
Abstract
One in five Barbadians has diabetes, suggesting that there is a severe burden of the disease.
Objective:
To assess the psychometric properties of the Diabetes Distress Scale, in order to determine the feasibility, practicality, internal consistency and criterion validity of the instrument when used with Barbadians living with Type 2 Diabetes.
Methods:
Patients with type 2 diabetes, (n = 106. 60% females, 40% males; mean age = 65.2, 11.3 years) attending a private clinic in Barbados were assessed for diabetes distress, depression, glycated hemoglobin (HbA1C) and blood pressure (BP).
A self-report questionnaire that included: clinical and demographic questions; the Diabetes Distress Scale (DDS); the Patient Health Questionnaire (PHQ-9); and the Problem Areas In Diabetes (PAID-5) scale. Glycated haemaglobin (HbA1C) and Blood pressure (BP) were also measured.
Results:
Of the 110 persons who participated, 106 persons completed the questionnaire. The Cronbach alpha coefficient of the PAID was 0.92 and the DDS was 0.92. Concurrent validity was demonstrated in a strong consistent relationship between the scores on the DDS and PAID-5, with a strong positive correlation, r = 0.70, n = 86, p < 0.001. There was a significant difference in the DDS scores between males (M = 1.26, SD = 0.37) and females (M = 1.50, SD = 0.73), t(73.31) = −1.99, p = 0.05 two tailed.
Conclusion:
The DDS is shown to be a valid and reliable measure within this Caribbean context. Thus, researchers and clinicians desirous of a tool to assess Diabetes Distress may be assured of the strong psychometric properties demonstrated thus far.
Introduction
Estimates from the International Diabetes Federation indicate that about 10% of adults in the Caribbean have diabetes, and that for Barbados, the prevalence of diabetes in adults 20–79 years was reported to be 14.8% in 2014. 1 Moreover, some persons with diabetes may also be suffering from co-existing psychological issues such as depression and diabetes distress, along with the compounding issue of co-morbidity.
Diabetes is notably one of the most psychologically challenging chronic illnesses, demanding lifestyle changes and education as well as a consistent awareness and adherence to medical regimens on the part of the patient. 2 Persons with diabetes often feel challenged by their disease and its daily demands. This heavy psychological toll can often affect self-care behavior and ultimately, lead to long-term complications.
In Barbados, incidences of such long term complications as lower extremity amputations, are considered to be among the highest in the world. 3 Further, self-management behaviors are often determined by psychological variables such as depression; through direct effects on the brain functions or indirectly through functional impairment, or decreased quality of life, and can often be stronger predictors than physiologic measures, in the prediction of such outcomes as hospitalizations and mortality. 4
Though depression has been shown to affect diabetes treatment outcome, and self-management behavior, existing evidence points more specifically to diabetes distress as a major factor associated with treatment outcomes. Diabetes distress (DD) refers to the “significant negative psychological reactions that are specific to the diagnosis of diabetes, the potential or actual complications, self-management burdens, difficult patient provider relationships and problematic interpersonal relationships.” 4
Diabetes related distress, a relatively recent concept, has been identified as conceptually and empirically distinct from depressive symptoms that accompany diabetes. Cross-sectional studies have indicated that similar to depressive symptoms, DD is associated with concurrent diabetes self-management,5,6 glycemic control5–7 and treatment adherence. 8
Due to the demanding nature of diabetes, individuals with diabetes and affective disorders, in comparison to persons with diabetes only, have increased functional impairment, increased risk of diabetic related complications, increased risk of early mortality, decreased medication adherence and decreased adherence with diabetes therapeutic regimens. 9 Identification of these psychological variables, may reduce such incidences through improvements in treatment.
Though studies have shown that interventions can improve diabetes therapeutic outcomes, 10 these are generally subsequent to the contextual understanding of the factors involved in the phenomena. In light of the prevalence of diabetes in Barbados, and limited knowledge of the nature and extent of certain types of psychopathy 11 it seems necessary to explore those factors that contribute to excess risk, in order to address the problems related to diabetes, as well as to inform probable future interventions.
The purpose of this study was to conduct a preliminary pilot test to determine the study’s feasibility, practicality and instrument internal consistency and criterion validity.
Design and methods
This pilot was conducted in order to test the feasibility of employing, the procedures, and use of instruments and equipment with a Barbadian population from August to September 2017. The sample of participants were recruited from a single facility using convenience sampling. Persons similar to the intended population (persons diagnosed with Type 2 diabetes between the ages of 20 and 80 years), were recruited within a private physician’s practice waiting room (as this was centrally located with a broad demographic) and invited to participate in the pilot. Individuals were provided information about the study and their consent obtained prior to the collection of quantitative and biological data.
Measures were taken to safeguard the participants while ensuring the research was ethically sound. Approval was granted by the Institutional Review Board of The University of The West Indies. All participants were informed of the minimal risks involved and provided assurance of anonymity.
For this study, quantitative data was collected using self report instruments in addition to biological measures, HbA1c and BP. A questionnaire battery was administered which included questions on patient characteristics (demographic information, clinical characteristics) in addition to, four short validated instruments, which included: the DDS used to measure diabetes distress and the PHQ-9 to measure depression. Also, HbA1c levels and BP measures were obtained using point of care machines.
The Patient Health Questionnaire (PHQ-9), measures the severity of depression with scores of “0” (not at all) to “3” (nearly every day) being summed. The inter-rater reliability (intra-class correlation [ICC] =0.98, 95% CI [0.96, 0.99]), test-retest reliability (ρ(Sp) =0.75, p < 0.001), and internal consistency (Cronbach’s α = 0.79) of the PHQ-9 have been shown to be good.
The DDS is a 17-item measure that screens and measures emotional distress and uses a Likert scale to score each item from 1 (no problem) to 6 (a serious problem) during the last month. Mean-item scores are then calculated (DDS17). The mean correlation between the 17-item total score (DDS) and the four subscales was shown to be high (r = 0.82). Internal reliability of the DDS and the four subscales was found to be adequate (α > 0.87).
Additionally, criterion validity of the DDS was determined by conducting concurrent validation, using the short form PAID-5 scale. The PAID-5, is a psychometrically robust short-form measure of diabetes-related emotional distress, demonstrates a reliability measure of cronbach alpha 0.86 (CI: 0.84–0.88). 12
To ensure that the questionnaire is comprehensible, and appropriate, and that the questions are well defined, clearly understood and presented consistently; this questionnaire battery was initially piloted for face validity via expert review by professionals in the field.
Further, participants were asked to offer a review, in an effort to determine whether there are any challenges with the language or items on the instrument. This process took 6 weeks to complete.
Statistical analysis were conducted using SPSS (Statistical Packages for Social Sciences) version 24.0 for Windows software. Descriptive and frequency statistics were calculated. Pearson product moment correlation coefficient was calculated to determine criterion validity. Independent samples t-test was conducted to compare the Diabetes Distress and depression scores for males and females.
Results
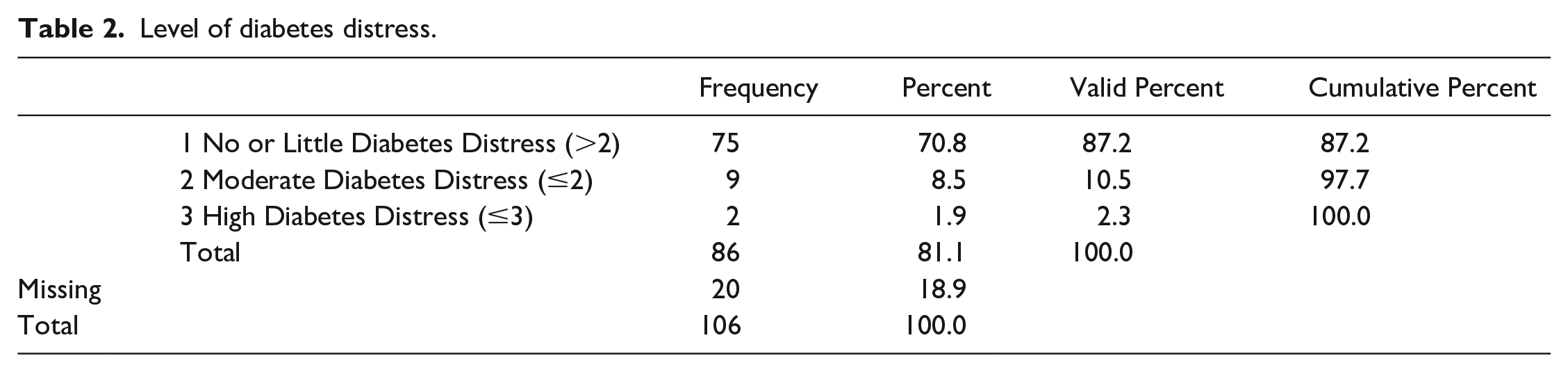
One hundred and six persons diagnosed with type 2 diabetes between the ages of 20 and 80 years completed the questionnaire (mean = 65.2, SD = 11.3), 42 males; 64 females. Participants’ mean age was 65.2 ± 11.3 years. The mean number of medications used by participants was two. 55% were married,2.8% legally separated, 28.3% never been married, 7.5%divorced, 6.6% widowed, 41% worked in the last 12 months; 45% retired, 2% with a job not working, 5% home duties, 1% student and 2% incapacitated. 1% reported amputations, 2% had kidney disease, 10% reported having a stroke, 18% reported having kidney disease, 12% had heart failure, 59% had high cholesterol. 36% knew their A1C levels. The median (interquartile range) scores for the DDS and the PHQ-9 were 1.18 (0) and 1.0 (4) respectively. Only 8.5% of participants reported moderate distress and 1.9% reported high diabetes distress. See Tables 1 and 2 respectively.
Level of depression.

Level of diabetes distress.
To determine the criterion validity of the DDS, an examination of the extent to which the DDS a relatively recent scale) is as good as the already established measure; the PAID-5 (criterion measure) was investigated using Pearson product Moment correlation coefficient and Spearman’s Rank Order correlation. The analysis showed that there was a strong positive correlation between the two scales r = 0.70, n = 86, p < 0.001.
According to Polonsky et al., 6 the DDS has satisfactory internal consistency, with a Cronbach alpha coefficient reported of 0.87. In the current study, the Cronbach alpha coefficient was 0.92. The results are also similar to other validation studies. Table 3.
Diabetes distress validation by country.

Cronbach alpha Coefficients.
Patients with poor glycemic control (as determined by an HbA1C of ≥7.1% or 53 mmol/mol) had significantly higher diabetic distress in the total score and on the subscales of emotional burden and regimen-related distress, than patients with good glycemic control (HbA1C≤7%or 53 mmol/mol).Table 4.
Diabetes distress and levels of glycemic control.
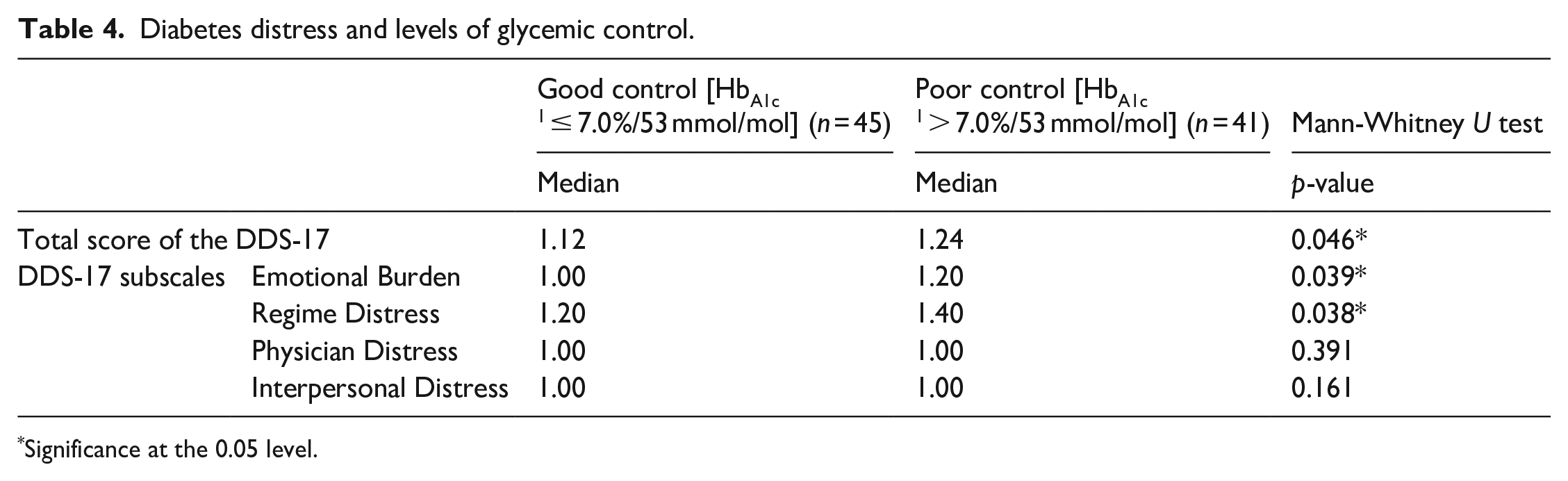
Significance at the 0.05 level.
An independent samples t-test conducted to compare the Depression (PHQ-9) scores for males and females found that; there was no significant difference in scores for males (M = 2.55, SD = 2.90) and females (M = 3.20, SD = 4.66, t(96.40) = −0.86, p = 0.39 two tailed). The magnitude of the difference in the means (mean difference = −0.65, 95% CI: −21.6 to 0.86) was small (eta squared = 0.01)
An independent samples t-test conducted to compare the Diabetes Distress Scores for males and females, found that; there was a significant difference in scores for males (M = 1.26, SD = 0.37) and females (M = 1.50, SD = 0.73; t(73.3) = −1.99, p = 0.05, two tailed). The magnitude of the difference in the means (mean difference = −0.242, 95% CI: −4.8 to 0.) was small (eta squared = 0.05).
Discussion
In an attempt to determine the psychometric properties of the DDS within a Caribbean context, the current study demonstrated an adequate internal consistency similar to results attained in other studies.13–19 Additionally, the face validity via expert review by professionals in the field, determined that the instrument was appropriate without any notable alterations, while participants offered positive comment on the ease and clarity of the questionnaire.
Since the findings of this study also demonstrated that the DDS is a valid and reliable tool in the assessment of diabetes distress, as it was able to distinguish persons with differing emotional states; it is therefore a suitable instrument for the identification and assessment of diabetes distress within the Barbadian population. This study to our knowledge is the first to validate the Diabetes Distress Scale in a Barbadian population.
For persons with diabetes, co morbid depression can have consequential effects on disease control, quality of life and cost of healthcare. This study indicated that about 21.7% of the participants with diabetes reported experiencing some degree of depression, from minimal as determined by a PHQ-9 score of 5–9 to severe (20 or higher). Depression is noted to be common in persons with type 2 Diabetes, and this may be a psychosocial consequence of the patients’ concern with having diabetes.
Contrary to the results of a systematic review, indicating that depression was higher in males than in females. 20 This study showed that in this sample there was no difference in depression between males or females. Since physical, mental and emotional wellbeing are often influenced by cultural context, the different setting therefore in which the reviewed studies were conducted, may account for this difference.
Though in the current study the mean scores for both males and females are indicative of no distress (≤2), this study showed that the mean diabetes distress scores were greater in females than in males. The latter finding was notably similar to other studies, notwithstanding that the scores demonstrated moderate distress in the sample, that females had higher diabetes distress than males.21,22 Again context may explain the observed difference, while homogeneity in the sample proportions (60% female) may qualify the similitude.
Strengths and limitations
The generalizability of these results is limited by the sample size of this pilot study, in addition, the fact that the sample of participants were recruited from a single facility using convenience sampling may not be representative of the wider Barbadian population of persons with type 2 diabetes. Moreover, the nature of this study does not permit the determination of causality of the observations made. Further research with larger samples may be needed to provide comprehensive understanding of these psychosocial variables.
Conclusion
Despite this limitation, this study adds to the validity and the use of the Diabetes Distress Scale in another setting, along with those studies conducted in other countries. As the DDS is brief and easy to administer, it serves as a valuable tool in identifying patients experiencing high levels of distress linked to their diabetes. Although the data set may be insufficient for a full understanding of the psychosocial behaviors, the DDS is shown to be a valid and reliable measure within this Caribbean context.
Footnotes
Acknowledgements
The authors would like to thank Professor Ian Hambleton for his contribution to statistical considerations, as well as the staff of the Endocrine Centre for their patience and support in the data collection process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was supported by The School for Graduate Studies and Research, The University of the West Indies, Cave Hill Campus.
Significance for public health
This study indicates the effective use and validity of the Diabetes Distress Scale in the Caribbean context. The study supports the innovative use in the Barbadian population, as this instrument offers clinicians, patients and other health care providers an additional effective tool for the management and care kit of this challenging disease.