
Abstract
Objective:
This study aimed to describe the determinant factors of men’s involvement in antenatal care and childbirth place preference in Indonesia.
Method:
Secondary data from the 2012 Indonesia Demographic and Health Survey was used to identify factors determining men’s presence during antenatal care and childbirth place preference. All factors were analyzed utilizing bivariate and multivariate logistic regression.
Result:
Men living in urban areas, having a sufficient economy, having higher educational levels, and having more interaction with mass media were more likely present during the antenatal care of their wives. Men in Sulawesi and Maluku showed lower involvement in accompanying wives during antenatal care than those in Papua. In terms of delivery place preference, men in age 15–19 and 35–49 years, living in urban areas, having a more stable economy, reading newspapers or magazines as well as watching television at least once a week, and living in Java and Nusa Tenggara, were more likely having wife giving birth in healthcare facilities.
Conclusions:
Type of residence, economic situations, lower educational level, and fewer interactions with mass media and electronics are essential barriers to men’s involvement in wives’ antenatal care visits and childbirth place preference in Indonesia. Particular attention should be put to Sulawesi and Maluku to enforce the men and women as those islands underutilized antenatal care services and health facilities for childbirth.
Introduction
Pregnancy is a natural process; nevertheless, if it is not checked up routinely, it may cause complications that endanger the pregnant woman. According to the data of the World Health Organization (WHO) in 2017, about 810 women die from complications related to pregnancy and childbirth, and about 94% of these occurred in developing countries, with a total maternal mortality rate of about 38%. 1 Complete antenatal care and appropriate support during childbirth are pivotal to ensure mothers and babies well-being and safety. 2 It can also be utilized by healthcare professionals to screen potential risks for pregnant women during their pregnancy and prevent complications. 3 Skillful healthcare personnel before, during, and after childbirth may save mother and newborn life.1,4
The mortality rate in Indonesia remains elevated. 5 Indonesia has an increased maternal mortality rate from 228/100,000 live births to 359/100,000 live births between 2007 and 2012. This number put Indonesia far from the ideal number set by the Millennium Development Goals (MDGs) in 2015, namely 108/100,000; even Indonesia could be said to retreat close to 20 years ago, where maternal mortality was still 390 per 100,000 in 1994. 1 According to WHO, the significant maternal mortality in some areas reflects inequities in health services access, including antenatal care. 1 The primary causes of maternal deaths include severe bleeding, infections, and preeclampsia/eclampsia. 6 Most maternal deaths are preventable. Nowadays, healthcare solutions to treat complications are widely available.
In developed countries, pregnant women at least should have four antenatal care visits, including one each in the first and second trimesters and two visits in the third trimester. In 2015, only 40% of pregnant women in low-income countries had a recommended antenatal care visits. Some significant factors should be examined and explored to enhance maternal health. 1 There is an emergency in the Indonesian maternal health viewpoint and a complex health challenge. Being the fourth most populous country globally causes this problem to be the biggest concern to overcome. 7
Descriptive data from the 2007 Indonesia Demographic and Health Survey (IDHS) depicted that the utilization of antenatal care services in Indonesia still needs to be inclined. 8 The socio-demographic factors of women, such as age, income, type of family, educational level, living in rural areas, and occupation, have been known as the factors contributing to childbirth place preference and antenatal care attendance9,10; however, men involvement is less explored, still have limited evidence, and is unusual regarding its influence on women’s antenatal care visit and childbirth preference.11,12 Under-participation of men in maternal health care may lead to delays in achieving the Sustainable Development Goals (SDGs) to reduce maternal mortality. 13
Antenatal care services may determine the health status of mothers and newborn babies. 14 Hence, if many pregnant women do not have complete antenatal care visit, they may have high-risk complications during delivery. As husbands, men are the closest and most influential ones in supporting complete and fulfilled antenatal care services for pregnant women. Therefore, this study examined male determinants presence in antenatal care and their relationship to the utilization of health facilities for childbirth using secondary data analysis from the 2012 IDHS. 15 This study finding can be a reference for the policymaker to make a regulation and strategy for men to increase access to childbirth in health services and subsequently influence maternal mortality in Indonesia.
Methods
Study design and setting
This study utilized secondary data from the 2012 Indonesia Demographic and Health Survey (IDHS). The study design of the 2012 IDHS was a cross-sectional study. The data variables examined in this study were based on data available in the 2012 IDHS. The IDHS is a national household-based survey. A two-stage cluster sample design was used in the study. The present analysis used data collected for men utilizing a questionnaire developed specifically for men. The study population was ever-married men aged 15–54 years, with a total sample of 9306. Of those participants, the men whose wives were pregnant and gave birth in the 5 years preceding the survey and completed the variable’s analysis were 2204.
The questionnaire included demographic characteristics, reproductive history, pregnancy, antenatal and postnatal care, and delivery assistance. Men’s involvement in antenatal care and childbirth place preference was assessed with two questions: [1] “Respondent was present during antenatal check-up for the most recent child” with the answer “Yes” or “No” and [2] “Place of birth of the most recent child” with the answer “Health facility” or “Other.” 15 The socio-demographic factors related to the men were examined and its association with men’s involvement in antenatal care and childbirth place preference was explored.
The IDHS data collection procedures were approved by the ICF Macro (Calverton, Maryland), which cooperated with the Indonesia Central Bureau of Statistics, the National Population and Family Planning Board, and the Ministry of Health. Informed consent was obtained from respondents at the beginning of the individual interviews. The data was obtained from “Measure DHS.” 15
Statistical methods
Men's sociodemographic characteristics were described. Bivariate associations between potential demographic factors and male participation in antenatal care and preference for place of birth were also examined. These significant values at p < 0.05 were entered into a multiple logistic regression model. All analyzes were performed with SPSS version 22.
Ethical approval
This study has received ethical approval number B.083/KEPK/FKIK/VI/2021 from the Health Research Ethics Committee, Faculty of Medicine and Health Sciences, UIN Alauddin Makassar.
Results
Of 9306 ever-married men interviewed in 2012/2013 IDHS, 2204 men whose wives were pregnant and gave birth in the 5 years preceding the survey completed the research item (Table 1). Of these, most respondents were in age 20–34 years (60.3%), lived in urban areas (50.2%), categorized in the poorest group (24.4%), had a secondary educational level (57.7%), and lived in Sumatera (33.8%). Most men had a wife with first to second delivery (67.4%), did not have insurance (54.9%), were present (accompanying wife) in antenatal care (77.05%), and had a wife giving birth in healthcare facilities (63.75%). In terms of literacy and interactions with mass media and electronics, most respondents were able to read whole sentences (93.5%), did not read newspapers or magazines nor listen to the radio (39.9% and 44.5%, respectively), and watched television at least once a week (89%).
Characteristic of the respondents.

Bivariate analysis and multivariate analysis
In bivariate analysis, most of the explanatory variables were significant predictors of the respondents’ involvement in wives’ antenatal care (p ≤ 0.05; Table 2). The men aged 20–34 years were more likely to be present during antenatal care than those aged 15–19 and 35–49 years. The age group used in this study was based on the Indonesian statistical center, which was based on male reproduction and productivity. 16 Urbanized, wealthy, well-educated men with access to the mass media were more likely to accompany their wives to antenatal care. Men in Sulawesi and Maluku exhibited a lower presence in antenatal care than those in Papua. Nonetheless, in terms of insurance, men with health insurance were more likely to utilize antenatal care services, although it was not statistically significant. There was a similar underutilization of antenatal care services between women who could not read and those who were blind or visually impaired. The higher the parity rate, the more men accompanied their wives for antenatal care.
Bivariate analysis in factors influencing men in accompany wife/present during antenatal care.

p value significance at 0.05 level.
In multivariate analysis (Table 3), men living in urban areas, having a higher wealth index, and reading newspapers or magazines as well as listening to the radio at least once a week, were more likely to accompany their wives in antenatal care than those in their counterparts. Men in Sulawesi and Maluku were less likely to present with their wives in antenatal care than in Papua.
Multivariate analysis in factors influencing men in accompany wife/present during antenatal care.

p value significance at 0.05 level.
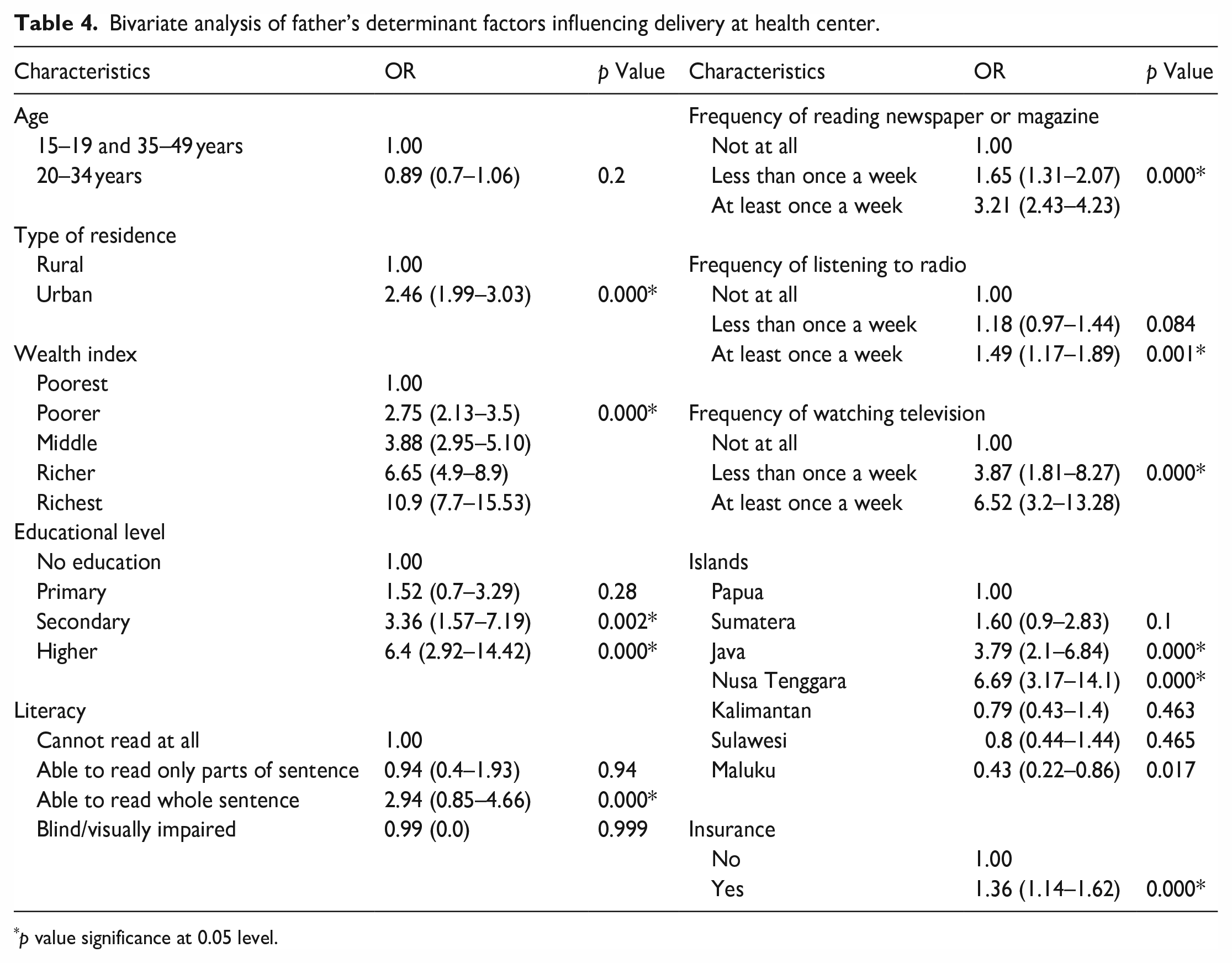
Regarding place to deliver (Table 4), men living in urban areas were 2.46 times to have wives giving birth in healthcare facilities. The higher men’s wealth index was, the more wives chose health facilities to deliver. Men with higher educational level could read whole sentences and were more likely to have wives giving birth in health facilities. Regarding interactions with mass media, men reading the newspaper, listening to the radio, and watching television at least once a week were more likely to have wives giving birth in health facilities. Men living in Java and Nusa Tenggara with insurance were more likely to have wives giving birth in healthcare facilities.
Bivariate analysis of father’s determinant factors influencing delivery at health center.
p value significance at 0.05 level.
In multivariate analysis (Table 5), men aged 15–19 and 35–49 years, living in urban areas, having a higher wealth index, reading newspapers or magazines and watching television at least once a week, and living in Java and Nusa Tenggara were more likely to have wives giving birth in healthcare facilities.
Multivariate analysis in father’s determinant factors influencing delivery at health center.

p value significance at 0.05 level.
Discussion
Men’s involvement in ensuring child development increases over time. 17 Before the children are born, the supervision of early development is required during pregnancy and childbirth. Men’s participation during pregnancy will guide healthier mothers practices and maintain the mothers’ and fetus’ health.18,19 This study found that 77.05% of men accompanied their wives to antenatal care. This percentage was higher than a study in Myanmar which found that of 426 men, 64.8% accompanied their wives in antenatal care. 20 In line with this study, research conducted in Tanzania in 2019 showed that male participation in antenatal care visits was high, with a percentage of 53.9%. 21
This study suggested that the men’s socio-demographic factors affected men’s involvement during antenatal care of their wives and the preferred place for delivery in healthcare facilities. Men who live in urban areas, having a higher wealth index, and interacting with mass media were more likely to accompany their wives to attend antenatal care and had wives giving birth in healthcare facilities. In bivariate analysis, the men’s educational level affected both men’s involvement during wives’ antenatal care and the preferred place for delivery. Socio-economic, personal and interpersonal barriers, health system barriers, and cultural factors also hindered father participation in Iran and Western Kenya.22,23 The similar finding was also exhibited by Wai et al. 20 that Men’s educational attainment and socialization of maternal health education are predictors of male participation.
In Java and Nusa Tenggara, men were more likely to have wives giving birth in health facilities. In contrast, men in Sulawesi and Maluku were less likely to get involved in wives’ antenatal care than maternal visits. Men’s involvement in wives’ antenatal care visits needs to be increased as women can also receive more often maternal healthcare services. 24 Even though women mainly initiate antenatal care, men have a dominant role in decision-making in the household. Men dominate the power in making the decision, including religious, traditional, and cultural factors.13,20 In this multivariate analysis, the educational background was not a statistically significant predictor of men’s involvement in wives’ antenatal care visits. Several reasons could be the underlying causes. A study by August (2015) found that the knowledge of men regarding danger signs in pregnancy was low; however, they were keen to know and learn about it. 25 The antenatal care utilization was significantly affected by the educational level of the spouses.9,26 Therefore, giving positive feedback to healthcare providers and providing an educational supplement for men are potential interventions to increase male participation in maternal health visits and birthplace preference. 27
On the other hand, some men may have reasons for not accompanying their wives into antenatal care, including occupational responsibility, long waiting times, repeated antenatal visits, and discomfort feelings. 28 In addition, different locations in various regions of Indonesia also affect participation in health services. Lack of access to transportation and challenging terrain are also obstacles. This aligns with the previous study, which states that accessibility is the factor that most influences community participation in the use of local health services. 29
Advantages of the research
This finding provides proof regarding the types of socio-demographic factors influencing men’s involvement in complete antenatal care visits of pregnant women. Furthermore, it is expected that these factors can later be modified to carry out various activities to increase men’s involvement in supporting pregnant women in utilizing antenatal care services. Besides that, after knowing the most influential factors, the policymaker can make a regulation and strategy targeted to the men to increase the uptake of delivery in healthcare services and later can impact maternal mortality in Indonesia.
Limitations
This study has potential limitations. First, this study may be subject to memory bias since this study employs a cross-sectional approach and relies on memory in recent years regarding men’s involvement in antenatal care. Second, the answer regarding the men’s involvement in antenatal care does not explain in detail whether they do not accompany their wives due to work or consider it unnecessary. Third, the involvement of men also needs to be explained whether the men are only limited to picking up the wives at the hospital or participate in consultations with doctors because the role may differ in decision-making in determining the selection of health facilities for childbirth.
Conclusion
Men living in an urban area, having a more stable economy, and interacting with mass media are more likely to accompany their wives to antenatal care and have wives giving birth in healthcare facilities. Men in Sulawesi and Maluku are less likely to accompany their wives in antenatal care visits than in Papua. Moreover, men in Maluku are also less likely to have wives giving birth in health facilities. Based on those circumstances, the national and local health centers may have some programs to involve men to increase knowledge about maternal health and provide more socialization in mass and electronic media targeted to men to increase the uptake of antenatal care and health facilities childbirth coverage.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.