
Abstract
Background:
According to current estimates, there are 665,723 people in Ethiopia who have human immunodeficiency syndrome. As Ethiopia inches closer to attaining the 95/95/95 targets for treatment coverage and reaching epidemic control, however, attrition from anti-retroviral treatment is still one of the key programmatic challenges.
Objective:
To assess the incidence of attrition rate and its predictors among adult HIV patients receiving anti retro viral treatment at Public Health Facility in Adea Berga/Enchini District.
Method:
A 6-year (June 28, 2015 to June 27, 2021) institution-based retrospective cohort study was used to recruit 540 study participants by using simple random sampling. Data were obtained from chart review, coded, entered into Epi Data, and exported to Stata 14.2 software for analysis. At least 1 month missed appointment is considered as attrition and the predictors of attrition were identified using bivariable and multivariable Cox proportional hazard models and an adjusted hazard ratio (AHR). Bivariate and multivariate analyses were conducted to find predictors of attrition, p-value < 0.05 was considered statistically significant.
Results:
From the total 540 study participant, 158 (29.26%) patients were discontinuing from follow up making the incidence rate of attrition 9.50 per 100 person years .Being WHO clinical stage III or IV (AHR = 1.96,), non-practice of Appointment spacing model (AHR = 3.98), poor or fair ART adherence level (AHR = 6.47), age groups (15–24) years (AHR = 1.73) and Others ART linkage points[index case testing, tuberculosis clinic and referral from private/public health institutions] (AHR = 1.76) were significantly associated.
Conclusions:
The study showed that the incidence of attrition among adults receiving antiretroviral therapy was high. Patient sociodemographic, clinical, and treatment-related factors were significantly associated with patients on ART.
Introduction background
Attrition is the sum of the dead, lost to follow-up (LTFU), dropout and discontinuation from chronic ART care. 1 Since the beginning of the epidemic in 2019, 75.7 million people have become infected with the Human Immunodeficiency Virus (HIV); among the 20.7 million people living with HIV in Eastern and Southern Africa, 15.0 million are receiving treatment; there were 730,000 new HIV infections in 2018, 660,000 among people aged 15 and older, and 300,000 AIDS-related deaths in 2018. Moreover, it takes a tremendous toll on human health, as it has been claimed that 38.0 million people were living with HIV so far globally, 1.7 million people became newly infected with HIV, and 690,000 people died from AIDS-related illnesses. Twenty-six million people were accessing antiretroviral therapy as of the end of June 2020. Moreover, 25.4 million people were accessing antiretroviral therapy, up from 6.4 million in 2009. 2
In 2018, 79% of PLHIV knew their status; 71% of eligible PLHIV are on ART, and 87% of those on ART have attained viral suppression in Ethiopia. However, viral load service coverage is 51%. The HIV prevention response will focus on adolescent girls, young women, and their partners, as well as key and priority population groups that include female sex workers, prisoners, distance drivers, divorced and widowed women, PLHIV and their partners, and mobile and resident workers at hotspot areas. Moreover, the general population will continue to be reached through social behavioral change communication through media and HIV prevention interventions integrated with the health extension program and the women’s development army. 3
Despite all efforts, retention in care has been challenging in many sub-Saharan African countries, including Ethiopia. 4 Countries face the dual challenge of managing and sustaining growing cohorts of patients on ART in addition to the need for increasing access to ART for the patients who still do not have access to it. The high levels of attrition undermine the proven benefits of early treatment for individuals and the prevention of onward transmission of HIV. 5 The retention of patients in care is a central pillar of the continuum of HIV care. It involves adherence to ART needed to achieve viral load suppression, which is the basis of individual and societal benefits. Furthermore, reductions in long term patient retention and high rates of attrition from treatment programs pose a serious challenge to treatment program outcomes.6,7 Attrition from care negatively impacts the immunological benefits of ART and leads to drug resistance, treatment failure, morbidity, hospitalization, and death.5,8 Multiple factors improve the coverage and better management of patients on ART care. Moreover, distance ART treatment regimen. 9
Even though attrition remains a huge programmatic challenge for HIV-positive adults in ART programs.3,10 Little information is known about the incidence and predictors of attrition in ART services in Ethiopia, particularly the study area. A separate study on incidence mortality, dropout rate, or LTFU, on the other hand, may underestimate or overestimate the case. Therefore, LTFU, dropout, and mortality were grouped as one in this study to solve this problem. The predictors of attrition from ART among adults enrolled as ART-initiated clients have not been studied yet in the study area. Therefore, the result of this study will be important in identifying the predictors of attrition from ART among people living with HIV after initiation of ART and the possible predictors of attrition status that can be used to design appropriate corrective action to reduce the occurrence of attrition status among HIV patients and improve the clinical outcome of patients who initiate ART.
Methods and materials
Study area and period
The study was conducted in Adea Berga district, west Shoa zone, central Ethiopia. Adea Berga district is one of the 23 districts in the West Shoa zone. The district is located 68 km from Addis Ababa, Ethiopia’s capital city, and 107 km north of the zonal town of Ambo. The area is located between 9°12″ to 9°37″N and 38°17″ to 38°36″E. 11 Its annual average precipitation is 1290 mm, and the minimum and maximum annual average temperatures lie between 12°C and 25°C. The mean annual rainfall of the district is 1290 mm. More than 85% of farmers in the study area mostly practice crop-livestock mixed farming, which is predominantly rain-fed. The district has two cement factories (Mugher and Dangote). The 2007 national census reported a total population for this district of 120,654, of whom 60,366 were men and 60,288 were women; 15,940 or 13. Twenty-one percent of its population were urban dwellers. The health institutions of the district include six governmental facilities (one primary hospital, five HCs, and one private HC). It has two ART facilities from the government and one from a private health facility. The study was conducted in Enchinni primary hospital and Enchinni Health center from November 01, 2021 to November 15, 2021.
Study design
An institution-based retrospective cohort study was undertaken.
Source population
The source population ART initiated adult clients who registered for the chronic HIV care and support program at Adea Berga district/Enchinni, selected ART public health Facility.
Study population
The study population is selected adult clients whoever initiated ART at Adea Berga district/Enchinni Primary Hospital & Enchini HC.
Inclusion and exclusion criteria
Inclusion criteria
All people aged 15 years and above who ever Started ART care clinic at Adea Berga district/Enchinni, Selected ART Public Health Facility.
Exclusion criteria
PLHIV on ART care clinic with incomplete socio-demographic and clinical baseline information were excluded from the study. Transfer out to other facilities was also excluded.
Sample size determination
The sample was determined for the first objective using OpenEpi, Sample Size for Frequency in a Population formula, from the study conducted in Woldia 12 by using 23.8% that means (100%–76.2%) proportion of Attrition among adult ART initiated clients in Woldia Town Public Health Facilities, Northeast Ethiopia, 5% margin of error with 95% confidence interval.

For the second objective, the sample was calculated based on OpenEpi’s Fleiss with Continuity Correction (CC) formula, considering the following assumptions: 95% CI, power 80%, ratio of unexposed to exposed: 1:1, anticipated proportion of the hazard of attrition among adults with functional status (bedridden) HIV patients (exposed) = 8.5% and adults working (unexposed) = 2.6%, and AHR = 3.3 . 12 Accordingly, sample size for functional status of bedridden exposed group is 270 and for functional status of working as unexposed group 270 which gives 540. So, the final sample size in this regard yielded 540, which is greater than the sample size calculated for other variables. See Table 1.
Sample size calculation using OPEN Epi, to determine the incidence and predictors of Attrition among adults received ART clients in Adea Berga District selected ART Public Health Facilities,Oromia, 2022.

CI: confidence interval; AHR: adjusted hazard ratio; WHO: World Health Organization; ART: anti-retro viral therapy.
Sampling procedure
Simple random sampling technique was used to recruit predetermined sample size by using registration/card number of the clients enrolled. From the total 1075 charts of adult records that are enrolled from (June 28, 2015, to June 27, 2021), 540 samples were selected randomly by using lottery methods based on their medical record numbers and the data were extracted with its necessary information. Adults ever started ART who fulfill the criteria were taken from previous 6 years (June 28, 2015, to June 27, 2021, and report of Adea Berga district selected ART public facilities (Enchinni primary hospital and Enchinni HC) (Figure 1).

Profiles of HIV/AIDS clients in Adea Berga district Public Health Facilities (June 28, 2015 to June 27, 2021) Central Ethiopia; 2022.
Data collection tools, measurements, and procedures data collection tools and measurements
The source of data was individual patient record documents, including registers and monitoring cards, SMART care, patient follow-up cards, and patient follow-up charts. First, the available information on the patient records was observed, and an appropriate data extraction format was prepared in the English language. Then the data were extracted by two nurses and one health officer who had ART training using the prepared data extraction format from the already existing records of clients’ follow-up cards. Two data clerks have also supported them by identifying the charts. Charts were retrieved using the patient registration number, which was found in the database (SMART Care) in the electronic system.
The clients’ outcome status was recorded as dead (of any cause), lost, dropped, stopped, or retained in care. The study began when clients-initiated ART; then, the duration of the study was the follow-up of clients until their next visit. Adult clients who were transferred out (TO) and a patient chart with missed age and date of ART initiation were excluded. The time component was taken from the first date of ART initiation, which was considered as a baseline date or time zero for this study. For adult ART clients, the event of interest is considered a success (event = 1) and a failure (event = 0). The outcome was labeled as lost, dropped out, dead, stopped, or retained. The follow-up status of clients was calculated in months (years), with a maximum of 72 months, or 6 years. If the client was active on follow-up during the data collection period, then the client was labeled as “retained in care,” otherwise labeled as “censored due to administrative censoring,” otherwise labeled as “attrition from care.” The time to attrition or censoring was recorded in months, starting from the date of ART initiation to the last date of a missed appointment, stopped treatment, or death, and the last date of medication pick-up in the case of administrative censoring.
Data collection procedures
Data collectors were trained for 1 day on data extraction procedures, questions included in the data extraction, the retrieval techniques, the objectives of the study, the selection of study participants, and the importance of privacy and confidentiality of the information obtained from the records. Based on the result, data collectors were reoriented, and the data extraction format was modified. Data collected from each record was checked for completeness, clarity, and consistency by the principal investigator at the end of each data collection day.
Variables
Dependent variable
Incidence of Attrition
Independent variables
Socio-demographic characteristic: Age, sex, place of residence, religion, level of education, occupation, marital status, disclosure status, cell phone
Behavioral factors: substance use(alcohol, chat, cigarettes, and drugs use)
Nutrition-related factors: BMI
Baseline clinical characteristics: WHO clinical Stage, Prior history of tuberculosis, functional status, CD4 counts, VL Count
Treatment-related factors: initial ART regimen, initial regimen change, IPT use, CPT Use, HAART and adherence level,
Operational definitions
Events: Attrition, which is defined in this study as the occurrence of attrition (lost to follow-up (LTFU), dead, drop out and stop) in people living with HIV any time after enrolled in adult chronic HIV care. 12
Adult: clients on ART were categorized as an adult if they were 15 years and above.
Censored: PLHIV was censored by the first date of lost, drop out, and died by any causes before the end of the follow-up period and completed the follow-up period without developed the event12,13
Lost: patients missing their appointment for follow up or drug picks up at least for 1–3 months. 10
Mortality: Recorded as “dead” on the Adult’s medical card.
Drop out: patients missing their appointment for follow up or drug pick up for more than 3 months. 10
Time scale: The time to occurrence of an event or censored cases was measured in months and calculated in both month and years for interpretation purpose accordingly.
Transferred out: those patients who are transferred to other health care facilities. 10
Substance use: was referred to as the use of at least one of the substances (alcohol, chat, cigarettes, and drugs) in an individual’s lifetime to alter mood or behavior. 14
Level of ART adherence: Good (≥95% or <2 doses missed per month or <3 dose missed per 2 months), fair (85%–94% or 3–5 doses missed per 30 doses or 3–9 doses of 60 doses), and poor (less than 85% or >6 doses of 30 doses or >9 dose of 60 doses). 15
Functional status defined as (a) Working = able to perform usual work in or out of the house, harvest, go to school (b) Ambulatory = able to perform activities of daily living but not able to work or play (c) Bedridden = not able to perform activities of daily living. 15
Data quality control
Data quality was assured through careful design of data extraction formats, appropriate modification, appropriate recruitment, and adequate training and follow-up for data collectors and supervisors. A pretest was performed on 5% of the populations in the selected public health facilities from records of adult ART registers and follow-up charts. Data quality was ensured during data extraction, coding, entry, and analysis. During data collection, adequate training and follow-up were provided to all data extractors and data clerks. The principal investigator conducted day-to-day on-site supervision during the whole period of data extraction.
Codes were given to the data extraction form during the data extraction to identify errors and trace them back using the codes. Data were first checked manually for completeness, then coded and entered into Epi-Data version 3.1 statistical software and cleaned thoroughly before being transferred to Stata version 14.2 for further analysis. The data was further cleaned by visualizing, calculating frequencies, and sorting in Stata. Corrections were made according to the original data.
Data processing and analysis
Data was edited, coded, entered, cleaned, and analyzed using Stata version 14.2 software. The frequency distribution was done to check for outliers, consistencies, and missing values. A descriptive analysis was computed. The incidence density rate (IDR) of attrition was calculated for the entire study period. A Kaplan-Meier estimate was used to estimate the cumulative attrition status of clients on ART. The log-rank test was used to compare attritional status curves between the different categories of the explanatory variables.
Both the bivariable and multivariable Cox proportional hazard models were used to identify the associated factors. Variables with a p-value less than 0.05 in the bivariate Cox proportional hazard model analysis are entered into the multivariable proportional hazard model. Ninety-five percent confidence interval of hazard ratio was computed, and a variable having a p-value of less than 0.05 in the multivariable Cox proportional hazards model was considered as significantly and independently associated with the dependent variable. The assumptions of the Cox proportional hazard model were checked using the Schoenfeld residuals test; the global test was above 0.05 on each independent variable, and the overall global test was=0.1903 (Supplemental File 1) and Cox proportional hazard model for its fitness to the data was checked using proportional hazard assumptions Harrell’s c (c = 0.8240), which indicates that this study can correctly order survival times for pair of Adults 82.40% of the time based on observations of fitted variables in the model. Generally, it can be concluded that the final model fits the data successfully and multicollinearity was also checked by using VIF (mean VIF = 1.32; (Supplemental File 2). In multivariate analysis, the association was summarized using an adjusted hazard ratio and statistical significance was considered at p value < 0.05. Finally, the findings were presented using tables, graphs, and texts.
Results
Socio demographic and behavioral characteristics of adults on ART
In total, 540 patients who had a follow-up at ART clinics in public health facilities were included in the study. The mean ages of the respondents were 36.6 (SD ± 9.11) years. 238 (44.07%) of them were found to be in the age group of 25–34 years. Adults were followed for a minimum of 1 month and a maximum of 72 months, starting from June 28, 2015, to June 27, 2021. The median duration of months on ART from the start of ART till the end of the follow-up period was 38 months (IQR, 1–72).
According to the findings, 93 (17.22%) of the 305 female participants (56.48%) experienced attrition. Four hundred twenty-five (78.7%) of the study participants were living in rural areas, of which 124 (22.96%) experienced attrition. One hundred fifteen (21.3%) study participants were living in an urban area, of which 34 (6.3%) experienced attrition. Three-fourths of the respondents 404 (74.81%) were Orthodox of which 122 (22.59%) experienced attrition. Moreover, 284 (52.59%) were unable to read or write, of which 64 (11.85%) experienced attrition. One hundred ninety-three (35.74%) of the respondents were housewives, and 346 (64.07%) were married. The majority of respondents (482 (89.26%)) did not use substances, with 135 (25.0%) experiencing attrition. Fifty-eight (10.74%) of the respondents were substance users in addition to their ART medication; of the total, 23 (4.26%) had experienced attrition. There were 49 (84.48%) alcohol drunkers among substance users, six (10.34%) cigarette smokers and alcohol drunker, and three patients who take alcohol, smoke cigarettes, chew tobacco, and drink alcohol (Table 2).
Socio demographic characteristic of adults receiving ART related with attrition in Adea Berga district public health facilities, central Ethiopia 2022, n = 540.

ART: anti-retro viral therapy.
Others: Religion with Muslims and waqefata followers.
Self employee: Occupational status with daily laborer, drivers, merchant and female commercial sex workers.
Primary & above: Educational status with grade (1–8, 9–12, and diploma & above).
Base line clinical, treatment and health system characteristics
Out of the total respondents, 236 (43.7%) were linked to ART care from VCT, and 144 (26.67%) were underweight (BMI < 18.5 kg/m2) according to their BMI. Eighty-five (78.70%) of the 108 study participants who were eligible for nutritional assistance had not received it, of whom 48 (44.44%) had experienced attrition. Of the 460 (85.19%) who had hemoglobin levels above 10 gm/dl at the initiation of ART, 130 (24.07%) were having attrition, while of the 66 (12.22%) who had hemoglobin levels below 10 gm/dl at the initiation of ART, 25 (4.63%) were having attrition and 14 (2.59%) had not been recorded at the initiation of ART. Regarding medication adherence, 190 (35.19%) of them had poor or fair adherence at the last visit of patient follow-up. felt better, social stigma, delivery traveling problem, and pill burden were among the 40 (21.05%), 38 (20%), 29 (15.26%), and 7 (2.63%) reasons for poor or fair adherence, respectively. There were 259 (90.56%) study participants who were eligible for CPT and received it, with 107 (37.41%) experiencing attrition. Similarly, 478 (93.00%) of 514 study participants were eligible for IPT and received it, with 123 (23.93%) experiencing attrition. Most patients’(354 (65.56%)) eligibility criteria for starting ART were test and treat, with 95 (17.59%) experiencing attrition.
Almost two-thirds (63.89%) of study participants began on a TDF+3TC+EFV base-line regimen. Almost all, 523 (96.5%) of the respondents, had not developed a drug side effect, of which 154 (28.52%) were experienced attrition. And, more than half (54.44%) of adults had changed or substituted their ART into another drug regimen, while 246 (45.56%) had not changed or substituted their ART, of which 135 (25.0%) experienced attrition. Almost all of the drug substitutions (293, or 99.66%) were due to the availability of new drugs (TDF+3TC+DTG). The majority of the clients who were not on ASM were 448 (82.96%), with 149 (27.59%) experiencing attrition. About 212 (39.26%) respondents had developed an opportunistic infection, of which 107 (19.81%) experienced attrition. There were 41 (19.34%) with unexplained chronic diarrhea, 34 (16.04%) with unexplained prolonged fever, 24 (11.32%) with PTB, and 13 (2.41%) with attrition. Each person had bacterial pneumonia, a minor mucocutaneous skin infection, and oral candidacies in about 23 people (10.85%) (Table 3).
Base line clinical, treatment and health system characteristic of among adults receiving ART related with attrition in Adea Berga district public health facilities, central Ethiopia 2022, (n = 540).

VL: viral load count; ART: anti retro viral therapy; VCT: voluntary counseling testing; OPD/IPD: outpatient/inpatient department; MNCH: mother neonatal and child health; PMTCT: prevention to child transmission; AZT: ziduvodene; 3TC: lamivudine; NVP: nevaripine; EFV: efavirenz; DTG: dolutegravir; TDF: tenofevir.
Others: from index case testing, TB clinic referral from private and public health institutions.
Attrition status among adult patients receiving antiretroviral therapy
At the end of 6 years, 382 (70.74%) of respondents had been retained, while 67 (12.41%) had dropped out, 47 (8.70%) had LTFU, 43 (7.96%) had died, and 1 (0.19%) had stopped. The cumulative incidence of attrition in this study was 158 (29.26%) (Figure 2).

Diagrammatic presentation of type outcome status among Adults Receiving ART Related with Attrition in Adea Berga district Public Health Facilities, central Ethiopia 2021, (n = 540).
The Kaplan-Meier estimate of attrition from care were 9.92% (7.67–12.79), 14.69% (11.93–18.03), 16.39% (13.46–19.88), 19.99% (16.74–23.78), 25.72% (22.00–29.95), 29.53% (25.45–34.09), 33.09% (28.57–38.12), and 48.41% (40.55–56.93) at 6, 12 months, 18, 24, 36, 48, 60, and 72 months, respectively, while the retention in care was vice versa. The Kaplan-Meier failure curve increases stepwise, and it crosses the failure function at a failure probability of 0.5 by confidence interval as time increases (Figure 3).

Kaplan–Meier failure estimates by failure function of attrition among adult patients on ART in Adea Berga district Public Health Facilities, central Ethiopia 2022.
The total time observed was found to be 1662.33 person-years, or 19948 person-months of observation, with a median follow-up time of 38 months (IQR 1–72). The overall incidence rate of attrition was estimated to be 9.50 (95% CI: 8.13–11.11) per 100 person-years (PY) or 0.79 (95% CI: 0.68–0.93) per 100 person-months. Drop out, LTFU, death, and stopping ART were responsible for 4.01/100 PY, 2.83/100 PY, 2.60/100 PY, and 0.06/100 PY of the total incidence of attrition rate, respectively.
The incidence density rate of attrition among males was 9.14, whereas among female was 9.78 per 100 person-years. Females accounted for 950.92 PY of total observation time. The incidence density rate of attrition among the rural was 9.29, whereas that among the urban was 10.37 per 100 PY. Rural observation time was 1334.58 PY of total time. The Attrition incidence density rate was 9.20 per 100 PY among disclosure status that disclosed to someone else and 12.29 per 100 PY among not disclosed. In total, the time disclosed to someone else was 1610.5 PY of observation. The incidence density rate of attrition among those with cell phone addresses was 13.71 per 100 person-years, whereas it was 8.55 per 100 person-years among those without cell phone addresses. The absence of a cell phone address accounted for 1356.08 PY of total observation time. The incidence density rate of attrition among substance users in addition to ART medications was 12.42 per 100 PY, whereas it was 9.14 per 100 PY among non-users. The total time spent by study participants who did not use substances was 1477.17 PY.
The incidence density rate of attrition among the ART linkage points of VCT, OPD, IPD, MNCH, and others (ART: anti-retro viral therapy.) was 6.83, 10.36, 21.93, 8.53, and 16.20 per 100 person-years of follow-up, respectively. The incidence density rate of attrition was 16.31 per 100 person-years of follow-up among those with a BMI less than 18.5 kg/m2, and 7.57 per 100 person-years of follow-up among those with a BMI greater than or equal to 18.5.BMI greater than or equal to 18.5 was 1294.42 p.y. among study participants. The incidence density rate of attrition was 12.12, 9.37, and 4.32 per 100 person-years of follow-up, respectively, for hemoglobin levels at baseline less than or equal to 10 (gm/dl), greater than 10, and not recorded.
Others: ART linkage point from index case testing; tuberculosis clinic; referral from private or public health institutions.
The incidence density rate of attrition among those on ASM was 2.54, while it was 11.39 per 100 person-years of follow-up among those not on ASM. It was 1307.67 PY of total time among study participants who were not on ASM. The incidence density rate of attrition among the eligibility criteria for initiating ART (CD4 cell count, WHO clinical stage 3 and 4), both CD4 cell count and WHO clinical stage 3 and 4, and test and treat were 5.30, 10.30, 14.00, and 11.63 per 100 person-years of follow-up, respectively (Table 4).
Incidence of attrition stratified by socio-demographic, baseline clinical, and treatment characteristics of ART initiated adult clients in Adea Berga district Public Health Facilities, central Ethiopia 2021, (n = 540).

IDR: incidence density rate; PY: person years; VL: viral load count; AZT: zudovudine; 3TC: lamivudine; NVP: nevarapine; EFV: efaverinz; TDF: tenofevir; DTG: dolutegravil.
Others: Religions with Muslims and waqefata followers.
Self employed: Occupational status with daily laborer, drivers, merchant and female commercial sex workers.
Comparison of survival/failure status using Kaplan Meier
The Kaplan Meier survival curve decreases stepwise, and it crosses the survival function at survival probability of 0.5 by confidence interval while time increases (Figure 4).

Kaplan–Meier survival estimates by survival function of attrition among adult patients on ART in Adea Berga district Public Health Facilities, central Ethiopia 2022.
The incidence of attrition has also shown differences among different levels of adherence. The incidence of attrition among respondents with a sub-optimal adherence status of fair or poor was higher than that among respondents with good adherence (Figure 5).

Kaplan–Meier failure estimates by Adherence level of attrition among adult patients on ART in Adea Berga district Public Health Facilities, central Ethiopia 2022.
The incidence of attrition had shown that differences among different levels of the WHO clinical stage. The incidence of attrition at advanced WHO clinical stage of either stage III or IV was higher than stage one (Figure 6).

Kaplan–Meier failure estimates by baseline WHO stage of attrition among adult patients on ART in Adea Berga district Public Health Facilities, central Ethiopia 2022.
The log-rank test revealed that age group, marital status, cell phone address, disclosure status, occupational status, educational status, ART linkage point, WHO clinical stage at baseline, CD4+ count at baseline, ART adherence level, Viral load count at or above 6 months, functional status at baseline, BMI at base line, presence of OI during enrollment, drug substitution during follow up, cotrimoxazole preventive therapy, IPT given for eligible Eligibility criteria, Base line regimen, & Appointment spacing Model(ASM) had statistically significant difference among survival curves of observed groups with p-value < 0.05 (Table 5).
Log rank test for equality of survivor functions between groups among adult patients receiving ART related to attrition in Adea Berga district public health facilities, central Ethiopia 2022 (n = 540).

VL: viral load count; BMI: body mass index; TB: tuberculosis; IPT: isonized preventive therapy; CPT: cotrimoxazole preventive therapy; ASM: appointment spacing model.
Predictors of attrition among adult ART clients
In the bi-variable analysis, variables like the age of the patient, marital status, disclosure status, cell phone address, educational status, ART linkage point, baseline WHO clinical stage, base line BMI, functional status, ART adherence level, and appointment spacing model (ASM) were found to have a p-value less than 0.05 and were included in the multivariate analysis.
However, some variables were not included in the multivariate analysis because they violated the proportional hazard assumption with a p-value of less than 0.05 during the global test. Those variables were the baseline CD4 count, the viral load count at six or above, and drug substitution. On the other hand, some variables were not included in the multivariate analysis because of multicollinearity and a variation inflation factor (VIF) above 10. These variables included occupational status, baseline regimen, opportunistic infection, and cotrimoxazole non-users. Finally, five of the predictors were found to be statistically significant with attrition during multivariate Cox proportional regression analysis at a 95% confidence level (p-value < 0.05). The Cox proportional hazard model (multivariate analysis) showed that age group, ART linkage point, WHO clinical stage, poor/fair ART adherence level, and appointment spacing model non-users were found to be significant predictors of attrition at the 5% significance level (p-value < 0.05(Table 6)).
Bi-variable and multivariate analysis using Cox regression model for predictors of attrition among adults on ART at Adea Berga district public Health facilities, central Ethiopia from June 2015 to June 2021). (n = 540).
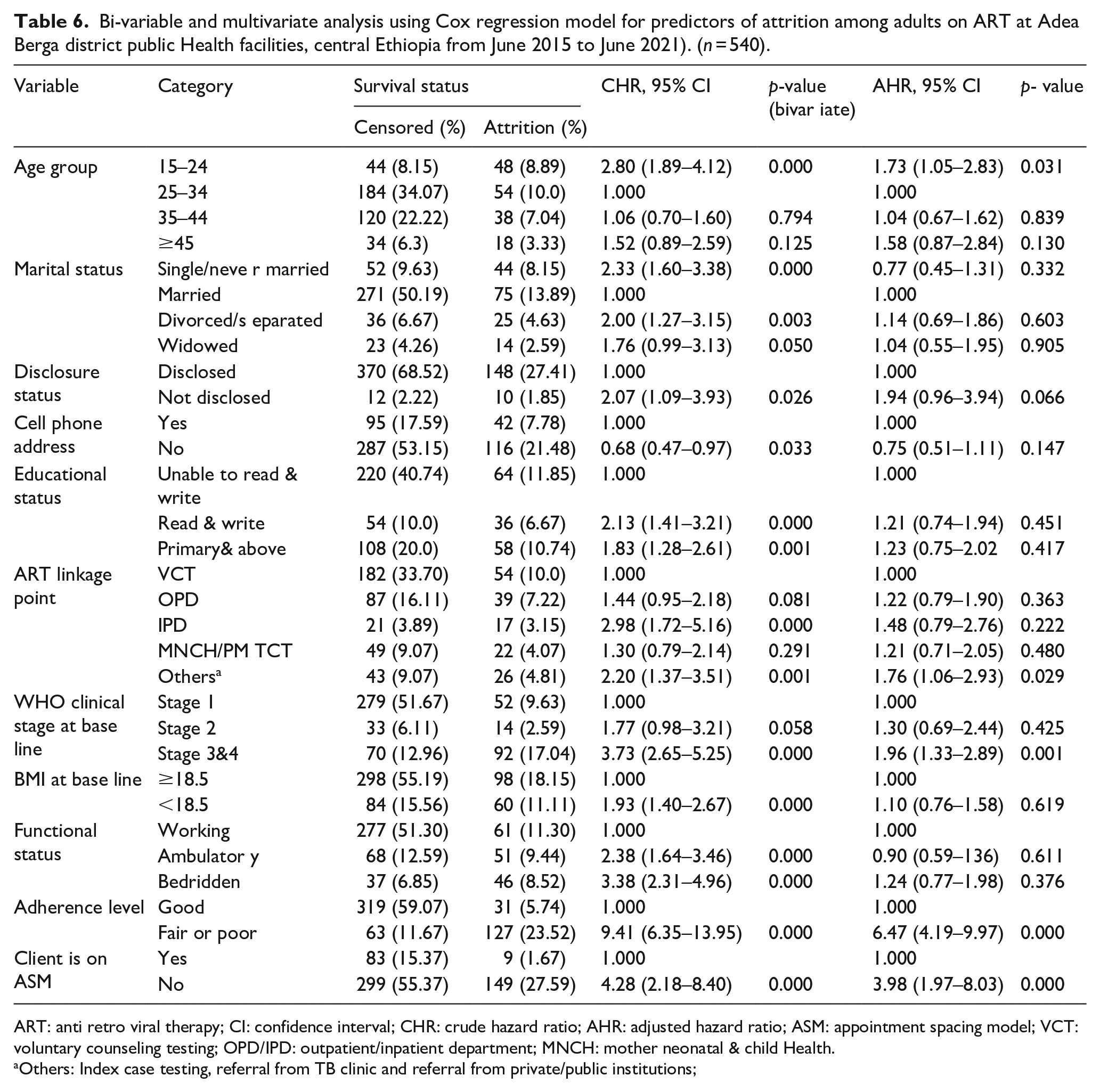
ART: anti retro viral therapy; CI: confidence interval; CHR: crude hazard ratio; AHR: adjusted hazard ratio; ASM: appointment spacing model; VCT: voluntary counseling testing; OPD/IPD: outpatient/inpatient department; MNCH: mother neonatal & child Health.
Others: Index case testing, referral from TB clinic and referral from private/public institutions;
The study found that respondent age was a significant predictor of attrition, with the risk of attrition among adults (15–24 years) being 1.7 (95% CI: 1.05–2.83) times higher than those with adults (25–34 years).
The risk of attrition among those with advanced WHO stages was higher as compared to early stages, in which the risk of attrition among those in stages III or IV was 2.0 (AHR = 1.96, 95% CI: 1.33–2.89) times higher as compared to those on WHO stage one. When compared to those with good adherence, the risk of attrition was 6.5 times higher in those with fair or poor adherence (AHR = 6.47, 95% CI: 4.19–9.97). Participants who did not use an appointment spacing model had a 4 (AHR = 3.98, 95% CI: 1.97–8.03) times higher risk of attrition than those who did.
Discussion
The cumulative incidence of attrition in this study was 158 (29.26%). The total time observed was found to be 19948 person-months of observation with a median follow-up time of 38 months (IQR 1–72). The overall incidence rate of attrition was estimated to be 9.50 (95% CI: 8.13–11.11) per 100 person-years (PY) or 0.79 (95% CI: 0.68–0.93) per 100 person-months. Moreover, the Cox proportional hazard model (multivariate analysis) showed that age group, ART linkage point, WHO clinical stage, poor/fair ART adherence level, and appointment spacing model non-user regimen were found to be significant predictors of attrition at the 5% significance level (p-value < 0.05).
In this study at least 1 month missed appointment is considered as attrition and the overall incidence rate of attrition was estimated to be 9.50 per 100 person-years (PY). This finding was lower as compared to studies conducted in Kenya (23.1/100 PY), India (14.1/100 PY), and Zimbabwe (11.8/100 PY). 16 This result was also lower when compared to studies conducted at Ethiopia’s University of Gondar Specialized Hospital (12.26/100 PY), Adama Medical College (19.2/100PY), Mettu Karl Hospital (17/100PY), Pawi Town in Benishangul Gumuz (11.6/100PY)5,17 –19). The reason for the lower attrition rate in this study might be a difference in the study participants included in the study. This might also be due to the practice of ASM implementation in the current study compared with the previous one, which was conducted before WHO recommendations for the ASM model and ongoing active tracing of clients who had missed their appointments by case managers, data clerks, and adherence supporters. It might result from the current rapid expansion and availability of potent antiretroviral treatment (ART). 10 The attrition rate was higher in Wodia town (8.36/100 PY) than in other Ethiopian studies; Debre Markos (3.7/100 PY).12,20 This high attrition rate might be due to the rapid scale-up of ART services without considering the package of care offered to clients and the absence of community-based ART services. This might be due to not including death as an attrition factor, as in the case of Debre Markos.
In this study, the risk of attrition among those with advanced WHO stages was higher as compared to early stages, in which the risk of attrition among those on III or IV was two times higher as compared to those on WHO stage one. This finding was in line with those at WHO clinical stage III or IV, with studies in Zimbabwe (2.06); Pawi in Benishan gul Gumuz (2.01).16,19 The possible explanation might be the late enrollment of individuals in HIV care at advanced stages (stage III or IV) and referral of complicated cases to the hospital, which leads to a higher risk of mortality.12,21 This finding was also lower when compared to studies conducted in Woldia, Ethiopia, among WHO clinical stages III or IV (3.6). However, finding was also higher when compared to studies done in Zimbabwe (AHR = 0.74), Kenya (AHR = 0.232), and Adama (AHR = 0.42),.5,12,22,23 Patients with advanced WHO clinical stages III or IV also underwent more attrition from the treatment as compared to those in stage I. Early HIV diagnosis and initiation of treatment could increase survival rates; this might be due to the “Test and Treat” approach. My findings confirmed the importance of initiating treatment immediately after the diagnoses recommended in the recently published study. 2018. 10
In this study, the risk of attrition among those with suboptimal (fair or poor) adherence was 6.5(AHR = 6.47, 95% CI: 4.19–9.97) as compared to those with good adherence. This finding was consistent with studies in Gonder (6.33), 17 and higher among poor adherence Woldia (AHR = 3.2) and fair adherence Woldia (1.9). 12 Clients might be discontinued their lifelong ART treatment due to social stigma, delivery problems due to long distances, forgetting and feeling better, the burden of pills with the presence of opportunistic infection, and a religious factor (holy water), resulting in a high viral load, treatment failure, and an increased likelihood of contracting OIs, and they would have died. Furthermore, substance use might be the cause of this high hazard of attrition. 17
The study found that respondent age was a significant predictor of attrition, with the risk of attrition among adults (15–24 years) being 1.7 times higher than that among adults (25–34 years). This finding was revealed elsewhere in previous studies conducted among the age group of 15–24 years in Woldia Town. 12 This high risk of attrition is higher when compared to studies conducted in Zimbabwe (1.19) and could be attributed to a high loss to follow-up as a result of stigma and discrimination, as well as a lack of psychosocial support during a health facility visit to pick up ART medication, and Zimbabwe.16,22 This could be due to social stigma, the fact that they forgot and felt better, the fact that they are naturally sexually active in this age group, the burden of pills with the presence of opportunistic infection, or the religious factor (holy water), which resulted in a high viral load, treatment failure, and an increased likelihood of contracting OIs, and they would have died. Furthermore, this high hazard of attrition might be due to substance use. 17
Participants who did not use the appointment spacing model had a fourfold higher risk of attrition than those who used the appointment spacing model. This might be due to the fact that continuing to provide ART to a large and growing number of individuals poses a significant challenge to health systems in resource-limited setups where there is a shortage of clinical staff. The challenge is highlighted by substantial rates of attrition reported across ART programs. 10 This could also be due to severe illness caused by opportunistic infections, social stigma, and delivery and travel issues caused by long distances.
The risk of attrition among those with an ART linkage point was higher as compared to VCT, in which the risk of attrition among those from index case testing, those referred from TB clinics, and those from private and public health institutions was 1.8 (AHR = 1.76, 95% CI, 1.06–2.93) times higher as compared to those from VCT. This could be due to social stigma, delivery issues due to long distances, forgetting and feeling better, the burden of pills with the presence of opportunistic infection, or a religious factor (holy water), which resulted in a high viral load, treatment failure, and an increased likelihood of contracting OIs, and then they died. 10
Limitation and strength of the study
Limitation
Since the study was conducted using secondary data (chart review), some variables that might be possible predictors of attrition, such as clinical and laboratory baseline data, were excluded due to a missed value so that it would not affect the finding. So, this might have created a selection bias. The study does not include information on socioeconomic factors like income and others which might be significant predictors of attrition due to incomplete data on the charts. Medical records that were not available during the data collection period were also excluded from the study and may underestimate or overestimate the results of the study. Another limitation of the study was that variables like mental illness were not considered as a predictor variable. The literature for the variable appointment spacing model and the ART linkage point was not obtained for the study. Additionally, the study relied on self-reported data from patients, such as medication adherence and appointment attendance, which may be subject to recall bias or social desirability bias.
Strength
The strength of the study was the consideration of censored observations. since it compares chart review with SMART care in the data clerk room. It excludes transfer outs because they did not know the patient or client’s outcome status, whether alive or attrition.
Conclussion
The result of this study showed that the incidence of attrition among adults receiving antiretroviral therapy was high. However, as a standard, every client who started antiretroviral therapy should be retained. The main positive predictors of attrition were age groups (15–24), ART linkage point, advanced WHO clinical stage, poor/fair ART adherence level, and appointment-spacing model non-users.
Supplemental Material
sj-docx-1-phj-10.1177_22799036231197194 – Supplemental material for Incidence and predictors of attrition among adults receiving first line anti-retroviral therapy at public health facility in Adea Berga district, Oromia, Ethiopia
Supplemental material, sj-docx-1-phj-10.1177_22799036231197194 for Incidence and predictors of attrition among adults receiving first line anti-retroviral therapy at public health facility in Adea Berga district, Oromia, Ethiopia by Seifu Kassa, Tariku Dingeta, Tesfaye Gobana and Tadesse Dufera in Journal of Public Health Research
Footnotes
Acknowledgements
We would like to thank Haramaya University, the College of Health and Medical Sciences, and the School of Graduate Studies for allowing us to do this research. Moreover, we would like to thank the participants of this study, the data collectors, and the supervisors.
Author contributions
S.K., T.D., and T.G. were all involved in the research concept, design, data collection, analysis, and interpretation. T.D. drafted the manuscript, and all authors reviewed and contributed intellectual content. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences, Haramaya University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.