
Abstract
Background:
Overweight is a risk factor for non-communicable diseases and is affecting an increasing number of children worldwide. The objective of this study was to measure the prevalence and related factors to overweight among children under 5 years in five West African countries.
Methods:
This study was a secondary analysis of nationally representative cross-sectional data. These data were drawn from Demographic and Health Surveys (DHS) from five countries in the West African region (Benin, Guinea, Mali, Nigeria, and Togo) from 2015 to 2018.Continuous quantitative data were categorized and all analyses were weighted according to the probability that each participant was selected in the sample. Children under 5 years of age were the study population. Multilevel logistic regression was used with Stata 16.0 software.
Results:
The total sample size for the analysis was 38,657 children. The pooled prevalence of overweight among children under 5 years of age in the five countries was 3%. Guinea had the highest prevalence (6%) compared to the other countries, which had a prevalence of 2%. The likelihood of being overweight was higher among children aged 0–6 months (adjusted odds ratio [AOR] = 3.09; 95% confidence interval [CI] [2.41–3.95]), who had a high birth height (AOR = 1.64; 95% CI [1.29–2.09]), whose mothers were overweight (AOR = 1.35; 95% CI [1.09–1.68]), who lived in households with fewer than five members (AOR = 1.19; 95% CI [1.00–1.46]), or who lived in Guinea (AOR = 2.79; 95% CI [1.62–4.79]).
Conclusion:
This study showed that overweight concerns few children under 5 years of age in West Africa. However, it does exist, and its prevalence could likely increase if its modifiable factors (maternal overweight, household size, and height at birth) are not taken into account in nutritional interventions.
Background
Overweight is a public health challenge as it increases the risk of both mortality and morbidity. It is common in high-income, as well as in middle- and low-income countries. 1 According to the World Health Organization (WHO), approximately 41 million children under the age of 5 years were overweight worldwide in 2016. A quarter of these children lived in Africa. 2 It has been reported that overweight in preschool children is a sign of obesity and morbidity in adulthood, leading to chronic diseases such as heart disease, diabetes, or cancer.3,4 Without action, the prevalence of overweight in preschool children could increase from 7% to 11% by 2025. 5
In sub-Saharan Africa, studies on overweight in children under 5 years have already been conducted in Malawi in 2015 and Ethiopia in 2017, and reported that the majority of children surveyed were overweight, at 14.5% and 6.9%, respectively.6,7 In North Africa, prevalence was estimated at 14% in Morocco in 2015 and at 8.6% in Algeria in 2020.8,9
The increasing urbanization in countries, and the changes in dietary and social habits in urban areas are considered to be factors contributing to overweight in children.10,11 Various studies have also found an association between overweight and dietary diversity, maternal body mass index, and the maternal job.9,12,13
However, these studies have been conducted either on specific regions within countries or in nurseries or schools and are therefore fragmented. Such studies, although useful in their specific contexts, do not provide the overall magnitude and determinants of child overweight. In West Africa, for example, few studies are available on these indicators. The Demographic and Health Survey (DHS) databases provide an opportunity to determine the prevalence of overweight among children under 5 years of age in this region, as well as the factors contributing to the occurrence of overweight. For a region such as West Africa, the organization of health systems and health behaviors may be quite different from other regions of the continent. Therefore, having indicators at this regional level will better guide interventions to address all forms of child malnutrition in this sub-Saharan region, such as the “nutrition-friendly” schools launched in Burkina Faso and Benin to strengthen nutrition education. The malnutrition is one of the priorities of public health because developing countries suffer from many factors that make malnutrition a major cause of mortality and morbidity in this age group. Therefore, this study involved five countries in the West African sub-region (Benin, Guinea, Mali, Nigeria, and Togo) and aimed to determine the prevalence of overweight in children under 5 years of age and to identify factors associated with overweight in children under 5 years of age.
Method
Type and period of study
This was a cross-sectional study using secondary data from DHS conducted between 2015 and 2018 in five West African countries: in 2015 in Togo and in 2018 in the other four countries (Benin, Guinea, Mali, and Nigeria).
Study setting
West Africa comprises 16 countries. It had a population of 402 million in 2020, which is almost 30% of the African continent’s population, and its total area is about 6,143,000 km2. 14
The data analyzed in this study covers Benin, Guinea, Mali, Nigeria, and Togo. The choice of these countries is based on the fact that they have the most recent DHS data (conducted over the last 5 years). These countries are considered low- and middle-income countries and have a socio-economic situation marked by persistent poverty and food insecurity that negatively impacts the quality of children’s diets. 14
Specific setting
Benin covers an area of 114,763 km2, with an estimated population of over 11 million in 2018, 9% are children under 5 years of age. 15 Guinea covers an area of 245,857 km2 with a population over 10 million. The population of children aged 0–5 years was over 2 million in 2018. 16 As for Mali, it is an interland country covering an area of about 1,241,248 km2, with a population of more than 18 million in 2016. The population of children under the age of 5 years was more than 3 million. 17 Nigeria, a country of 923,768 km2, had a population over 195 million in 2016, with 18% of children under the age of 5 years. 18 Togo is located on the southern edge of West Africa; it covers an area of 56,600 km², with a population of more than 6 million in 2010 and has 90,1271 of children under the age of 5 years. 19
Study population
For this study, all West African countries were eligible, but we chose those with their recent DHS surveys, which were conducted within the last five years: Benin, Guinea, Mali, Nigeria, and Togo.
The population consisted of all children aged from 0 to 59 months in the five countries who had received anthropometric measurements during the survey.
All children who did not have anthropometric measurements at the time of data collection were excluded from this study.
Study variables
Dependent variable
The overweight. This variable was built from the weight-for-age ratio (WFA). This ratio is an index commonly used to classify nutritional status according to the 2006 WHO criteria that define the nutritional status of children under 5 years of age. 20 For this purpose, the z-score is a measure that allows to situate an overweight child in relation to its reference population. Weight-for-age z-scores in children less than 24 months and beyond 24 months were calculated with reference to the 2006 WHO growth chart. 20 Thus, all values greater than 2 were retained (z-score >+ 2) and considered as overweight (Yes = 1) and not in the opposite case (No = 0).
Independent variables
The hierarchical structure of the data led us to classify them into individual, community, and contextual variables.
– Individual variables were individual characteristics of mothers and children: children’s age in months (0–6; 7–23; and 24–59), gender (male and female), weight (<4000 and >4000 g), birth rank (1–3 and ≥4), and height at birth (small, medium, and tall), maternal years (15–24, 25–34, and 35-49), parents’ (mothers’ and fathers’), and schooling level was classified as: none, primary, and secondary/high school. Marital status, body mass index is weight in kilograms (kg) divided by height in square, so we classified it into two categories (normal weight and overweight). Parity was classified as having 1–2, 4–7, and ≥7 children and occupation (none, private/public employee, farmer/worker, and salesperson).
– Community or contextual variables were represented by socioeconomic status (very poor, poor, rich, and very rich), household size was classified as having ≤5 and >5 members in the household, number of children under the of age 5 years households ≤ 2, > 2, and countries (Guinea, Benin, Mali, Nigeria, and Togo), and area of residence (urban and rural).
Data sources
Our analysis sample comprised all children who received anthropometric measurements during the investigators’ visit to the households. The sample comprised: 12,034 in Benin, 3,429 in Guinea, 8588 in Mali, 11,400 in Nigeria, and 3206 in Togo, for a total of 38,657 children. For all these countries, the DHS sampling was nationally representative, based on a two-stage stratified cluster survey.
In Benin
The first step consisted of a draw of 555 clusters from the list of enumeration areas (EA) established during the General Census of Population and Housing (RGPH-2013). A total of 14,435 households (6528 in urban areas and 7907 in rural areas) were selected. All women aged 15–49 years living in the selected households or present on the day before the survey were eligible to be interviewed. Similarly, all women (15–49 years) and children under five were eligible for the various biological and anthropometric tests and measurements.
In Guinea
A total of 8020 households (2760 urban and 5260 rural) were selected. All women aged 15–49 years and children under 5 years of age living in the selected households, or present the day preceding the survey, were eligible to be interviewed.
In Mali
In the first stage, 379 clusters were drawn from the list of enumeration areas established during the 2009 General Population Census, using a systematic draw with probability proportional to size, the probability of the Primary Survey Unit (UPS) being the number of households. A count of households in each of these clusters provided a list of households from which a sample of 35 households per cluster was drawn in the Kidal, Gao, and Timbuktu regions and 26 households in all others, a systematic draw with equal probability. A total of 10,574 households (2992 in urban areas and 7582 in rural areas) were selected. All women aged 15–49 years usually living in the selected households or present the day preceding the survey were eligible to be surveyed. Also, all women (15–49) and children under the age of five were eligible for the various biological and anthropometric tests and measurements.
In Nigeria
Prior to sample selection, all the areas were classified separately into urban and rural areas based on predetermined minimum urban area sizes (cut-off points), with any area having a minimum population size of 20,000 being classified as urban. Stratification was performed to obtain 37 urban and rural regions. A total of 74 sampling strata were identified. In the first stage, 1400 enumeration areas were selected. The size of the enumeration areas was the number of households residing in the simple random sample. In the second selection stage, a fixed number of 30 households were selected from each household by systematic equal probability sampling, resulting in a total sample of about 42,000 household’s representatives of the entire country. Thus, all women of childbearing age (15–49 years) and children under 5 years of age were eligible for the various biological and anthropometric tests and measurements.
In Togo
At the first level, 330 Primary Survey Units or clusters were drawn from the list of enumeration areas established during the 2010 General Census of Population and Housing conducted by the General Directorate of Statistics and National Accounting. By proceeding to a systematic drawing with a probability proportional to the size, the UPS being the number of households. In a second step, a sample of 30 households per cluster was drawn systematically with probability. A total of 9899 households (3840 urban in 128 clusters and 6059 rural in 202 clusters) were selected. All women aged 15–49 years usually living in the selected households, or present the day preceding the survey, were eligible to be interviewed.
Data processing and analysis
For all analysis, STATA 16.0 software was used. After the descriptive analysis of each variable, a bivariate analysis at the overall country level was performed to estimate the association between childhood overweight and the selected variables at the individual and contextual levels by performing a simple logistic regression. For inclusion of variables in the multilevel multivariate model, a threshold of 20% (that means with a p < 0.20) was used. The choice of this threshold of significance made it possible to take into account all the variables according to the literature that could explain the final model of this study. Using a threshold of 5% would lead to the omission of important variables in the explanation of this phenomenon, which led us to widen the threshold to 20%.A multilevel binary random-effects logistic regression was performed using the bottom-up stepwise method. Adjusted odds ratios (ORs) were estimated with their p-values and confidence intervals (CIs). Successive models were compared by using the likelihood ratio test.
Using this same analytical technique, we looked for associations between overweight and variables at the individual and community level. Three statistical models were implemented:
The first model contained no independent variables. This allowed us to compare our multilevel regression model to a classical logistic model and to evaluate the variation of overweight according to the area of residence (urban and rural).
The second model was obtained after the introduction of individual level explanatory variables.
The third or full model contains, in addition to the individual level variables, the contextual level variable which is the residence setting. The intra-class correlation coefficient was calculated for each statistical model and the discriminative power of the model was calculated using Roc’s table.
A multilevel analysis was performed considering the hierarchical structure of the data.
We chose random-effects models because such an analysis allows us to distinguish the variability in overweight that exists between individual characteristics and different regions of the five countries.
Ethical Considerations
Permission to use DHS data from individual countries for this study was obtained from the DHS platform (https://dhsprogram.com).
Results
Socio-demographic characteristics of participants
A total of 38,657 children were identified in the DHS of the five countries: 1234 in Benin, 3429 in Guinea, 8588 in Mali, 1400 in Nigeria, and 3206 in Togo.
Table 1 shows that children in the 24- to 59-month age group were more represented (57%), with 51% of the children being male; the median age of the children was 28 months, with the age groups ranging from 13 to 43 years. A 9/10 of the children weighed less than 4000 g (93%). Moreover, 65% of them lived in urban areas and 41% were from the second quintile, which means poor families. More than half of the mothers had no educational background (58%). In contrast to the other four French speaking countries, Nigeria had a higher rate of mothers with secondary school or higher educational background (45%). Almost all mothers in the overall sample were in union (95%). Less than 14% of the mothers were overweight, almost half of them had a parity of between four and seven births (47%), and 62% of the children were born in households with more than five people.
Sociodemographic characteristics of participants by country.

Prevalence of overweight
Figure 1 presents the overall and country-specific prevalence of overweight among children under 5 years in West Africa. The overall prevalence was 3%. This was highest in Guinea at 6% compared to 2% in each of the other countries.

Prevalence of overweight in children under 5 years of age by country 2018.
Factors related to overweight children in all countries
Table 2 reports the results of the multilevel analysis. Individual factors independently associated with the occurrence of overweight in children were: children’s age and height at birth and mother’s body mass index. Children aged 0–6 months had a higher odd of overweight occurrence compared to those aged 7–23 months and 24 to 59 months (adjusted odds ratio [AOR] = 3.09; 95% [CI] [2.41–3.95). The odds of overweight occurrence among children with high birth heights were 1.64 times those of their peers with low birth heights (AOR = 1.64; 95% CI [1.29–2.09]). In addition, overweight mothers were 1.35 times more likely to have overweight children (AOR = 1.35; 95% CI [1.09–1.68]) compared with normal weight mothers.
Factors associated with childhood overweight across countries in multilevel analysis.
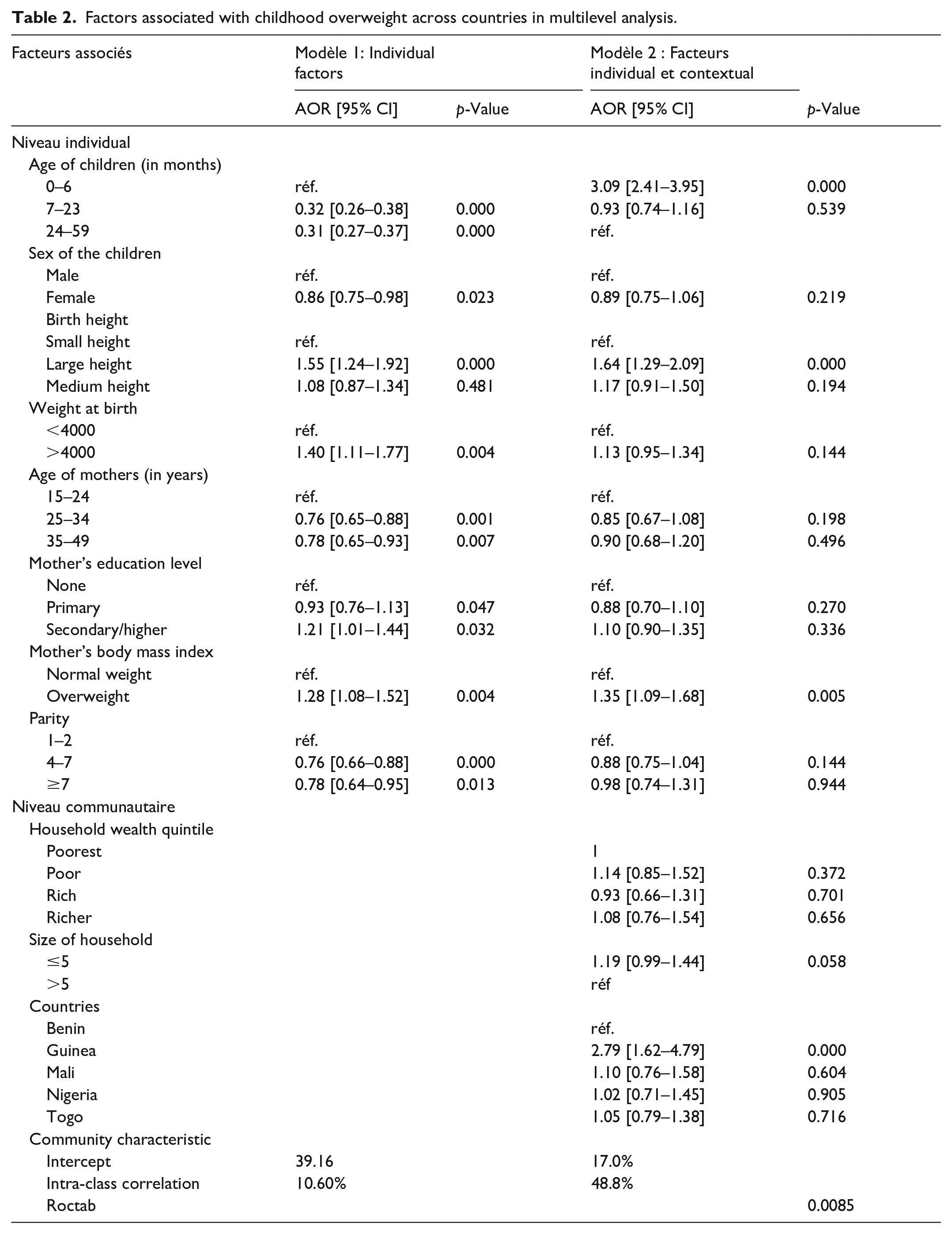
Contextual factors independently associated with the occurrence of overweight in young children were household size and country of residence. Thus, in household size, among children from households with less than five members the odds of overweight occurrence were 1.19% higher (AOR = 1.19; 95% CI [0.99–1.44]). At the country level, children in Guinea were 2.79 times more likely to be overweight (AOR = 2.76; 95% CI [1.62–4.79]) compared to children in Benin. Although not statistically significant, children in Mali (AOR = 1.10; 95% CI [0.76–1.58]), Nigeria (AOR = 1.02; 95% CI [0.71–1.45]), and Togo (AOR = 1.05; 95% CI [0.79–1.38]) were more likely to be overweight compared to children in Benin.
Discussion
The results of this study showed an overall prevalence of 3% overweight in children under 5 years of age with a higher proportion in Guinea (6%). This high prevalence in Guinea is significantly higher than average of the African continent (4.9%). This increase is contrary to the objectives of the Sustainable Development Goals, which aim to eliminate all forms of malnutrition in children. 21 It could be explained by the low level of education or information of mothers on nutritional practices in the country, both at the community level and in health facilities during prenatal and postnatal consultations, which are the right moments for mothers to adhere to good practices. Studies conducted in sub-Saharan Africa have shown that the lack of information and knowledge of mothers about nutritional practices for children has an influence on the occurrence of types of malnutrition.22,23 Our results were higher than those found in Ghana (2.4%) but lower than those in Ethiopia (13.8%) which are not among the countries participating in this study.22,24
It is therefore important to focus on information and promotion of good nutritional practices in order to improve knowledge about a rich and diversified diet that would help prevent and fight overweight; this can be done through awareness and information.
The results of this study show that beyond the individual characteristics of the participants, overweight is explained by contextual factors. The overweight is explained in 39.16% by individual characteristics and 17.00% by the community level. After adjusting individual and community characteristics, this study suggests that: age, birth size of children, maternal body mass index, and household size were significantly associated with overweight in children under the age of five in all five countries.
This study found that country of residence was significantly associated with the occurrence of overweight in children under 5 years of age. Children in Guinea were more likely to be overweight than those in Benin. This could depend on the high proportion of mothers with no educational background in our sample.
For improving this indicator, attention from the states is needed to reorient nutrition policies, implement nutrition interventions that integrate the valorization of local products and promote nutrition education specifically targeting mothers of children under the age of 5 years.
The study also found that the age of the child was statistically associated with the development of overweight. The results show that infants (0–6 months) were more likely to be overweight. The results found by this study could be the result of insufficient nutritional counseling in the dedicated services. These arguments are consistent with those found in Algeria. 8 In contrast to Algeria, other studies conducted in Ghana and Cameroon suggest that the occurrence of overweight increases with the age of the child. 25 For this component, promotion and awareness of good dietary practices could help prevent forms of malnutrition in this population. To this end, the education sector could play a key role in providing health and nutrition education, increasing opportunities for physical activity, and promoting a healthy environment.
The results of the study also showed that children who were of higher birth size were more likely to be overweight, the results showed that it is a risk factor for the occurrence of overweight. However, a comparison of these results with other studies was not found. Maternal body mass index (BMI) is also a predictor of overweight in children. While genetic and environmental predispositions may explain this, there is also the dietary habits and sedentary lifestyle of mothers. Many studies have also found this correlation between parental and child overweight.6,11,23,24,26 The authorities in these countries should place special emphasis on the promotion of good dietary practices and physical activity by creating conducive spaces in preschools and schools through awareness campaigns on their benefits for the health of the individual.
Households with less than five members were also more likely to have overweight children according to our results. This could be explained by the fact that this number allows parents to provide their children with nutrient-rich foods in sufficient quantities. Studies in sub-Saharan Africa have found similar results, namely that a small family size increases the risk of overweight children. 27 It is important that the means of regular monitoring of children’s growth in the countries’ health districts be reviewed in order to better manage this growing phenomenon.
The gender of the child, Child birth weight, maternal age, maternal education, maternal parity, household socioeconomic status, and maternal occupation were not factors associated with the development of overweight children, contrary to the literature.11,27,28 These variables were not included in the final model, as their p-values were greater than 20%.
Conclusion
This study measured the prevalence and identified the main individual and contextual factors associated with overweight in children under the age of 5 years in the five West African countries namely: Benin, Guinea, Mali, Nigeria, and Togo. They were mainly children’s age, children’s birth size, mothers’ body mass index, household size and country of residence.
The data from this study should help to adjust strategies for improving the nutritional status of children in West African countries to address the double nutritional burden (lack or excess) in the region. Interventions to prevent and control malnutrition should not only focus on malnutrition but also on overweight. The associated factors are at the individual and community level and imply the need to take them into account.
Footnotes
Acknowledgements
We thank the DHS program for approval and access to the original data.
Author contributions
Study design: RD, AB, EC, and MDB. Data analysis: SC, AD, BSC, AOT, AMS, AB, and SK. Initial drafting of the manuscript: RD, AD, SC, AMS, and BSC. Revision of the manuscript: MDB, AB, EC, and SK. The author(s) read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Strengths and limitations of the study
This study provides data for the West African region that will help inform nutrition programs aimed at combating overweight. The analysis of information was based on children born in the last 5 years prior to collection. The absence of information on parental physical activity, maternal nutritional habits and practices, dietary advice and habits received during the pre- and postnatal period, fruit consumption, and children’s leisure and sleep were limitations of our study. These variables could have improved our pattern. We were only able to use data from five countries that are recent. Thus, these five countries may not be representative of the entire region.