Results:
Three themes emerged in our study: (1) individual factors with the sub-themes of medication adherence, education, initial laboratory examination, comorbid disease, nutrition, and lifestyle; (2) environmental factors with the sub-themes of types of support, sources of support, environmental conditions and stigma; and (3) health service factors with the sub-theme of access to health service facilities.
Conclusions:
Problems related to TB management are not only the individual's responsibility but need to strengthen support from the environment and health services.
Background
Treatment success rates and cure rates are critical indicators of tuberculosis (TB) control programs because they play an essential role in preventing the spread of TB and immediately impact reducing the incidence of TB cases. 1 Furthermore, these two figures support the achievement of the End-TB strategy 2016–2035, especially in reducing mortality and the incidence rate of TB. 2 Even though the global TB incidence rate and mortality reduction were still under the target of the World Health Organization (WHO) End TB strategy: 2020 milestones. 3 While referring to the Global tuberculosis report 2021, Indonesia is one of eight high-TB burden countries with alarmingly low levels of treatment coverage in 2020, with best projections of less than 50%. 3
Sputum conversion is a widely used indicator to measure response to TB treatment. Sputum conversion to negative after 2 months of treatment indicates a bacteriological response to anti-TB therapy. This indicator is closely related to the success of long-term treatment and also an increase in the cure rate. 4 On the other hand, some factors influence sputum conversion. The review shows that sputum conversion is affected directly or through risk factors by social determinants, namely age, education, occupation, income, and social class. These factors lead to stratification in society which causes a person to become more resistant or more susceptible to disease, including sputum conversion.5,6
While the risk factors for TB sputum conversion include smoking, malnutrition, HIV-AIDS, alcohol consumption, diabetes mellitus, relapsed and treatment interrupted, and heavy bacillary load.5,7 –9 Such factors contributing to delayed sputum conversion need to be identified as early as possible. 10 Bandar Lampung is one of the city in Lampung province, Indonesia which has a high incidence of TB cases in 2021. Furthermore, there were 156 cases of drug-resistant TB, while the 44 cases of TB deaths with HIV-AIDS. 11 One of the indicators to determine the success of TB treatment is the conversion of sputum from smear positive to negative in the first 2 months of treatment. However, several factors can lead to this failure of sputum conversion. From the TB patients’ perspective, numerous quantitative studies have examined the associated factors of delayed sputum conversion. However, qualitative research on risk factors for delayed sputum conversion is scarce from the perspective of the person in charge of the TB program in the primary health care setting. The results of this study are significant as basic information for policy-making, especially related to advocacy for program allocations to reduce delayed sputum conversion in Indonesia. This research is beneficial to develop strategies and further interventions to prevent delayed sputum conversion and eventually increase the treatment success rates and cure rates of TB programs. This study aimed to investigate the risk factors for delayed sputum conversion from the person-in-charge (PIC) of the TB program’s perspective.
Methods
Study design, study period, and sample
This qualitative case study was conducted on September 7th, 2022. As our study was intended to explore the point of view of the PICs of the TB program regarding the risk factors for delayed sputum conversion in patients with TB, a purposive sample was selected for this study. All thirty-one PICs of the TB program from 31 public health centers (Puskesmas) in Bandar Lampung, Indonesia, were recruited purposively. None refused to participate in our study. The details of the participants are presented in Table 1.
Characteristics of participants (n = 31).

P: participant.
Data collection
Developed semi-structured interview questions were used to achieve the purpose of this study. All participants were grouped into three FGDs (Focus Groups Discussions) Groups which were conducted simultaneously and facilitated by a facilitator in each group. The three facilitators were the principal investigator and members of the research team. Before the FGDs were employed, the protocol was sent to participants. After obtaining both written and verbal consent, the initial interviews were conducted at the participant’s work unit. Face-to-face FGDs were conducted in Bahasa Indonesia, lasted between 50 and 60 min, and were voice-recorded. Notes were taken during the FGDs to supplement the FGD scripts.
Data analysis
The transcripts were not returned to the participants, nor were feedback provided to them. The principal investigator translated the transcripts, and all researcher members checked the accuracy of the recorded interviews. Thematic analysis was used to synthesize and cross-reference emerging topics. 12 The stages were as follows: (1) familiarization with the data; (2) generation of the initial codes; (3) search for themes; (4) review of the themes; (5) definition and naming of the themes, and (6) production of the report. 13 Using the triangulation principle, we validated the data by examining it from the perspectives of the PICs of the TB program through various lenses and with various questions. Then we compared the results with the theories and previous studies. Furthermore, all methodological issues and judgments were documented and subjected to peer review by a third party or seasoned researcher to ensure accuracy and consistency. Researchers also maintained audit trails and made notes on thematic and interpretive decisions.
Ethics and consent
We obtained the ethical clearance from the Committee of Health Research Ethics, Faculty of Medicine, Universitas Lampung, Indonesia (Number 1987/UN26.18/PP.05.02.00/2022). We also received the permission from the institutions as the study site. Prior to the interview, verbal and written informed consent was obtained from all participants.
Results
Of the thirty-one participants who were PICs for the TB program at Puskesmas, the age range is between 27 and 57 years. The majority of participants was female, work as nurses and has worked between 1 and 18 years (Table 1). Based on the results of the FGDs, three themes emerged related to risk factors for delayed sputum conversion in patients with pulmonary TB in our study. These themes include (1) individual factors with the sub-themes of medication adherence, education, initial laboratory examination, comorbid disease, nutrition, and lifestyle; (2) environmental factors with the sub-themes of types of support, sources of support, environmental conditions and stigma; and (3) health service factors with the sub-theme of access to health service facilities (Table 2).
The emerged themes based on the participants’ responses.
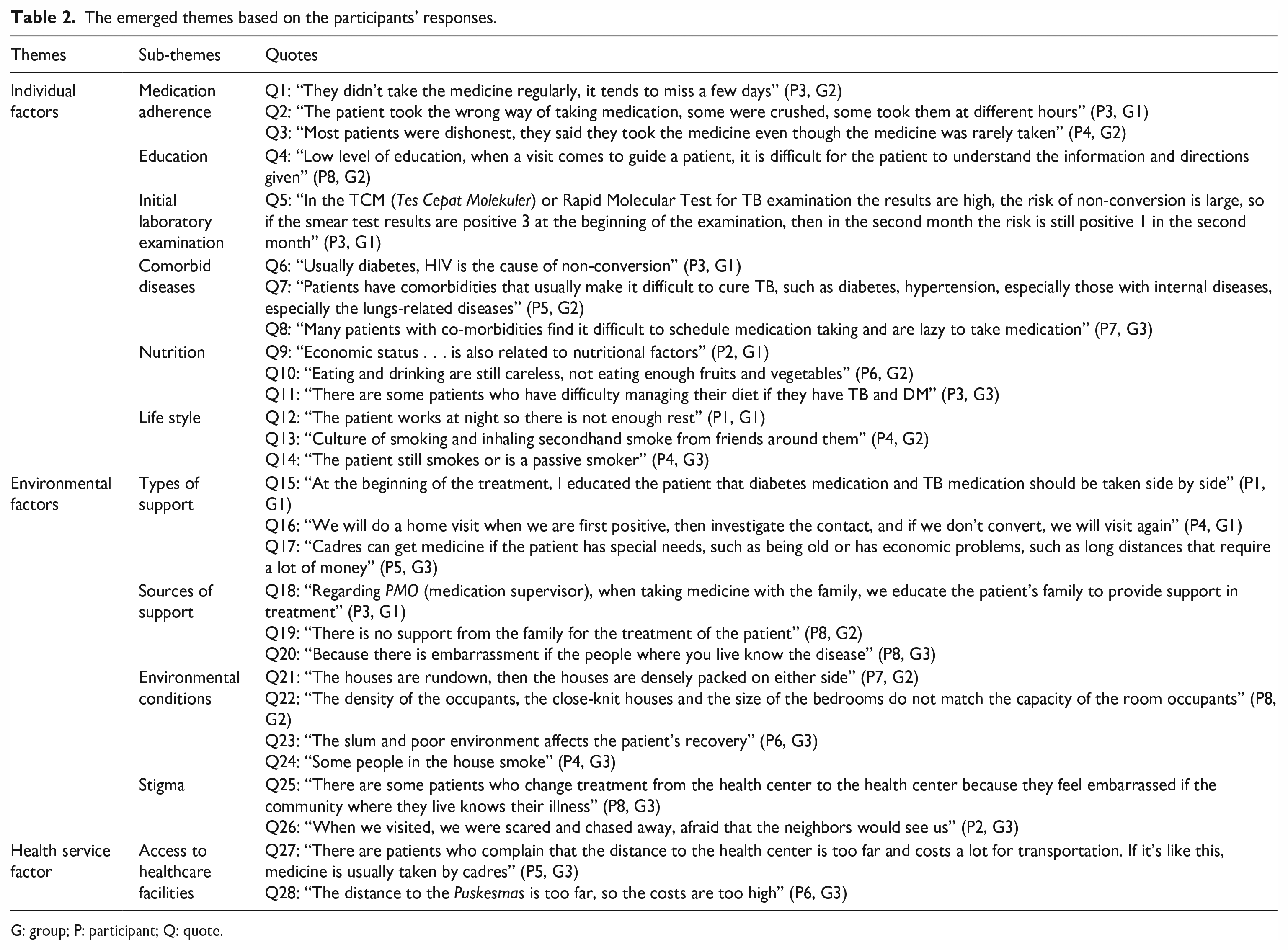
G: group; P: participant; Q: quote.
a. Theme 1: Individual factors
Individual factors are interpreted as risk factors for delayed sputum conversion originating from the individual itself, and consist of six sub-themes namely medication adherence, education, initial laboratory examination, comorbid disease, nutrition, and lifestyle. The majority of participants stated that TB patients did not experience sputum conversion, generally caused by non-adherence to taking medication (quote 1–3), low education (quote 4), relatively poor initial laboratory results (quote 5), have comorbid diseases (quote 6–8), inadequate nutritional intake (quote 9–11), and lifestyles such as smoking or lack of rest (quote 12–14) (Table 2).
b. Theme 2: Environmental factors
External factors come from the surrounding environment both in the form of the living environment and the support of the people around. Environmental factors consist of four sub-themes such as types of support, sources of support, conditions of living environment, and stigma. Forms of support provided by Puskesmas staff and cadres include staff support, motivation, and education/information (quotes 15–17). Support from the supervisor for administering medication, especially the family, as well as neighbors and the surrounding community are also factors that influence sputum conversion in TB patients (quote 18–20). Living conditions with poor sanitation, dense population, slums, and family members smoking in the house contributed to delays in sputum conversion (quotes 21–24) (Table 1). Stigma in the community is also a factor in patients’ reluctance to take routine medication so that sputum conversion is delayed (quote 25–26) (Table 2).
c. Theme 3: Health service factors
Factors of health services with a sub-theme, namely access to health service facilities. The distance between the patient’s house and the Puskesmas which is far away is a factor causing treatment interruption even though in general there are no obstacles related to the availability of TB drugs at the Puskesmas (quote 27–28) (Table 2).
Discussion
Studies from various countries report delayed sputum conversion rates of 5–32%.14,15 In our qualitative study, three themes emerged as risk factors for delayed sputum conversion in pulmonary TB patients based on the perspective of PICs of TB programs: individual, environmental, and health service factors.
1. Individual factors
a. Medication adherence
In clinical practice, treatment adherence and drug resistance remain important considerations in TB patients with delayed sputum conversion. Treatment with non-standard regimens or missed doses of anti-tuberculosis drugs is also a risk factor for delayed sputum conversion in TB patients. 5 Previous research in Malaysia showed that non-adherence in taking medication was a factor associated with delayed sputum conversion. 16 Other potential causes for delayed sputum conversion may be due to patient non-compliance, poor implementation of Directly Observed Treatment Shortcourse (DOTS) therapy, improper dose calculation, possible drug resistance, high pre-treatment bacillary load and a high proportion of cases of relapse and treatment failure.17,18
b. Education
Previous research in Indonesia showed that low education in TB patients was a determining factor causing delayed sputum conversion. 19 These results are consistent with previous reviews which reported that low educational attainment, either directly or indirectly through other TB risk factors, affects the likelihood of successful TB treatment, particularly delayed sputum conversion. 4 The current results are also in line with the review which concluded that higher education levels tend to increase career opportunities and a better work environment. As higher education is also likely to lead to higher incomes and accumulation of productive assets, increase patient access to health care and increase the likelihood of sputum conversion. 20
c. Initial laboratory examination
One of the predictors of delayed sputum conversion in TB patients who are undergoing treatment is the high number of bacilli at the initial examination.14,21 Higher bacillary counts at diagnosis were consistently associated with delayed Acid-Fast Bacilli (AFB) conversion at 2 months of treatment22,23 as revealed in our interviews with participants. The grade of sputum smear positive TB is a predictive factor for the slow conversion of positive sputum smears from positive to negative after 2 months of intensive treatment phase. 24 This study is in line with a case-control study in Suriname which showed that a higher bacillary count was significantly associated with delayed sputum conversion. 25 Several other studies have also shown a significant relationship between high bacillary counts and delayed sputum conversion.21,26
d. Comorbid diseases
Diabetes mellitus was identified as a risk factor associated with delayed sputum conversion among TB patients both in Indonesia and Malaysia.16,19 However, our study findings contradict those of another case-control study which showed no significant effect of diabetes on positive sputum smears after 2 months of treatment. 23 In this regard, we must look at the pathophysiology of diabetes and its relationship to general bodily functions. Diabetic patients have some degree of impaired gastrointestinal drug absorption, even in the absence of clinical gastroparesis. Furthermore, hyperglycemia can also interfere with drug absorption to the tissue level, or interfere with alveolar macrophages or CD4+ cell function. 20 A separate study discovered that individuals with inadequate glycemic control at the time of tuberculosis diagnosis were more likely to experience unfavorable outcomes, such as delayed sputum conversion. 27
As for HIV cases in TB sufferers, in the general population, HIV negative cases and those with HIV status were not recorded had respectively 20 and 30% greater risk compared to HIV cases in TB sufferers. 28 This is probably due to the adherence to treatment undertaken by HIV positive patients which also has a positive effect on TB patients who start their treatment, consequently affecting their sputum conversion. However, previous study in Tanzania have shown that HIV status is not a significant predictor of sputum smear non-conversion 2 months after intensive treatment. 29 A prior study discovered that several immunological indicators could be used to identify an autoimmune component in tuberculosis development. Changes in B cells and follicular Th cell subsets suggest autoimmune-related mechanisms in the pathophysiology of M. tuberculosis infection and suggest new avenues for pulmonary tuberculosis treatment. 30
e. Nutrition
Delayed sputum conversion is more likely in malnourished patients (a body mass index or BMI <18.5 kg/m2). 31 A systematic review related to factors that affect delayed sputum conversion shows that nutritional status, as seen from low BMI, is one of the factors causing delayed sputum conversion in TB patients. 32 Lower BMI is significant in malnourished people and is likely to result in lower immunity. This condition is closely related to the economic level of TB patients, who are generally below the poverty line. 33 A prior investigation demonstrated that having a BMI below 18.5 kg/m2, decreased the levels of immunoglobulins, interleukin-2 receptors, and various T-cell subsets (including suppressor-cytotoxic, helper, and natural killer cells) in individuals with TB. 34 This finding indicates that malnourished individuals with TB may continue to spread the disease within the community for an extended duration.
f. Life style
Smoking is a predictive factor for slow AFB conversion. 24 Smoking has been linked to a range of negative effects on lung health, including more severe lung disease, lung cavitation, delayed conversion of sputum at 2 months, higher rates of treatment default, treatment failures, and relapses. 35 Former smokers exhibited inferior treatment outcomes for tuberculosis. 35 The co-occurrence of smoking and alcohol consumption exacerbates the detrimental impact on the outcome of tuberculosis treatment. 36 Smoking enhances the accumulation of particles in macrophage lysosomes, resulting in decreased migration and degradation of TB granulomas. 37 The phagocytic capacity of macrophages in TB patients is diminished compared to non-smoking TB patients. 38 An increasing global tobacco use and remain largely high in countries with high tuberculosis cases. Therefore, the effective tobacco control measures are needed, especially among low-income countries, with smoking rates highest in those with poverty and low levels of education. 39
2. Environmental factors
a. Types of support
Family support is an attitude, an act of family acceptance of family members, in the form of informational, appraisal, instrumental, and emotional support. 40 So that family members feel that someone is paying attention. People who are in a supportive social environment generally have better conditions than their counterparts without these advantages, because family support is thought to reduce or buffer the effects of individual mental health. Family support has a relationship with adherence to taking medication for TB patients where the supervisor for administering medication should be a family member himself, for instance a child or spouse with more reliable reasons. Apart from being a supervisor for taking medication, they also provide emotional support to TB sufferers. 40
b. Sources of support
Positive family support is expected either to take them directly to check at the health center or at the hospital, doctor or other health worker. Positive family support is full participation in the treatment of sufferers such as; setting menus for eating and drinking, resting patterns, self-care especially hygiene, taking medication and being able to refer sufferers if there are severe side effects of drugs. 40
The long treatment time causes sufferers to be threatened with discontinuation of treatment during the healing period for various reasons, including feeling healthy or economic factors. The result is that the pattern of treatment must be started from scratch with even greater costs and longer treatment time. The role of the family as the supervisor for pulmonary TB patients in supervising, motivating, ensuring sputum re-examination, and providing education to TB patients, will help the healing process for pulmonary TB patients. 41
c. Environmental conditions
The results of our study, which identified the condition of the living environment as a risk factor for delayed sputum conversion in TB patients, is in line with previous studies which showed that there was a significant relationship between the physical condition of the house and the incidence of smear-positive pulmonary TB. 42 This is due to densely populated settlements, there are no kitchen smoke holes, humidity conditions in the house are high and there is no ventilation in the house, even though there is ventilation but it does not work properly, resulting in the temperature in the room and the house not being able to rotate and changing, the result is that the room and house feel cold and stuffy, these conditions have a big influence on the development of M. tuberculosis transmission in the house. This is considered by the physical condition of the house which does not meet the requirements according to the Decree of the Indonesian Minister of Health Number 829/Menkes/SK/VII/1999 concerning health requirements for housing and residential houses. 43
Considering the living environments of TB patients in our study were mainly in the lower altitude, it might affect the TB disease notification. An ecological analysis study revealed that lower altitudes benefit TB transmission since TB notifications declined with increasing altitude. 44 The observed phenomenon could be attributed to reduced crowding and population density at higher altitudes, leading to less time spent indoors by residents.45,46 Furthermore, increased altitude results in elevated UV-B exposure, leading to higher levels of Vitamin D. This increase in Vitamin D may enhance immune response and reduce the subsequent reactivation of tuberculosis. 47
d. Stigma
Stigma is frequently associated with health issues, including tuberculosis. Stigmatization has serious consequences for the emotional and physical health of those suffering from contagious diseases such as tuberculosis. 48 The reasons why there may be a stigma on TB include transmission, inaccurate knowledge of the causes, treatment or contact with marginalized groups such as poverty, racial minorities, sex workers, prisoners, and people infected with HIV/AIDS. 49 The results of this study are in line with the results of previous studies where the community initially did not want to associate with TB patients for fear of contracting the disease. 49 If seen from the characteristics of the place of residence of TB patients who live in densely populated settlements with relatively low levels of education, it affects the misunderstanding of a disease, one of which is pulmonary TB, there are still many people who think that this disease cannot be cured and can be transmitted easily. Lack of knowledge and misperceptions regarding TB transmission contributed to stigma. 50 The patients are afraid of the stigmatization that exists in society so that the patients hide their illness and do not provide space for other people to carry out stigmatizing actions against them. Improving societal understanding and awareness of certain infectious diseases could result in a considerable improvement in a patient’s well-being. 48
3. Health service factors
a. Access to healthcare facilities
The location of health facilities that are far from where they live also affects the delay in sputum conversion in TB patients. The results of this study are in line with previous research which shows that there is a relationship between access to health services and family support together with the utilization of health services for positive smear TB patients. 14 Access to health services is health services that can be achieved by the community, not hindered by geographical, social, economic and language conditions. One of them is the condition or geography that can be measured by distance, travel time, type of transportation that can prevent someone from getting health services. The results of the interviews show that access to health services is one of the risk factors for delayed sputum conversion in TB patients. In general, patients who have difficulty accessing will receive assistance from TB cadres by getting medicines at the Puskesmas.
Limitation
The sampling technique was purposive so the results can not be generalized for the whole population.
Conclusion
Three themes emerged as the risk factors for delayed sputum conversion in TB patients in our study were: (1) individual factors with the sub-themes of medication adherence, education, initial laboratory tests, comorbid diseases, nutrition, and lifestyle; (2) environmental factors with the sub-themes of types of support, sources of support, environmental conditions and stigma; and (3) health service factor with the sub-theme of access to health service facilities. Problems related to TB management are not only the responsibility of the individual, but need to strengthen support from the environment and also health services. Patients should increase their commitment to comply with taking medication by continuing to improve a healthy lifestyle. In addition, families, communities, health professionals, and cadres can jointly support and pay more attention to TB patients during the treatment process. Further research would be needed to initiate alternative interventions in order to reduce those risk factors of delayed sputum conversion in TB patients.
Significance for public health
This article investigated the risk factors for delayed sputum conversion from the person-in-charge (PIC) of the TB program’s perspective. Individual, environmental, and health service factors were emerged as the risk factors for delayed sputum conversion in TB patients. Problems related to TB management are not only the individual’s responsibility but need to strengthen support from the environment and health services.
Footnotes
Acknowledgements
We wish to thank the HETI Project Universitas Lampung for funding this study. We also thank all participants in this study.
Author contributions
Dyah Wulan Sumekar Rengganis Wardani (DWSRW); Bayu Anggileo Pramesona (BAP); Trisya Septiana (TS); Retno Ariza Soeprihatini Soemarwoto (RASS)
Conceptualization: DWSRW
Data curation: DWSRW BAP
Formal analysis: DWSRW BAP TS
Funding acquisition: DWSRW
Investigation: DWSRW BAP
Methodology: DWSRW BAP
Project administration: DWSRW BAP TS
Resources: DWSRW
Supervision: DWSRW
Validation: DWSRW BAP TS RASS
Visualization: DWSRW BAP TS RASS
Writing – original draft: DWSRW BAP
Writing – review & editing: DWSRW BAP
All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from HETI Project Universitas Lampung (No. 6021/UN26/HK.01.02/2022).