
Abstract
Background:
Nurses have to work different and often irregular shifts to provide care. This puts nurses at health risks, such as sleep impairment.
Design and methods:
The aim of this study was to test the comprehensive conceptual framework for predicting shift work sleep disorder of female nurses, we used a structural equation model analysis based on shift worker’s coping and transactional stress coping theory. This study used a cross-sectional design. We collected the data from three public hospitals and three private hospitals in South Kalimantan, Indonesia, with a total sample of 201 female shift work nurses. Data were collected from February to April 2020. We were also granted permission by the director and the head nurse of these hospitals. After obtaining the informed consent forms, we distributed the online self-report questionnaire using Google Forms. Demographic data were evaluated using descriptive statistical analysis. We used a structural equation model analysis to test the comprehensive conceptual framework for predicting shift work sleep disorder of female shift work nurses.
Results:
The model’s effectiveness in predicting factors contributing to shift work sleep disorder was confirmed by the good statistical fit indicated by the comparative fit index, root-mean-square error of approximation, incremental fit index, and Tucker Lewis Index.
Conclusions:
This study provides evidences that workload and interpersonal conflict contribute to occupational stress. Workload, interpersonal conflict, and the biological sleep clock influences shift work sleep disorder through mediators of coping strategies and stress.
Introduction
Sleep disorders (SDs) are conditions that change the usual way to sleep. They are considered a relevant public health issue because they can affect health and increase the risk of injury. Some of common SDs are insomnia (difficulty falling asleep throughout the night), sleep apnea, difficulty in breathing while sleeping), narcolepsy (extreme sleepiness during the day). 1 Shift work sleep disorder (SWSD) is a sleep impairment typified by sleepiness or insomnia due to the shift work schedule.2,3 Rotating and often irregular shifts make nurses at high risk of sleep impairment. In effect, insomnia is often experienced by nurses who work on the night shift system in comparison with nurses who work a regular shift.4–7 In addition, shift work sleep disorder among nurses is related to work accident and patient safety. 8
Women are strongly represented in the health-care sector, and the majority of nurses in hospitals are women. 9 In Indonesia, the prevalence of sleep disorders among shift work nurses is 52.50%. 10 Many of them work in hospitals and account for the largest number of health care workers compared to other health shift workers, such as physicians, nutritionists, midwives, and clinical psychologists. 11 In conclusion, female nurses with irregular shifts tend to experience high level of stress and sleep disorders related to shift due to hormonal changes. 12 In addition to the gender, shift workers’ coping with stress model showed that other factors affecting shift workers night rest include potential occupational stressors, non-occupational stressors, and personal factors, mediated by coping and stress. 13 A similar model found that SWSD was affected by the biological clock, sleep factors, and social factors. 14 However, very little theoretically based research has been conducted, particularly in a structural pathways model of the factors affecting shift work sleep disorder. We tested factors affecting shift work sleep disorder based on these models as well as coping strategies. We also highlight a new type of coping in the transactional stress called the meaning based coping. This response can promote personal growth and help nurses to find positive meaning in their caregiving experience, so it will improve the adaptive coping.15,16
The summary of the theoretical framework of factors affecting shift work sleep disorder among shift work nurses, is depicted in Figure 1. The underlying hypothesis is that selected occupational stressors, workload, interpersonal conflict, and biological sleep clock (morningness-eveningness) influence SWSD among shift work nurses through coping strategies and stress. The final aims of this study were to evaluate factors that affect SWSD and also provide a conceptual framework for implementing corrective intervention among female shift work nurses.

Factors affecting shift work sleep disorder in nurses: Tested model.
Methods
Research design
This study used a cross-sectional design to investigate the risk factors SWSD in nurses through a structural equation model.
Settings
Data were collected from February to April 2020 from three regional public hospitals and three private hospitals in South Kalimantan Province, Indonesia.
Participants
Female shift work nurses were recruited by convenience sampling. We focused on female nurses because gender influenced the circadian regulation of sleep in humans. The other inclusion criteria were: minimum 3 months working experience, a diploma degree, age ≤35 years, no history of chronic disease such as hypertension, non-pregnant, and agreement to join this study. As a reward, the participants who completed fulfill the questionnaire got a voucher (e-money for shopping).
Outcome
The study outcome was the SWSD.
Dependent variables
The study predictors were demographic variables (such as age, level of education, work experience, kind of employees, marital status, and number of children), workload, interpersonal conflict, biological sleep clock, coping, meaning-based coping, and perceived stress.
Data sources/measurement
All the study variables were measured through validated questionnaires adapted and translated into Bahasa based on World Health Organization (WHO) guidelines. 17 The permission to adapt all the questionnaires was granted by the original authors. Three questions were used to assess SWSD based on previous study. 18 It was developed based on International Classifications of Sleep Disorder, second edition 3. We also assessed physical and mental fatigue using the brief self-rated fatigue scale (FS), is 10 items self-report questionnaires, using 5-point scale (1: never to 5: always). Higher score indicates higher fatigue. 19 Perceived stress was measured by a shortened version of perceived stress scale (PSS) created by Cohen.20, 21 The short PSS consist of item 2, 4, 5, and 6 in PSS. It is rated on a 5-point Likert type scale, ranging from 0 (never) to 4 (very frequently). Scores of items 4 and 5 are reversed. Higher scores indicated higher perceived stress. According to Lazarus and Folkman’s theory, 20 we assessed Coping through emotional-focused (five items) and problem-focused (three items) domains of the Brief COPE (we did not consider the dysfunctional coping dimension). Items were scored with a 4-point scale; 1 (I have not been doing this at all) to 4 (I have been doing this lot). 20 Meaning-based coping consists of positive reinterpretation, human caring, and spiritual. Positive reappraisal was measured by using cognitive emotion regulation questionnaire (CERQ) in the related domain; this is a four-item scale to assess positive meaning to the event. Each item was scored on 1 ((almost) never) to 5 ((almost) always) Likert scale. Higher scores indicate positive reappraisal. 22 Human caring and spiritual were measured by cultural justifications for caregiving scale-revised (CJCS-R) 27. CJCS-R was used to measure caregivers’ cultural motivation in providing caring, it is a 10 items self-report questionnaire on a 4-point scale (4 strongly agree to 1 strongly disagree). We adopted this questionnaire to measure motivation among shift work nurses in providing caring, which refers to human caring. The Workload was measured by the National Aeronautics and Space Administration Task Load Index (NASA-TLX), which is a six item questionnaire for measuring mental demand, physical demand, temporal demand and frustration. The range of score was 1 (low) to 20 (High). 20 Interpersonal conflict was measured by the nursing stress scale (NSS) in the domain of conflict with physicians (five items) and with other nurses (five items) to measure stressful situations in the nurse’s interaction with physicians and with other nurses or supervisors respectively. Each item scored 0 (never), occasionally (1), frequently (2), and very frequently (3), with a high score indicating more frequent conflict. 23 We used the reduced morningness-eveningness scale (rMES) to measure biological sleep clock, especially to assess circadian variations and preference for morning or evening activities. The rMES is a shortened version of the MES (item 1, 7, 10, 18, and 19). Items 1, 10, 18 are on 1–5 point scale, item 7 is on 1–4 scales, and item 19 is on 0, 2, 4, and 6 point scales, with a high score indicating morning type. 24
Study size
The statistical indices in a structural equation model (SEM) will perform adequately when the sample size is 200 or more or five cases per free parameter in the model 16–18.25–27 We had 25 parameters, the minimum sample size was 125, but we recruited 201 nurses to prevent missing data. Previous study recommended that 60% response rate. 28 All participants were female nurses who had a shift work.
Statistical methods
All the data were keyed in the Statistical Product and Service Solutions (SPSS) computer software version 22. Univariate analysis (chi-squared test) was used to investigate the frequency of each variable and their relationship with shift work sleep disorder. Our present study evaluated the reliability and validity of the scale. The internal consistency reliability was used to calculate the Cronbach’s alpha for each questionnaire; previous studies suggest that Cronbach’s alpha >0.5 is considered acceptable reliability. In this study, we had 11 hypotheses. To estimate the hypothesized model fit with the actual data, AMOS 20.0 was used for the structural equation model. Maximum likelihood was used to estimate loadings on the effect of the variable. We determined the standardized path (β), the standard error (SE), and p-values which was significant at <0.05 was addressed to include or exclude the hypotheses. Direct, indirect, and total effects were calculated in the model using the standardized path (β). The following fit indices were used to evaluate the hypothesized model fit with the actual data: standardized chi-square index (χ2/df), root mean square error of approximation (RMSEA), goodness-of-fit indexed (GFI), comparative fit index (CFI), the Tucker-Lewis index (TLI), and incremental fit index (IFI). The standardized chisquare index (χ2/df) value of 5 or less indicated good fit. Acceptable fit values for the GFI, CFI, TLI, IFI were 0.90 or greater and the RMSEA were 0.1 or less. 29
Ethical consideration
The procedure was reviewed and granted ethical clearance (number: 1903-KEPK) by the Institutional Review Board (IRB) at Nursing Faculty, Universitas Airlangga, Indonesia.
Significance for public health
Sleep is public health issue with broad implications. Nurses have to work different and often irregular shifts to provide care. This puts nurses at health risk, such as of sleep impairment and it is considered as shift work sleep disorder. In addition, shift work sleep disorder among nurses is related to work accident and patient safety. Analysis of the factors affecting shift work sleep disorder is needed which may be considered as potential target of intervention among female shift nurses.
Results
Table 1 lists the characteristics of all participants. Our 201 participants’ mean age (standard deviation; SD) was 27.27 (3.82). Most of participants were permanent employee (87%), and had work experience more than 60 months (54.20%).
Distribution of respondent characteristics (n = 201).
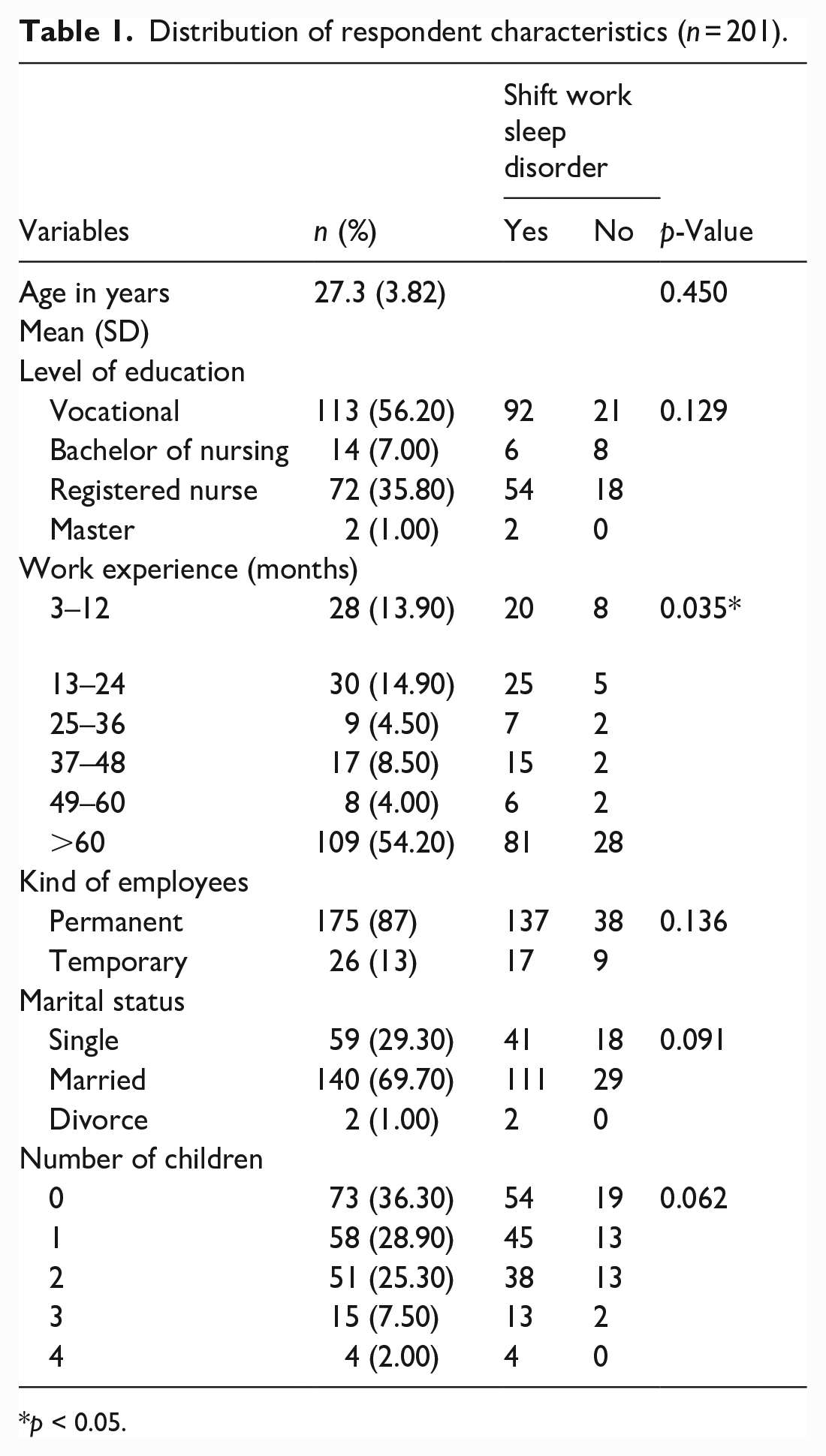
p < 0.05.
Table 2 lists scores and consistency ratings for the used scales. It consists of total item, range, mean, and standard deviation and Cronbach’s alpha for all variables. The Cronbach’s alpha of every variable addressed was acceptable. Previous studies mentioned that Cronbach’s alpha >0.5 was considered acceptable reliability30,31; thus, the scales met the structural equation model requirement.
Scores and consistency ratings for the used scales.

In this study we evaluated reliability and validity of the scale (Table 1). Our present study showed the overall SWSD and brief self-rated fatigue scale (FS) (four items) indicated fit to the data. The results of the CFA indicated GFI 0.922; AGFI 0.832; CFI 0.906; RMSEA 0.1. The Cronbach’s alpha for shift work sleep disorder 0.752. The Cronbach’s alpha of short perceived stress scale (PSS), BRIEF COPE, and meaning based coping in this study presented 0.586, 0.783, 0.822, respectively. The Cronbach’s alpha of the NASA Task Load Index (TLX) for this study was 0.840. Results of confirmatory factor analysis (CFA) indicated that only four structures showed a tolerable fit to the data. These were mental demand, physical demand, temporal demand, and frustration; the results demonstrated that goodness-of-fit indexed (GFI) 0.995; adjusted goodness-of-fit indexed (AGFI) 0.976; normed-fit index (NFI) 0.995; root mean square error of approximation (RMSEA) 0.01. We examined the reliability and validity of the nursing stress scale (NSS) to measure interpersonal conflict. Cronbach’s alpha for this study was 0.761. Results of CFA indicated that four items in the domain conflict with physicians and four items in the domain conflict with other nurses demonstrated a tolerable fit to the data; the results showed that GFI 0.927; AGFI 0.862; CFI 0.885; RMSEA 0.1. In addition, we measured the reliability of the rMES. Cronbach’s alpha for this study was 0.52.
Table 3 presented regression estimates. It reports β coefficients, SE, and the p-value. Ten paths were considered significant at p < 0.05, which are indicated by solid line and one path was non-significant at p > 0.05, which is indicated by broken line. In the model, interpersonal conflict (β = 0.392, p < 0.05; H2), workload (β = 0.647, p < 0.05; H6), biological sleep clock (β = 0.271, p < 0.05; H8), and stress (β = 0.370, p < 0.05; H11) had significantly positive path on shift work sleep disorder. Interpersonal conflict (β = −0.348, p < 0.05; H3) and biological sleep clock (β = 0.153, p < 0.05; H7) had significantly positive path on coping strategies; however coping strategies were not affected by the variable of workload (β = −0.070, p > 0.05; H5). Additionally, workload had significantly path on interpersonal conflict (β = 0.516, p < 0.05; H1). Coping strategies had significantly positive path on stress (β = −0.676, p < 0.05; H10). Meaning-based coping was affected by interpersonal conflict (β = 0.302, p < 0.05; H4) and had significantly positive effect on coping strategies (β = 0.864, p < 0.05; H9).
Regression estimates.

β: standardized regression weight.
Significant estimates at 0.05 significance level.
According to Figure 2, eleven hypotheses (H1–H11) were examined. The statistical goodness of fit of the structural model, denoted by χ2 207.775 (df = 112, p = 0.00); showed goodness-of-fit index (GFI) = 0.890, adjusted goodness-of-fit index (AGFI) = 0.850, comparative fit index (CFI) = 0.907, root-mean-square error of approximation (RMSEA) = 0.065, incremental fit index (IFI) = 0.909, Tucker Lewis Index (TLI) = 0.886, as shown in Figure 2. We had three adequacy indices that indicated the data were fit our hypothetical model.

Path diagram of the confirmatory factor analysis. Significant pathways are represented with solid lines, and the others with broken lines. “e” indicates errors.
Table 4 presented standardized total, direct, and indirect effects of the variables. It shows that workload exhibited the strongest total effect on shift work sleep disorder and performed the strongest total direct effect on shift work sleep disorder.
Standardized total, direct, and indirect effects of the variables.

Discussion
We tested the comprehensive conceptual framework for predicting shift work sleep disorder of female shift work nurses which include occupational stressors: workload and interpersonal conflict, and biological sleep clock as risk factors with coping strategies and stress as mediator; also meaning-based coping was another coping strategy to induce adaptive coping in a sample of female shift work nurses. Statistical results supported the hypothesis that risk factors influence shift work sleep disorder by mediating coping strategies and stress. Other results showed that meaning based coping positively influenced coping strategies, and workload positively influenced interpersonal conflict. Our results provided applicable evidence of the conceptual framework for predicting shift work sleep disorder among female shift work nurses.
Our findings showed that occupational stressors: workload and interpersonal conflict, biological sleep clock, and stress were predictors of shift work sleep disorder. In Table 4, our results showed that occupational stressors such as workload, caused direct effect on shift work sleep disorder. Moreover, occupational stressors: workload demonstrated to be the strongest predictor of sleep quality (β = 0.647, p < 0.05), as shown in Figure 2. Workload may be an important factor of shift work sleep disorder among female shift work nurses. This finding is consistent with previous study. 32
There are several patient-handling tasks that are considered as producing high workload among nursing, such as transferring and lifting patients and working standing, and these were related to sickness absence. 33 In this study especially in South Kalimantan, nurses on night shift also extended their working hours because they have to wait for nurses on the day shift to conduct handover. Moreover, nurses conducted irregular shifts and changed their shift with other friends in a ward, due to personal reasons, such as family. Workload can negatively affect sleep because heavy workload will decrease sleep duration.34,35
In Table 3, our results showed that occupational stressor such as interpersonal conflict were a predictor of shift work sleep disorder (β = 0.392, p < 0.05). Moreover, interpersonal conflict caused direct and indirect effect on shift work sleep disorder and also positively influenced meaning-based coping. In addition, interpersonal conflict was affected by workload, as shown in Figure 2. One of occupational stressor is interpersonal conflict. Obviously, nurses have to work with others health care profession, such as physicians, 36 and also work with supervisors and other nurses. 37
Our findings showed that biological sleep clock is a significant predictor of shift work sleep disorder (β = 0.271, p < 0.05) as shown in Figure 2. Biological sleep clock causes direct and indirect effect on shift work sleep disorder. Shift workers who spent more time at night going against their internal biological sleep clock significantly associated with shift work sleep disorder. 4
Interpersonal conflict, biological sleep clock, and meaning-based coping are significant predictors of coping strategies among female shift work nurses. Coping strategies as an approach to deal with stressors, is classified as problem-focused and emotional-focused. 38 Nurses utilized coping strategies to prevent distress and maintain health and well-being. In this study, it depicted the coping strategies utilized by female shift work nurses were acceptance (accepting the situation), positive reframing (finding meaning in stressful event), religion (praying and meditating), active coping (adopting strategies to solve problems), emotional support (getting support from others), and humor (making situations fun) to deal with stressor such as interpersonal conflict and biological sleep clock and prevent shift work sleep disorder.
Meaning-based coping strongly affects coping strategies (β = 0.864, p < 0.05), as shown in Figure 2. This finding is consistent with previous study, which mentioned that meaning-based coping might lead adaptive coping in stressful conditions. 39 Meaning based coping consists of positive reappraisal, revised goals, spiritual/acceptance, or and positive events. 40 Previous study showed that caring from nurses increased the coping style to patients, 41 meanwhile, in this study, caring increases coping style among the nurses. This result implies that meaning-based coping is needed for female shift work nurses to increase coping strategies and prevent shift work sleep disorder.
Several limitations in this study should be considered. This study used cross-sectional design; therefore, the causal direction implied by the path in structural equation model must be interpreted carefully. This study limits the generalization of the effect of occupational stressors: workload and interpersonal conflict, biological sleep clock, coping strategies and meaning based coping, and stress on shift work sleep disorder among female shift work nurses. Intervention studies are necessary to manage factors affecting shift work sleep disorder among female shift work nurses.
Conclusion
Our results supported the hypothesis that selected occupational stressors: workload and interpersonal conflict, and biological sleep clock influences shift work sleep disorder among shift work nurses through coping strategies and stress. Coping strategies significantly mediated the effect of interpersonal conflict on stress and stress significantly mediated the effect of coping strategies and shift work sleep disorder. The clinical significance of our findings is that the effect of interpersonal conflict and biological sleep clock on shift work sleep disorder may be reduced by increasing coping and stress management.
Footnotes
Acknowledgements
We would like to thank to Ulin Hospital Banjarmasin, Ansari Shaleh Hospital, and Idaman Hospital Banjarbaru, Indonesia as the research place.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from Ministry of Research and Technology/National Research and Innovation Agency Indonesia, 2021 and Universitas Lambung Mangkurat, Banjarmasin Indonesia.
Ethical
The procedure was reviewed and granted ethical clearance (number: 1903-KEPK) by the Institutional Review Board (IRB) at Nursing Faculty, Universitas Airlangga, Indonesia.