
Abstract
Introduction
There is evidence of the relationship between psychosocial distress and elevated blood glucose levels. However, data in the Dominican Republic is limited. The study aims to measure the prevalence of four types of psychosocial distress, assess their associations with A1c levels and stratify these associations by gender among rural Dominican adults with diabetes.
Methods
Between June-July 2023, 501 diabetes patients participated in a cross-sectional survey measuring psychosocial distress (e.g., diabetes distress, depressive symptoms, acute stress, anxiety). Descriptive analyses were conducted to determine prevalence of psychosocial distress, linear regression was run on psychosocial distress and A1c levels, and logistic regression was run to examine psychosocial distress levels by gender.
Results
Participants reported mild-to-moderate levels of psychosocial distress. Almost a fifth of participants reported high levels of depressive symptoms (20.2%) and acute stress (22.0%). Only diabetes distress was significantly associated with A1c levels (b = 0.037, SE = 0.009, p = 0.001). Men were significantly less likely to report moderate-to-severe depressive symptoms (OR:2.35; CI:1.51–3.66), anxiety (OR:3.07; CI:1.52–6.19), and acute stress (OR:2.13; CI:1.51–3.66) than women.
Conclusion
Prevalence of psychosocial distress varies by type, and severity varies by gender. Diabetes distress is associated with diabetes outcomes. Findings highlight the importance of addressing psychological distress and mental health in the context of diabetes care.
Purpose
Type 2 diabetes mellitus (T2DM) is a chronic condition caused by insufficient insulin production by the pancreas and resistance to the effect of insulin in the body (World Health Organization, 2023). T2DM is characterized by hyperglycemia, or raised blood glucose, and when not managed can lead to health complications such as coronary artery disease, stroke, vision loss, nephropathy, neuropathy, and amputations (Goyal et al., 2023). These health outcomes are linked to increased morbidity and mortality, and can require advanced and expensive medical care (Mayo Clinic, 2023).
The World Health Organization estimates that 442 million people live with diabetes globally, of which 95% is T2DM (World Health Organization, 2023). According to the Global Burden of Disease Study, approximately 6.3% of the world's population lives with T2DM (Khan et al., 2020). The Dominican Republic, a Caribbean country, is experiencing increasing burden of chronic, noncommunicable diseases such as T2DM (Armora Langoni et al., 2025), a shared occurrence across many countries in the region. An estimated 10–12% of Dominican adults have T2DM (Soto et al., 2025). T2DM is the eighth top cause of death in the Dominican Republic, and is a risk factor for heart disease, the top cause of death in the country (World Health Organization, 2024). Despite the significant proportion of adults living with T2DM, there are several structural barriers to access appropriate care. Specifically, the Dominican Republic is a country with some of the highest medical out-of-pocket costs across Latin America and the Caribbean, making costs a barrier to managing conditions such as T2DM (Wallace et al., 2023). Additionally, diabetes care is typically concentrated in major urban centers in the country, thus individuals living in rural areas experience disproportionately poor access to diabetes-related care (Castro et al., 2018).
In general for adults living with T2DM, management of elevated blood glucose levels includes taking medications, such as metformin or insulin injections, and other medications to manage co-occurring conditions such as high blood pressure and high cholesterol (World Health Organization, 2023). In addition to biomedical interventions, other management strategies include regular check-ups with medical practitioners (i.e., physicians, nutritionists, diabetes educators, pharmacists), self-monitoring of blood glucose levels, adapting dietary behaviors, and engaging in more or different forms of physical activity (NIDDK, 2023).
The ability of adults to manage T2DM is influenced by psychosocial distress (Chima et al., 2021; Ehrmann et al., 2024). Psychosocial distress is defined broadly as the tendency to experience stress, negative events, and a general negative outlook on life (Henderson et al., 2013), and encompasses various psychosocial experiences such as depressive symptoms, stress, and anxiety – all of which are associated with poorer T2DM management (Chlebowy et al., 2019). For example, studies conducted in the United States (US) among Latino adults with T2DM found that depressive symptoms were associated with worse glycemic control and increased mortality (Cardenas et al., 2017; Colon et al., 2013; Leyva et al., 2011). In a study of older Puerto Rican adults, T2DM prevalence was significantly higher among adults with major depression compared to adults without major depression (POR = 1.59, p < 0.001) (Disdier-Flores, 2010). Acute (i.e., short-term) and chronic (i.e., long-term) forms of stress are both associated with hormonal and behavioral changes, which each can affect glucose levels (Dungan et al., 2009; Kyrou & Tsigos, 2009; Sharma & Singh, 2020). In a study with US Latinos, including Dominicans, chronic stress was associated with higher prevalence of diabetes [OR = 1.20, (95%CI: 1.11–1.31)], and acute stress was associated with changes in adaptive behaviors such as engagement in smoking [OR = 1.03 (95%CI: 1.01–1.19)] (Gallo et al., 2014). Anxiety is also associated with poor metabolic outcomes for those with T2DM (Bickett & Tapp, 2016). Metanalyses with data primarily from the US and Europe, have found that diabetes is associated with anxiety disorders and elevated anxiety symptoms [pooled OR = 1.22, (95%CI: 1.11–1.32)] (Smith et al., 2013). Fewer data are available on anxiety, particularly among Latin American and Caribbean populations.
While depressive symptoms, anxiety, and acute stress are general forms of psychosocial distress that are associated with T2DM outcomes there are, however, forms of distress that account for the specificity of living with T2DM. Specifically, diabetes distress refers to the medical, social, and psychological challenges with managing diabetes (Polonsky et al., 2005; Verdecias et al., 2023). It is estimated that 30–50% of people living with diabetes experience diabetes distress (CDC, 2024). Studies have found strong evidence of the association between diabetes distress and poor self-management (Emery et al., 2022), increased diabetes-related complications (Bruno et al., 2019), elevated hemoglobin A1c (A1c) (Hendrieckx et al., 2021), poorer engagement in medication adherence (Hessler et al., 2017), poor dietary quality, and reduced likelihood of physical activity (Bruno et al., 2019). Prior qualitative studies have shown that the emotional burden of managing T2DM is present for adults in rural Dominican Republic. This prior qualitative work highlighted that the manifestation of diabetes distress can vary based on gender with women reporting experiencing depressive symptoms, stress, and anxiety more often than men (Gonzalez Rodriguez et al., 2018). In addition, the availability of social support in and outside of the home, consistent engagement with medical care, and availability of recommended foods all influenced feelings of diabetes distress, which can vary by gender (Gonzalez Rodriguez et al., 2018; Wallace et al., 2019).
As understanding of the role of psychosocial distress for adults managing T2DM in the Caribbean is limited, we aimed to provide data to address that gap. Our primary aims were to first, measure the prevalence of four different types of psychosocial distress, specifically diabetes distress, depressive symptoms, anxiety, and acute stress, among Dominican adults with T2DM residing in rural areas. Second, to assess the association of each psychosocial distress measure with A1c levels among our Dominican sample and finally stratify these associations by gender. Findings will highlight areas to target for future programs aimed at improving quality of life for adults living with diabetes in similar contexts.
Methods
The study design employed was a cross-sectional quantitative study in which all data collection occurred at one timepoint. This study was informed by results of previous qualitative studies conducted in these Dominican communities and with our ILAC-CCI partners. Since 2015, our research team has conducted qualitative studies exploring social support (Wallace et al., 2019), stress (Gonzalez Rodriguez et al., 2018), scoping strategies (Sadeghzadeh et al., 2021), and provider experiences of providing emotional support to program participants (Wallace, Núñez et al., 2022).
Research team members from the university (DDW, QBN, TA, KH, RD) are bilingual (Spanish and English), of Latin American descent, and were trained in informed consent, the survey tool, and data quality assurance before the start of data collection. Research team members resided in the participating communities throughout the data collection period. All materials were written in Spanish by the first author. This study was approved by the UNC Institutional Review Board (#23–0568).
Depressive Symptoms. We used the Center for Epidemiologic Studies Depression 10-item Scale (CESD-10). Studies have found that the CESD-10 is acceptably reliable (alpha >0.80) and valid for Spanish-speaking populations, including those from the Dominican Republic (González et al., 2020). Items include “I was bothered by things that usually don’t bother me,” “I felt that everything I did was an effort,” and “I was happy.” Responses range from (1) rarely or none of the time, to (4) all of the time. We assessed two levels of depressive symptoms with scores under 10 indicating moderate depressive symptoms, and scores 10 or higher as greater severity of symptoms (Björgvinsson et al., 2013). For this study, the omega coefficient value is 0.72.
Anxiety. We used the Generalized Anxiety Disorder 7-item Scale (GAD-7). The GAD-7 is highly utilized in Latin America and the Caribbean, and studies have demonstrated consistently high reliability (omega coefficient >0.91) and validity across Spanish-speaking populations, including the Dominican Republic (López et al., 2025a, 2025b). Items include “feeling nervous, anxious or on edge,” and “trouble relaxing.” Responses range from (0) not at all to (3) nearly every day. Scores range from 0–4 (minimal anxiety), 5–9 (mild anxiety), 10–14 (moderate anxiety), and ≥15 (severe anxiety) (Spitzer et al., 2006). The omega coefficient for the GAD-7 is 0.66 for this study.
Acute Stress. We used the Perceived Stress 4-item Scale (PSS-4) measuring acute stress in the last month. Reliability and validity across populations, including in Latin America and the Caribbean, are well reported for the PSS (Vallejo et al., 2018). Reliability scores are acceptable (alpha >0.70, omega >0.75), and construct validity is high for English and Spanish speakers (Baik et al., 2019; Ruisoto et al., 2020). Items include “how often have you felt that you were unable to control the important things in your life?” and “how often have you felt confident about your ability to handle your personal problems?” Responses range from (0) never to (4) very often. Mean stress scores ≥6 classify as high levels of stress (Ingram et al., 2016). The omega coefficient for the PSS-4 is 0.60.
Diabetes Distress. The Diabetes Distress 19-item Scale (DDS-19) was adapted for use in the Dominican Republic (Wallace, Pereira et al., 2022). The DDS has been used in multiple Spanish-speaking countries and regions including Spain, Mexico, South America, and among Spanish-speakers in the US (Martinez-Vega et al., 2016; Peña-Purcell et al., 2019; Duarte-Díaz et al., 2022). The adapted DDS-19 is comprised of four subdomains: emotional distress, interpersonal distress, physician distress, and regimen distress. Items included “feeling angry, scared, and/or depressed when I think about living with diabetes” and “feeling that friends or family don’t give me the emotional support that I would like.” Responses ranged from (1) not a problem to (5) a very serious problem. Mean scores of 2–2.9 or higher indicate moderate distress, and scores of 3 or higher indicate high level of distress (Fisher et al., 2012). The omega coefficient for the DDS-19 in the study is 0.60.
Biomedical and Health Measures. We collected information on the most recently recorded hemoglobin A1c (A1c) and blood pressure (i.e., systolic and diastolic). A1c is a measure of average blood sugar levels over the previous three months (American Diabetes Association Professional Practice Committee, 2024). Below 5.7% is normal, 5.7–6.4% is elevated blood glucose (i.e., prediabetes), and 6.5% and higher indicates diabetes mellitus (Cheng et al., 2011). All A1c measures were collected using a National Glycohemoglobin Standardization Program certified device. We recorded self-reported use of cholesterol medication, alcohol, and tobacco use.
Demographics. We collected age, gender, highest level of education completed (in years), number of adults in the household, number of children or adolescents in the household, marital status, and years since diabetes diagnosis.
We conducted linear regression to determine the unadjusted association between psychosocial distress measures and A1c. We ran age-adjusted linear models to account for age, the greatest risk factor for T2DM, and logistic regression for the level of diabetes distress, acute stress, depressive symptoms, and anxiety levels between minimal compared to moderate-to-severe forms of distress. This analysis was stratified by gender to quantitively examine patterns reported in prior qualitative studies (Gonzalez Rodriguez et al., 2018; Wallace et al., 2019).
Results
Participant Demographics.
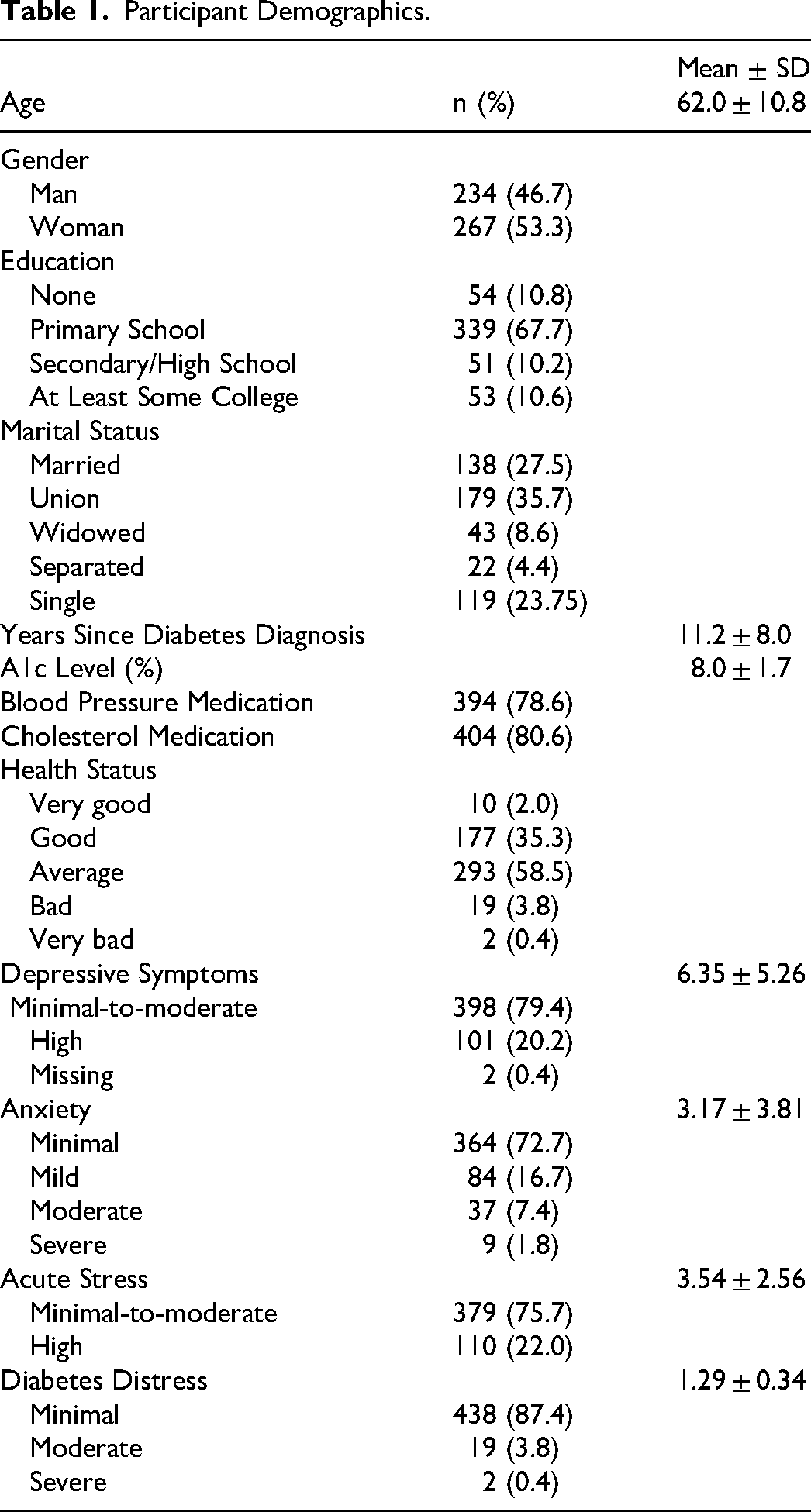
Participants self-reported living with T2DM for an average of 11 years and mean A1c levels of 8.0 ± 1.7 (range: 4.8–14.0%). Most participants self-reported blood pressure medication use (78.6%) and cholesterol medication use (80.6%) and described their health status as average (58.8%).
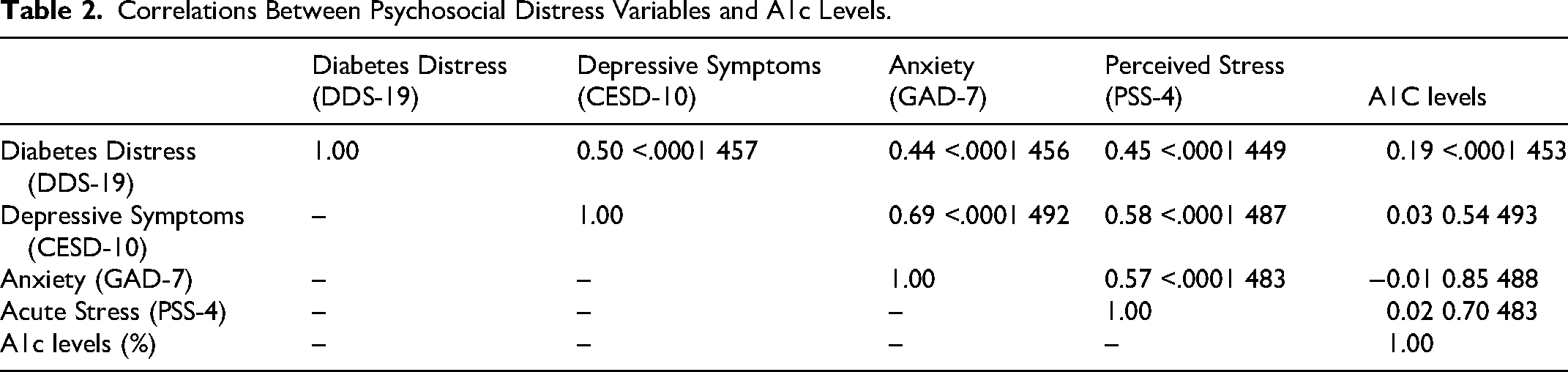
Correlations of Psychosocial Distress Measures. All forms of psychosocial distress (diabetes distress, depressive symptoms, anxiety, acute stress) were significantly correlated with one another; but not multicollinear, suggesting that psychosocial distress variables are related yet distinct (Table 2). Correlation values ranged from 0.44–0.69 and each psychosocial distress measure was statistically significant at less than 0.001. Each distress variable was evaluated against clinical A1c levels, and only diabetes distress was significantly correlated with A1c (r = 0.19; p < 0.001).
Correlations Between Psychosocial Distress Variables and A1c Levels.
Associations Between Psychosocial Distress Measures and A1c.
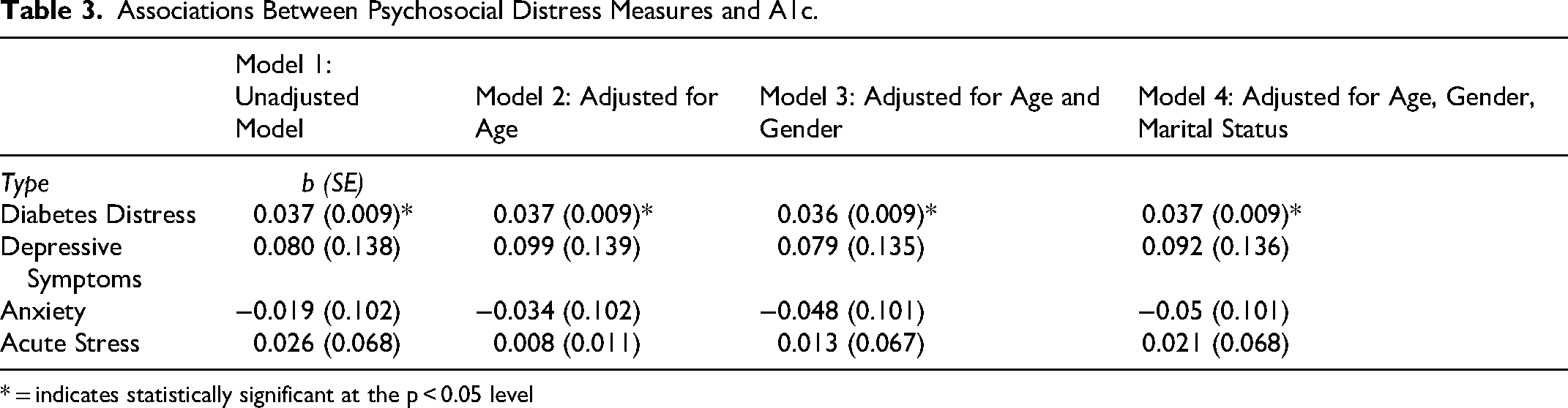
* = indicates statistically significant at the p < 0.05 level
In the analyses stratified by gender, A1c levels were not statistically different between women (mean=8.06%) and men (mean=7.85%). Diabetes distress was minimal for 95% of both women and men. A significantly greater proportion of women indicated high levels of anxiety than men; specifically, for moderate and severe levels of anxiety (13.31% versus 4.76%, p < .05). Twice as many women than men scored at moderate-to-severe depressive symptoms (30.08% versus 15.45%, p < 0.05). A similar pattern was observed for women compared to men when examining reported high levels of acute stress (28.46% versus 15.74%, p < 0.05).
We examined diabetes distress variables across gender. Overall, men reported less diabetes distress than women. There was no difference in the likelihood of men or women reporting minimal diabetes distress compared to moderate-to-severe distress. When compared to women, men were 2.13 times more likely to report minimal acute stress than moderate-to-severe acute stress (OR: 2.13; CI: 1.36–3.33). Similarly, men were 2.35 times more likely to report minimal depressive symptoms than moderate-to-severe depressive symptoms than women (OR: 2.35; CI: 1.51–3.66). Finally, men were over three times more likely to report minimal levels of anxiety than moderate-to-severe levels of anxiety than women (OR: 3.07; CI: 1.52–6.19). In the adjusted models, there were no significant differences between men and women reporting minimal versus moderate-to-severe levels of any of the four forms of distress (Table 4).
Odds Ratios for Diabetes Distress, Acute Stress, Depressive Symptoms and Anxiety by Gender.
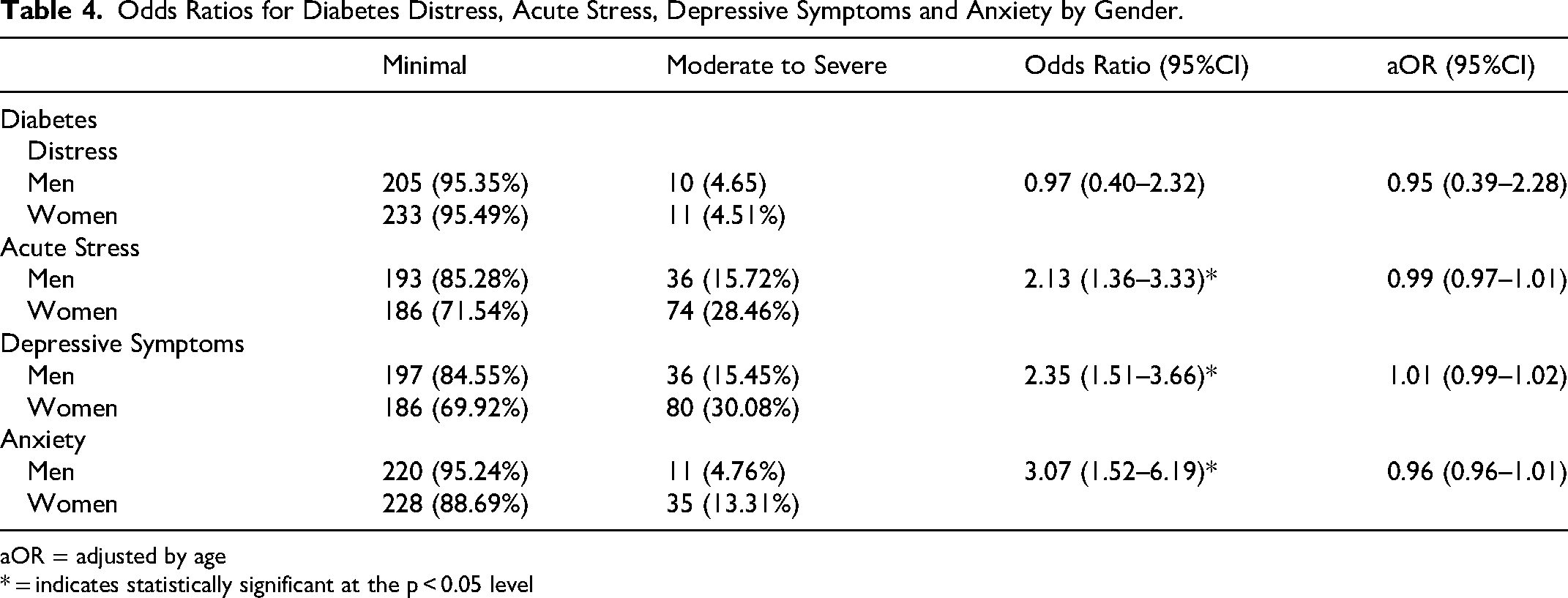
aOR = adjusted by age
* = indicates statistically significant at the p < 0.05 level
We ran adjusted odds ratios for the four diabetes distress subdomains (emotional, interpersonal, physician, regimen). For all subdomains, men were more likely to report minimal levels of distress compared to women. However, no association was significant.
Discussion
The aims of this study were to measure the prevalence of different types of psychosocial distress, and to assess the associations for each type of psychosocial distress variable with A1c levels among adults living with T2DM in the rural Dominican Republic. We further examined the associations between each form of psychosocial distress and A1c stratified these associations by gender. Overall, most participants reported minimal levels of depressive symptoms, anxiety, acute stress, and diabetes distress. The highest reported severe symptoms were depressive symptoms (20.2%) and acute stress (22.0%). Whereas participants reported low levels of severe anxiety (1.8%) and diabetes distress (0.4%). The low levels of diabetes distress may be due to all participants having consistent access to diabetes-specific care.
Almost one-fifth of participants in our study (20.2%) reported high levels of depressive symptoms, which is in line with other published studies (Aschner et al., 2021). A review of T2DM in the rural US noted that for adults with depression, medication non-adherence was higher among rural Latino patients than urban Latino patients (Dugani et al., 2021). Clinically significant depression is present in one in four people with T2DM and studies have found that depression increases the risk of hyperglycemia, insulin resistance, and diabetes-related complications (Semenkovich et al., 2015). Although we did not find an association between depressive symptom severity and A1c, studies have shown that living with T2DM increases the risk of depression and can contribute to more severe depression (Mukherjee & Chaturvedi, 2019; Semenkovich et al., 2015). A 2021 community-based study examining depressive symptoms and incident T2DM among 30,360 adults, reported that elevated depressive symptoms using the Patient Health Questionnaire 9 (PHQ-9) was associated with a 17% increased risk of T2DM (Graham et al., 2021). The study also found that a diagnosis of depression was associated with a 20% increased risk of T2DM (Graham et al., 2021). In our study the proportion of women reporting moderate-to-severe depressive symptoms was over double the proportion of men. This is in line with our previous qualitative work which described differences in received social support in the home between men and women, with women feeling less familial support to manage their diabetes thereby contributing to feelings of depression (Wallace et al., 2019). Our results reflect studies noting gender differences related to depression and diabetes among US Latinos (Mansyur et al., 2016, 2021), in Mexico (Agudelo-Botero et al., 2022), Puerto Rico (Bell et al., 2017), and in countries in South America (Aschner et al., 2021).
We also found that women endorsed higher levels of anxiety symptoms than men. Research on the role of anxiety on diabetes management is limited, particularly in Latin America. While studies have shown that anxiety is associated with diabetes (Wilczynska et al., 2022), a Multi-ethnic Study of Atherosclerosis (MESA) study examining the association between anxiety and incident T2DM found that anxiety did not predict T2DM (Abraham et al., 2015). Participants in a 2018 qualitative study in the Dominican Republic explained that they experience “ansiedad para comer” or the desire to eat when they are anxious (Gonzalez Rodriguez et al., 2018). Further, they contrasted anxiety with depression, which they tied to feelings of ennui and a lack of appetite. Additional studies are needed to better understand how anxiety affects diabetes management among Latin American and the Caribbean adults.
Our study examined acute stress and found that approximately 22% of participants endorsed experiencing moderate-to-severe levels of acute stress, although acute stress was not associated with A1c levels. Different forms of stress can produce different behaviors. Findings from Gallo et al. (2014) suggested that acute stress was associated with higher smoking behaviors but chronic—or long-term stress—was associated with heart disease, stroke, and diabetes risk among US Latinos (Gallo et al., 2014).
Despite the high proportion of minimal diabetes distress, when examining associations and psychosocial distress and A1c, only diabetes distress was associated with higher blood glucose levels. Studies among primarily Puerto Ricans in the US showed that compared to depressive symptoms, reductions in diabetes distress were associated with a clinically significant reduction in A1c levels (m = 0.55%, SD = 0.06%) (Leyva et al., 2011).This suggests that there are health implications for adults, regardless of gender, with T2DM even at minimal-to-moderate levels of diabetes distress. When examining the subdomains of diabetes distress, interpersonal and emotional distress were the most endorsed by participants. The association between diabetes distress and A1c has been noted in other studies. A 2018 study in the United Kingdom reported that regimen-related distress was the strongest predictor of glycemic control measured by A1c (Martinez et al., 2018).
There are several implications of this study for research and practice. There has been a rising consensus among researchers and health providers on the need to address emotional and mental health to improve diabetes outcomes (Matlock et al., 2024). Results of this study may support clinical practice by informing ways to integrate individualized and tailored conversations between providers and patients. For example, clinics can integrate psychosocial measures to gain a better understanding of the emotional and mental health of their diabetes patients and adjust diabetes management conversations around the relevant forms of psychosocial distress. At clinical and community levels, evidence of psychosocial distress can support health education efforts and coping interventions to address psychosocial distress and its impact on diabetes management. Clinically, interventions can include screening patients for psychosocial comorbidities to adequately treat them for conditions like depression, which in turn may affect management of T2DM. Community-level interventions can include the expansion of the stress modules in Diabetes Education Programs to support diabetes management that is inclusive of emotional and mental health.
Future directions of this research include additional validation studies for the adapted diabetes distress scale for use in the Dominican Republic and extend its use into other nearby Spanish-speaking Caribbean countries. As we cannot assess causality in this study, an extension of this study involves using a longitudinal cohort design to investigate to what extent psychosocial distress affects diabetes-related behaviors (i.e., diet, physical activity, medication adherence) and A1c over time. Additionally, studies are needed to parse out the mechanisms by which each type of psychosocial distress affects the biological and behavioral factors associated with A1c levels.
Study strengths include collaborating with long-standing partners to develop research questions that are relevant for public health and for clinical practice. In working with clinics, we were able to confirm diabetes status of participants. Our study is the first of its kind examining multiple forms of psychosocial distress that have been reported qualitatively among Dominican adults with diabetes in previous studies. In collaboration with the clinical team, collected data were integrated into program design to help better address psychosocial distress in this population. The limitations of the study are that we collected data at one time point and cannot assess causality. We did not collect self-reported information on anti-depression or anti-anxiety medication use, which could have provided additional and distinct measures of distress.
Conclusion
To our knowledge, this is the first study of its kind to present the prevalence of multiple types of psychosocial distress factors in a Dominican context. Among adults with T2DM in rural communities in the Dominican Republic, the most prevalent types of psychosocial distress were depressive symptoms and acute stress. Although diabetes distress was mild across most participants, diabetes distress was the only type of psychosocial distress associated with A1c level. Patient distress can be influenced by one or several types of distress, suggesting the need for clinical teams and researchers to assess clinical and psychosocial measures in tandem. While diabetes distress, acute stress, anxiety, and depressive symptoms are correlated, they are still distinct forms of distress. Noting each form of distress can support tailored and holistic conversations to support diabetes management. Further attention in public health and clinical approaches is needed to account for differences between how men and women report severity of psychosocial distress to support intervention development.
Footnotes
Acknowledgements
The authors would like to thank patient participants who shared their time with the study team. We would also like to thank the community health workers and nurses who facilitated our engagement with patients. We thank Dr. Elizabeth Walker for her feedback on the data collection instrument and process.
Ethical Approval and Consent to Participate
Ethical approval was given by the University of North Carolina at Chapel Hill Institutional Review Board (#23–0568). All participants gave full informed verbal consent to participate in the study.
Authors’ Contributions
DDW contributed to the study design, conceptualization, performed the analysis, and drafted the manuscript. KH contributed to data collection, data analysis, and writing the manuscript. QBN, TA, and RD contributed to data collection and critically reviewed the manuscript. LJE and APM provided access to the research site, feedback on recruitment of the clinics, and provided insightful feedback on the results as well as clinical significance. HD provided support for the study design and reviewed the manuscript. CB supported the conceptualization of the study and critically reviewed the manuscript. All authors read and approved of the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to participant vulnerability but are available from the corresponding author on reasonable request.