
Abstract
Background:
Drugstores are preferred patients’ channels of contact when getting minor ailments. Given the hike in both the prevalence and severity of influenza and acute childhood diarrhea, the role, and performances of pharmacy staff should be examined.
Design and methods:
A team of pharmacy students was voluntarily recruited and trained to play the role of simulated customer visiting 228 chosen community pharmacies in six districts in Can Tho city. This process is conducted from 2021 to 2022.
Results:
The study reveals detailed information about symptoms is the most common inquiry (99.2% in scenario 1). The consulting quality is poor, 85% of instances recorded to have no medical guidelines for influenza circumstances. Meanwhile, nearly four-fifths of pharmacists provide instructions on dosage intake. It is also found that length of services is statistically different between influenza and watery diarrhea (p < 0.05, CI = 95%).
Conclusions:
Clinical practices of community pharmacists, overall, are disappointing and far below expectations.
Three questions-and-answers
- What do we already know about this topic?—The actual performances of community pharmacists are of poor quality, particularly in developing economies. However, drugstores are commonly the first point of entry among local residents.
- How does your research contribute to the field?—By using simulated customers technique, the authors examine the skills of staff at local pharmacies in Can Tho city, Vietnam. It is evidently revealed that they fail to manage minor infectious diseases in children (i.e. influenza and acute diarrhea). Under half of the dispensers offer Oral Rehydrating Salts (ORS) for patients with watery diarrhea without being asked.
- What are your research’s implications toward theory, practice, or policy?—More multifaceted collaborations are necessary in order to enhance the skill level and confidence of drug sellers. Also, the importance of ORS seems to be underrated in dealing with diarrhea.
Introduction
Community pharmacists are supposed to play a crucial role in monitoring children’s healthcare. Such a problem surprisingly hard hits lower- and middle-income countries.1–6 Vietnam, a Southeast Asian developing country, locates wholly in tropical rainforest climate, which is an ideal environment for the growth of infectious factors. Influenza, also known as the flu, is a highly contagious respiratory illness caused by influenza viruses. 7 It is a serious public health threat in Vietnam, where the population is particularly vulnerable due to its high levels of poverty and poor access to healthcare. The epidemiology of influenza in Vietnam is complex, due to its large population size, diverse climate, and its geographic location near other countries in the region.8,9 Acute diarrhea, as defined by the World Health Organization, is the passing of loose or watery stools three times or more per day, or more often than normal. It is frequently a sign of a gastrointestinal infection, which can be caused by a variety of bacteria, viruses, and parasites. Acute diarrhea is a frequent childhood illness that, if not properly treated, can result in dehydration, electrolyte imbalance, and a significantly high risk of mortality. 10 Consequently, the involvement of the primary health care practitioner is vital. Removal of formerly prescription-only medications from the list of over-the-counter drugs (OTC switch) and the preference of individuals to assume greater responsibility for their own well-being trigger more and more people self-diagnose and self-prescribe.11,12 This dilemma emphasizes the importance of community pharmacists in drug retail establishments, as this is where individuals frequently go when dealing with minor health issues. 13 In cases of mild diarrhea with no signs of toxicity, clinical pharmacists should follow the treatment guidelines of the Ministry of Health by dispensing oral rehydration salts (ORS) or advice on resuscitation for children at home. However, the practical interventions of pharmaceutical retailers still have many limitations, such as an absence of initiative; a lack of confidence in the amount and quality of information transmitted; low levels of effectiveness in counseling; and do not meet the requirements for knowledge enhancement.14–17
Accordingly, the primary aim of this study is to examine the actual practices of community pharmacists in Can Tho city, Vietnam regarding acute watery diarrhea and seasonal influenza from May 2021 to April 2022.
Methods
Study design and settings
Descriptive cross-sectional research was conducted in six districts in Can Tho city (four urban and two rural, the central region in the Mekong Delta River area with a total population of more than 1.25 million (in 2021). As aforementioned, we set goals to explore and emphasize the actual clinical practices of pharmacy dispensers. To be specific, we look at their three skills: making inquiries, counseling, and providing instructions to customers. In this research, the simulated client technique is employed.
Simulated client methodology, in which buyers simulated a seemingly real situation in order to evaluate services provided.18,19 It is an internationally recognized method for assessing the professional performance of community pharmacists. 20 Some drawbacks include high revenues originating from the data-gathering process in addition to variations in the assessment (different test purchasers and different interactions in between). A team of simulated patients (SPs), or mystery shoppers, were mostly undergraduates from our institution. Participant recruitment strictly complied with the principles of voluntarism and anonymity. Their conversations with pharmacy personnel were audio-recorded to mitigate memory inaccuracies and only used for scientific purposes.
The customer portrayed a caregiver of a 5-year-old boy, who entered a drug retail outlet in search of some medicines. The high incidence of common colds or influenza (scenario 1) and acute diarrhea (scenario 2) among children in Southwest Vietnam and its considerable connection with both household self-medication. The following information would be provided in case the sellers asked (outlined in Table 1):
Prepared scripts for two scenario.

Sampling
The overall number of community pharmacies (CPs) (630) in Can Tho city was provided by the Can Tho Department of Health.
According to the formula below (equation (1), the minimum required sample size for this analysis is n = 94. Nevertheless, in order to maximize the generalizability of the results, eventually, the authors decided to take a sample of 120 and 108 subjects, respectively.
With n = number of necessarily required sample size:

d = a degree of variability (d = 0.05);
p = the anticipated percentage of CPs giving counseling to clients (p1 = 0.412, p2 = 0.42; two domestic published article was taken into account prior to choosing this p-value); a confidence interval of 95% (corresponding to a Z-score of 1.96).
In each chosen district, the authors randomly selected 20 drugstores for scenario 1 and 18 drugstores for scenario 2. There were 228 local pharmacies being sampled in total.
Data analysis and quality assurance
The independent sample t-test enables us to compare the means between two categorical variables (with significance at p < 0.05).
Statistical Package for Social Sciences (SPSS) version 20.0 together with Microsoft Excel 2013 was adopted to interpret data. Throughout the data synthesizing progress, our team verified them for validity, then cleaned them by cross-checking. Subsequently, the outcomes were summarized in descriptive statistic tables (shown in percentages and frequencies).
Previously, the visiting procedure, transcripts of the presentation of symptoms, and planned replies to certain pharmacy employee questions have been documented. The SP team piloted 10 drugstores, which were not on the list of targeted ones with the aim of training and standardizing two scenarios to mitigate any potential biases and mistakes. Certain sensitive data will be encoded. The subject of the research is unaware of the activities of the simulated customers.
Inclusion and exclusion criteria
Drug stores, which are not GPP-certified, and hospital pharmacies, are both discarded from the study. Neither do those belonging to pharmaceutical companies nor public medical facilities fall under our scope.
Patient and public involvement
A team of Pharmacy students at our institution was voluntarily recruited and trained to play the role of simulated customers in accordance with the abovementioned contexts. The students were all informed about the protocol and purposes of the research and agreed to participate.
Due to the nature of simulated patient technique, the pharmacy staff is not allowed to know about our visits and investigation.
Results
The outcomes of 228 visits indicate that over three-quarters of accessed pharmacies (75.3%) are placed along major streets or in populous areas; otherwise, only 24.7% have geographical locations within a suburban neighborhood or local market. 208 (91.2%) of the visits occur in an independent pharmacy, whereas chained ones make up 20 (8.8%) in aggregate. Plus, there is an evident gender disparity among dispensary personnel, in which females dominates male counterparts (78.9% vs 21.1%). A different pattern is witnessed in the overall time of each purchase with approximately 33.6% of visits taking no longer than 3 min, which is just half of those with a registered time of more than 3 min. Half of valid interactions (50.9%) take place in conditions when the quantity of dispensers is at least equal to that of clients. Last but not least, approximately three-fifths of the interviewed staff (137 out of 228) are predicted to be younger than 40. Interestingly, age category, quantity of sellers and service time are indicated to be statistically different among categories (p < 0.05, 95% CI) (shown in Table 2).
Demographic characteristics of questioned outlets and respondent staff.

Scenario 2 slightly outweighs the first one in terms of inquiries taken (Figure 1). Further details about physical conditions (age and weight) show the fairly equivalent proportions of question asked between the two circumstances (from 90% and over for age and around 50% for weight). Nevertheless, inquiries about the presence of concurrent symptoms witness a stark difference, in which the figure for the influenza nearly reached 100% (99.2%), and are nearly quadrupled the diarrhea context (26.4%). There are no community pharmacists posing questions concerning drug allergic reactions in both situations and only 2.8% asked about underlying diseases of the diarrhea patients. Meanwhile, questions regarding symptoms onset were encountered only 10% and 27.8%, respectively.

Percentages of information inquired by community pharmacists in two contexts.
Figure 2 displays the percentages of sellers giving consultant recommendations to clients. Quantities of sales employees referring patients for an appointment with doctors are disappointingly low, with under 2.5% visits. Some professional suggestions were recorded in just one scenario. Also, there is 13.3% dietary adjustment recommendations for the simulated child getting influenza-like symptoms, even that of diarrhea 6.9%. By contrast, almost 80% of dispensers give instruction on dosage and duration (77.5% and 79.6%, respectively). Lastly, alertness on side effect is recorded in one visit.
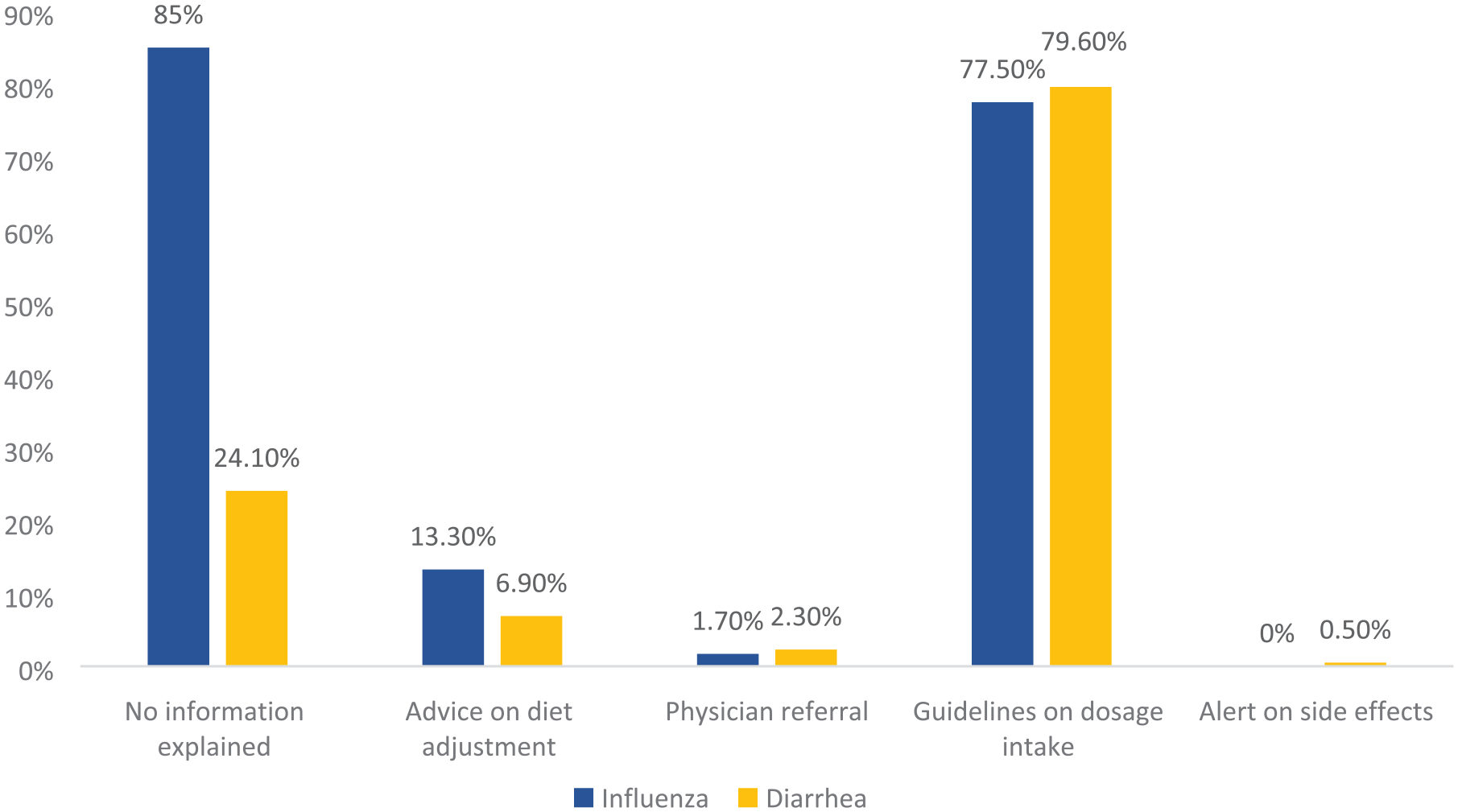
Percentage of professional counseling and explanatory statements (B) in both scenarios.
In terms of ORS category, the authors registered approximately one-fifth (20.8%) pharmacy staff dispense ORS products without demand, whereas over half of them (54.6%) denied to offer despite being asked for (Figure 3).

Percentages of community pharmacists providing ORS products in diarrhea in two circumstances.
Discussion
Theoretically, it is believed that community pharmacies have become the first point of contact for Vietnamese residents with the public health system, necessitating a focus on pharmacists’ clinical competence. Overall findings discover just a negligible number of sales personnel (1.7%–2.3%) manage to refer the SPs to visit physicians for an official prescription, which is seven times lower than in Khartoum, Sudan, 18 and east Indonesia (7%–19%). 21 Also, the history of medications used is only asked in 0.8% and 1.9% in the two contexts, respectively. The results are far worse than studies in German (32.7%) 22 and Iraq (80%), 23 relatively similar to Thailand, 24 but higher than Turkey (0%). However, the rates of requesting details about concomitant symptoms (40.8%–99.2%) are better than in Sudan (around 25%–30%). 18 Plus, information about monitoring side effects was surprisingly low (about 0%), which is far under Gonzar, Ethiopia (59.1%). 25
The results of ORS dispension is nearly 50%, which is pretty much higher than Ethiopia 25 and Pakistan. 26 The findings of counseling quality are poor, which is comparable to Qatar, 2 and Saudi Arabia. 27
Limitations
This study is conducted in merely a city which may bring conflicts arising from cultural bias and other personal issues. Therefore, the conclusion should not be generalized to other populations. We only make evaluations based on two scenarios with common questionnaires as they can not be comprehensive enough. Besides, our estimates may be conservative and did not consider the potential error.
Conclusion
A cross-sectional investigation utilizing simulated patient method was done to uncover routine operations of community pharmacists in Can Tho, Vietnam 2021–2022. There is an urgent need for multifaceted cooperation of administrative authorities, healthcare providers as well as local residents to improve daily practices of pharmacy personnel.28–30
When it comes to medical consultant recommendations, the number of pharmacists recommending a doctor visit was notably low. They failed to meet the requirements to manage childhood seasonal influenza and watery diarrhea inside the local community. Specifically, figures for information inquiry as well as making consultation are disappointing and far below average. More efforts and collaboration should be made to enhance performances.
Footnotes
Acknowledgements
The authors are grateful of Can Tho University of Medicine and Pharmacy, Can Tho city, Vietnam. Without their persistent support, this work could not complete.
Authors’ contribution
Conceptualization: Hung NP, Huong VTM; Methodology: Hung NP, Thuy NP; Data synthesizing, analyzing, and interpreting: Hung NP, Thuy NP, Minh NTT; Project administration: Hung NP; Validating: Huong VTM; Writing-original draft: Thuy NP; Reviewing and editing: Hung NP, Thuy NP, Huong VTN, Minh NTT.
Availability of data and materials
All data used in this paper is collected by Dr. Phuc Hung Nguyen.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and informed consent to participants
Our research was done following the guidelines presented in the Declaration of Helsinki. The study protocol was approved by the Medical Ethics Council of Can Tho University of Medicine and Pharmacy, Vietnam (approval number 325/HDDD-PCT).
Consent for publication
We the undersigned declare that this manuscript is original, has not been published before, and is not currently being considered for publication elsewhere. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We understand that the Corresponding Author is the sole contact for the Editorial process. She is responsible for communicating with the other authors about progress, submissions of revisions, and final approval of proofs.