
Abstract
Background:
Many countries introduce CBHI as their healthcare financing system to ensure healthcare access. Understanding the level of satisfaction and factors associated with it is essential to ensure the sustainability of the program. Therefore, this study aimed to assess household satisfaction with a CBHI scheme and its associated factors in Addis Ababa.
Design and methods:
Institutional-based cross-sectional study was conducted in the 10 health centers found in the 10 sub-cities of Addis Ababa. Both quantitative and qualitative methods were used. Logistic regression analysis was carried out to identify its associated factors and thematic analysis was used for qualitative data. Finally, variables with a p-value of <0.05 have been considered statistically significant.
Results:
In this study, the overall satisfaction level of households with CBHI was 46.3%. Satisfaction was associated with valid CBHI management regulations (AOR = 1.96, 95% CI: 1.12, 3.46), participants who received the right drug (AOR = 1.77, 95% CI: 1.08, 2.93), households who got immediate care (AOR = 4.95, 95% CI: 2.72, 8.98), those who agreed with the adequacy of medical equipment (AOR = 1.65, 95% CI: 1.02, 2.69), and households who agreed with qualification of health personnel (AOR = 1.89, 95% CI: 1.12, 3.20) were more satisfied with the scheme than their counterparts. The challenges mentioned by the discussants were the shortage of drugs, poor attitude of health professionals, absence of kenema pharmacy, lack of laboratory services, lack of awareness about the CBHI scheme, and tight payment schedule.
Conclusions:
the satisfaction level of households was low. To achieve a better result, the concerned bodies should work to improve the availability of medication, and medical equipment and improve the attitude of healthcare workers.
Introduction
The financing of healthcare is a significant problem in low- and middle-income countries. 1 In these countries, the disease burden can be high and people need to pay from their pockets. 2 Quality healthcare services are only possible if you have the financial means to pay for them. 3 The lack of a reliable financing system is the primary reason that millions die each year from preventable diseases, especially in developing countries.4,5
Over 60% of countries have incomes below $1000/person. Out-of-pocket payment accounts for 40% or more of total healthcare expenditures. 6 Ethiopians spend 31% on healthcare through out-of-pocket payments. Additionally, 32% of Ethiopia’s total health spending is spent by the government, and NGO contributions account for 35% of total health spending.7,8 Ethiopia’s health financing relies on the government’s expenditure, out-of-pocket expenditures from users, and donor contributions. 9 The federal ministry of health (FMoH) reported that out-of-pocket spending has increased from 31% in 2000 to 37% in 2010. 10
Countries use different systems to finance their health systems. The systems are tax-based systems, social insurance systems, and mixed systems.11,12 The Ethiopian government seeks to address the financial disaster caused by out-of-pocket payments using social health insurance (SHI) and community-based health insurance (CBHI) in 2010/2011 G.C to provide an alternative to funding healthcare financing.13,14 SHI covers a portion of the population who is employed and receives a monthly salary while CBHI is for the part of the population who are involved in the informal economy sector 14 CBHI was initially implemented in Ethiopia’s four largest regions: Amhara, Oromia, SNNP, and Tigray in order to combat high pocket spending. 15 Latter in 2016 CBHI began to be implemented in Addis Ababa and is currently being expanded across the country. 16
It is important to ensure universal health coverage. CBHI has been adopted by many countries to provide additional funding for their healthcare systems and to ensure access to healthcare. This increases citizens’ willingness to seek care and reduces the fear of not being able to pay. 17 CBHI employs insurance principles that include resource pooling and paying a premium, sharing the risk among members, and dealing with other partners in the system to improve healthcare access, financial protection, and responsiveness.10,18 This will in turn ensure the health system remains responsive and enable the members to get quality healthcare service without creating a financial burden on them. 18
The health sector’s main objective is to make health care accessible to all, without undue hardship. In other words, universal health coverage must become Ethiopia’s goal for the future. 17 The Ethiopian Health Sector Transformation Plan (EHSTP-2) focuses on the importance to make healthcare accessible to everyone. 19 CBHI was included as part of the EHSTP-2 to provide financial risk protection and ensure universal health coverage (UHC). CBHI Ethiopia’s main features include voluntary membership at a household level; financing the poor; general and targeted subventions; benefits packages and community participation in the management of the scheme. 20 CBHI schemes are established at the woreda levels in regional states as well as the sub-city level of Addis Ababa. 21 CBHI benefits packages include all family healthcare services and curative (inpatient, outpatient, and acute illness treatment) services that are part of Ethiopia’s essential health package. 22 To remain enrolled in the program, it is important to improve a household satisfaction level with the CBHI scheme.
Household satisfaction is influenced by the following factors: members’ age, household size, laboratory services, CBHI opening times, affordability of membership, card collection, waiting time after payment, type of healthcare facility visited, and length of enrollment.4,23–25 CBHI members’ satisfaction is also associated with the factors such as service quality, friendliness of health service providers, subjective disconfirmation, client expectations, and emotions during service delivery.24–26 However, the results of these studies were inconsistent in rural settings and poorly explored in urban settings. Thus the proposed study examined the level of satisfaction and its associated factors in the urban settings of Addis Ababa. The study also highlights the main implementation challenges that the scheme faces in order to increase satisfaction.
Methods
Study area
Addis Ababa is Ethiopia’s capital and it lies at 38.763611 and 9.005401 respectively. Ethiopia’s capital has 527 km of land. According to the 2019GC 27 report of the Ethiopian statistical agency, the area covered by this capital city is 527 km2. The population is estimated to be over 3636 4,000,000. Females are more numerous than males (1,880,000 males and 2,120,000 females). The city is divided into 10 sub-cities to facilitate administrative tasks. There are 112 health facilities 3939 and 1092 private institutions at different levels of the city’s healthcare system. 28 This study examined health centers located in woredas that have adopted CBHI since 2017G.C. Forty woredas (four in each of the sub-cities) have implemented CBHI. Of these, only 10 woredas began implementation in 2017 G.C. Therefore, the study included all the 10 health centers found in each woreda, one for each sub-city.
Study design
To assess satisfaction and factors in Addis Ababa, a cross-sectional institutional study design was used. It also included qualitative and quantitative methods.
Source population
The study’s source population was all members of community-based insurance that had been in existence since 2017G.C. in Addis Ababa.
Study population
The study population was chosen from community-based health insurance members who use the CBHI service during the data collection period.
Sample size determination
The sample size was determined by using the single population proportion formula by taking all the necessary assumptions for a cross-sectional study: proportion taken from a study conducted in the Sheko district (southern part of Ethiopia) 54.7% on the satisfaction level of CBHI members, 4 95% confidence interval (CI), 5% margin of error, and adding 10% non-response rate, Therefore, using the above assumptions, the sample size was calculated as follows:

Where/P = 54.7% = 0.547

(1.96)2 × 0.54 × 0.46/(0.05)2 = 3.81.7, then by adding a 10% non-response rate the final sample size was 419.
Ten focus group discussions (FGDs) were conducted for the qualitative part. They were held in every sub-city within woredas that implement CBHI. The size of each FGD varies from 8 to 12 CBHI members. CBHI members were invited to participate in the FGD and the FGDs were guided by trained facilitators.
Sampling techniques, and other procedures
Study participants were selected using a random sampling technique. In Addis Ababa, CBHI was implemented in 10 pilot woredas located in ten city sub-cities. CBHI members who lived in these woredas were the subject of the study. Participants in the study were CBHI members from each of the woredas and used the CBHI services in their respective woredas. A proportional allocation was used to allocate the sample size to each woreda based on the CBHI beneficiaries’ monthly reports and the daily flow of clients. Systematic random sampling was used to select the study participants. The lottery method was used for the selection of the first clients. Healthcare workers were responsible for identifying and interviewing the study participants from those who visited the health centers every day.
Examine variables
Dependent variable
The dependent variable was the level of satisfaction with the pilot CBHI Scheme.
Independent variables
The socio-demographic characteristics of members
Members’ knowledge and experience about the CBHI scheme
CBHI Process and Management-related Factors and
Factors that influence the provision of healthcare services
Operational definitions
CBHI Satisfaction: Seventeen (17) satisfaction questions developed from similar previous literatures were used to assess satisfaction with the CBHI program. Participants who scored the median value and above were classified as satisfied. Participants with lower scores than the median were classed as dissatisfied.
Data collection procedures
Quantitative data were collected using a structured questionnaire that was administered with the assistance of healthcare workers. FGD was used for qualitative data. Healthcare workers conducted face-to-face interviews with CBHI members on their exit from their respective health centers using a structured questionnaire. To assess participant perceptions about the CBHI scheme’s challenges, qualitative semi-structured interview guide questions were used.
Data quality management
The questionnaire was developed based on a review of similar studies. To ensure consistency, the English version of the questionnaire was translated into the Amharic language. To make sure the questionnaire is accurate, it was pretested. As well as supervisors were trained to supervise the data collection process and to ensure data quality. The quantitative data was collected from CBHI members by using an interviewer-assisted questionnaire. The qualitative data was collected using trained qualitative data collection workers.
Data entry and analysis
Data were coded into Epi data version 3 and then exported to SPSS version 20 for analysis. The data were analyzed using descriptive and Inferential statics. Regression analysis was used for analyzing the relationship between satisfaction with different socio-demographic factors, other factors such as knowledge, experience, CBHI processes, and management-related factors.
Participants’ satisfaction was measured in terms of frequency and percentage. Bivariate analysis was used for the assessment of factors associated with the satisfaction level of households. FGDs were used to examine the major challenges of the scheme and the data were analyzed using thematic analyses using open code software.
Ethical consideration
Addis Ababa University’s Department of Health Sciences granted ethical approval. Additional ethical clearances were also obtained from all relevant bodies within their hierarchy, starting at the regional health bureau and ending at the woreda office. Before participants could participate in the study they were informed about the purpose of the study and verbal consent was obtained from all participants.
Result
Socio-demographic characteristics of study participants
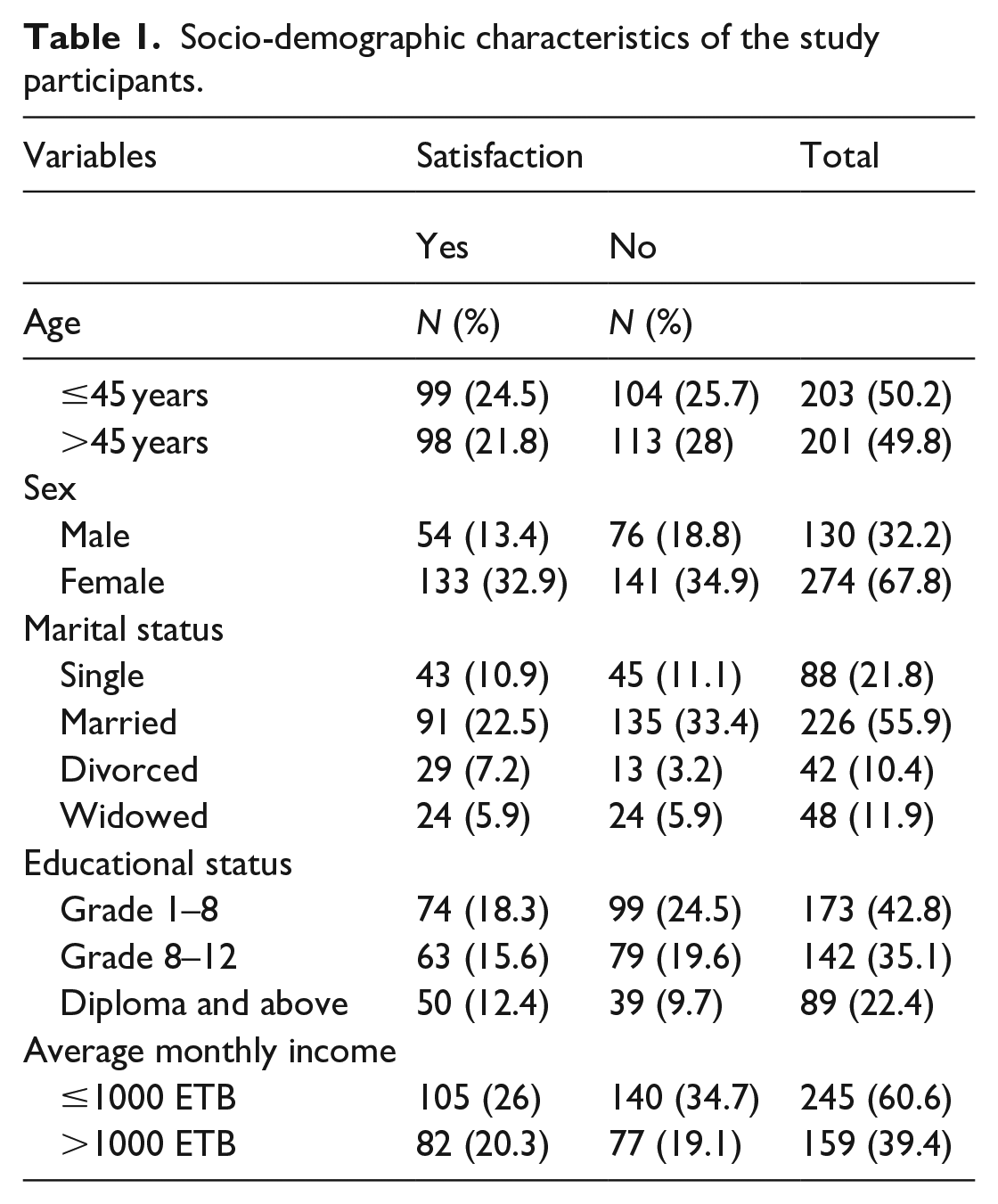
A total of 404 study participants were enrolled in this study with a response rate of (96.4%). The majority of the study participants 274 (67.8%) were women. The mean age of the study participants is 45 years (ranging from 18 to 85 years of age) with (an Sd of ±14.38) years. Concerning marital status, the majority of the study participants 226 (55.9%) were married. Similarly, most of the study participants 245 (60.6%) have an average monthly income of above 1000 ETB. Only 89 (22.4%) of the study, participants have an educational status of diploma and above diploma level (Table 1)
Socio-demographic characteristics of the study participants.
Knowledge and experience of the study participants
Nine items were used to assess the knowledge of the study participants regarding the benefits of the CBHI package. Almost all 399 (98.8%) of the study participants were aware that CBHI is a good way of relieving CBHI members to off health expenditures. Likewise, the majority of the study participants know the benefits of the CBHI package. In this study participants who answered seven or more questions successfully from a total of nine knowledge questions are considered knowledgeable. Accordingly, 222 (55%) of the study participants have adequate knowledge about CBHI packages. All the study participants who take part in this study had an experience of visiting health institutions after enrolling in the CBHI scheme (Table 2).
Knowledge of participants about the principle of the CBHI scheme and their experience.

Level of satisfaction with the CBHI scheme
The reliability of the questions used to assess the level of satisfaction was assessed using Cronbach’s Alpha. Household satisfaction level with the CBHI scheme was assessed using 17 standardized questions. Each question used a five-point Likert scale from strongly disagree to strongly agree. The internal consistency of the 17 items tested using Cronbach’s Alpha was found to be 0.831. In this study, the median score was used to classify households as satisfied and not satisfied. Then households were categorized as satisfied if they score above the median score otherwise unsatisfied. Accordingly, the share of study participants who are satisfied with community-based health insurance was found to be 46.3%, as shown in Figure, 1 below.
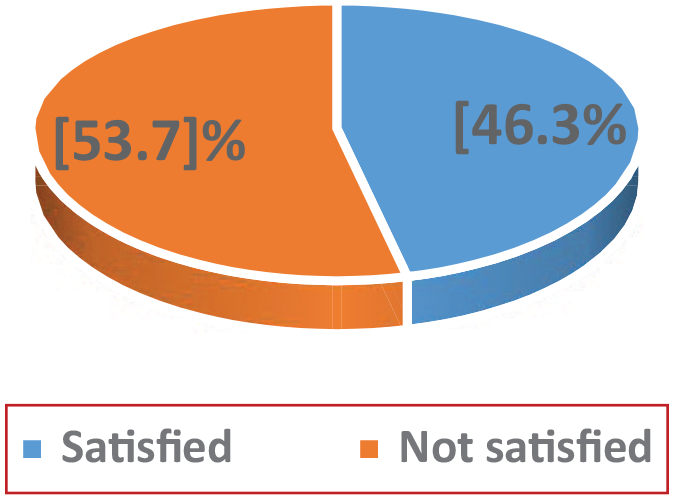
Satisfaction level of households on the CBHI scheme.
Result of multivariate analysis
Variables that have a significant association at a p-value of 20% in the simple binary logistic regression analysis were further examined in the multiple binary logistic regression analysis to control the confounding factors and to see their real association with the outcome variable. The result of the multivariate analysis showed that study participants whose age lies between 40 and 49 were 45% less likely to satisfy with the CBHI scheme compared to study participants above 50 years old (AOR = 0.55, 95% CI: 0.31, 0.96). Correspondingly, study participants who think that CBHI regulations were valid were almost 2 times more likely to satisfy with the CBHI scheme compared to their counterparts (AOR = 1.96, 95% CI: 1.12, 3.46). Households who think they got the right prescribed drug during the recent visit were 1.77 times more likely to satisfy with the CBHI scheme compared to their counterparts (AOR = 1.77, 95% CI: 1.08, 2.93). In addition, study participants who got immediate care during health facility visits were almost 5 times more likely to satisfy with the CBHI program (AOR = 4.95, 95% CI: 2.72, 8.98). Households who believed that the permitted public health facilities have adequate medical equipment were 1.65 times more likely to satisfy with the CBHI program compared to their counterparts (AOR = 1.65, 95% CI: 1.02, 2.69). Likewise, households who believed that the permitted public health facilities have adequate qualified health personnel were 1.89 times more likely to satisfy by the program compared to their counterparts (AOR = 1.89, 95% CI:1.12, 3.20) (Table 3).
Bivariate and Multivariate logistic regression analysis results on factors associated with overall household satisfaction level in Addis Ababa, 2021.
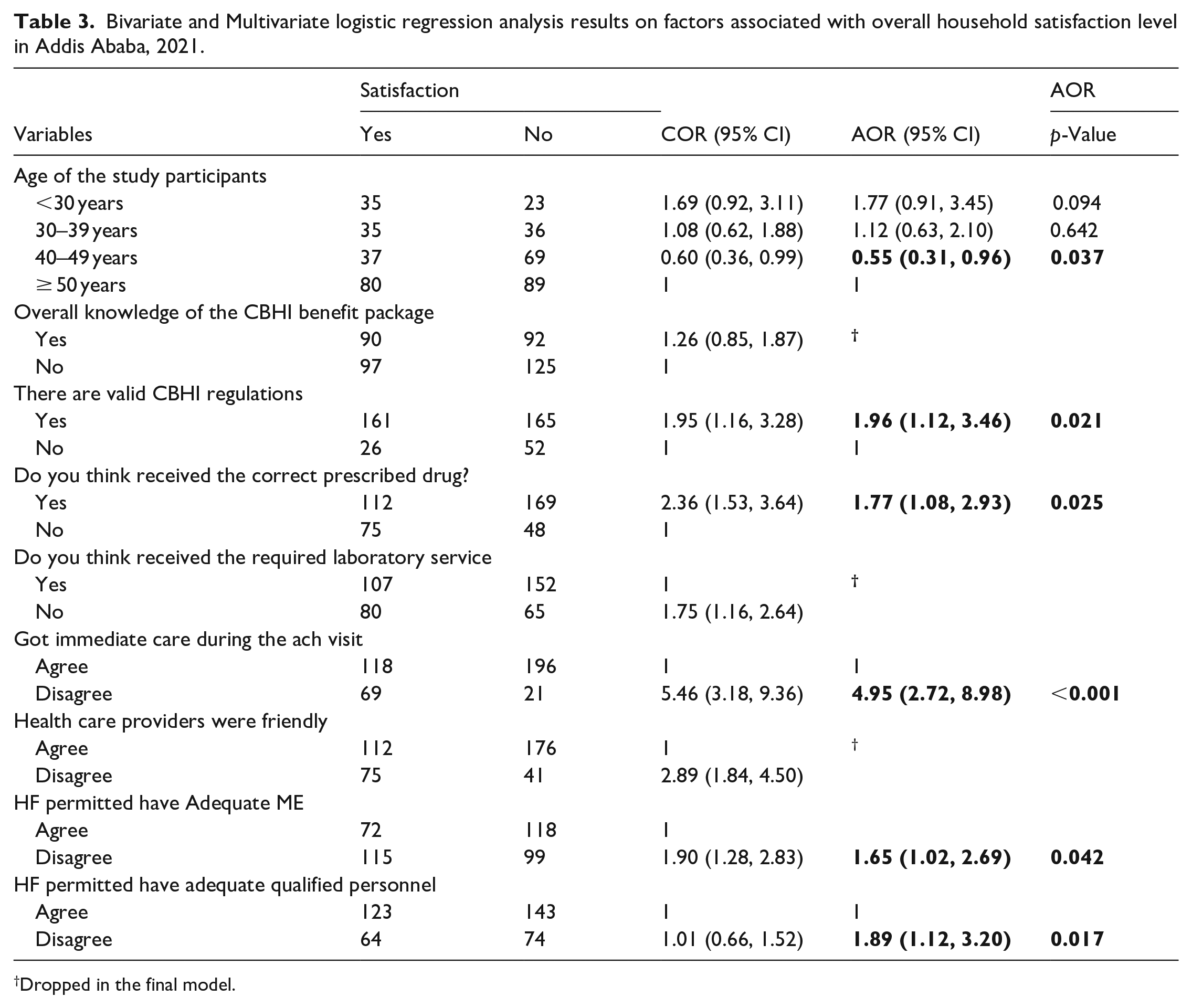
Dropped in the final model.
Perception of CBHI beneficiaries about challenges of the program
The qualitative results
The analysis of qualitative data revealed six major challenges of the CBHI program. The challenges were a shortage of drugs in the health institutions, nonappearance of kenema/public pharmacy in their nearby place of the beneficiary, disrespect and poor attitude of health professionals, lack of laboratory and other diagnostic services in the permitted public health facilities, health professionals lacked awareness about CBHI scheme and tight payment schedule.
Shortage of drugs in the permitted public health facilities (them 1)
Shortage of drugs in the permitted public health facilities is one the leading deliberated challenges by the majority of the FGD discussants. Although the CBHI benefit package is supposed to cover all outpatient costs of the beneficiary, a significant number of the FGD discussants were complaining about the unavailability of drugs in the permitted public health facilities
One of the FGD participants reflected that one of the most common challenges faced by the members of the CBHI scheme is the lack of drugs and laboratory services in the permitted public health facilities. This is mainly due to the lack of laboratory services and the absence of prescribed drugs in pharmacy rooms. Even though I get referred to hospitals to get better laboratory services and medications the reality is the opposite. I get referred to private institutions for both services which makes me unsatisfied with the service
Another FGD discussant also commented on the following: the problem with both hospitals and health centers is that the medications and laboratory services ordered are not available within the institutions. This is a big problem for us since we have to pay from our pocket to get these services in private clinics. In turn, we don’t even get our money back from CBHI. Because there is no system to get our money back after we paid from our pocket to private institutions it makes me so sad. So it would be very nice for us if this problem gets solved
Absence of kenema/Public pharmacy in their nearby place (theme 2)
The other challenge mentioned by the participants was the absence of a kenema pharmacy in their nearby place to get the prescribed drug easily. According to the FGD discussants traveling a long distance to get to kenema pharmacy and ordering drugs makes them very disappointed. In relation to this one of the FGD discussants explained that in addition to the challenges mentioned by the previous discussants, we don’t have kenema pharmacy in our woreda. We have to go far from here to find kenema pharmacy so it would be so nice if someone was built for us nearby. Because most of us are very old people and it is tiresome and inconvenient for us to travel a long distance to find drugs. Apart from this, the transport fee is also another cost for us. Moreover, occasionally the pharmacy professionals also send us back to the health center if there is a problem with the prescription. All these things are cumbersome for us
Disrespect and poor attitude of health professionals (theme 3)
Disrespect and poor attitude of health professionals were one of the boldly visible extracts from the FGD. The FGD participants said: the main problem of pharmacists working at kenema pharmacies is their wrong attitude towards CBHI members. They do not serve us as similarly as those who pay out of their pocket. I remember one time I was having a prescription paper and another patient who is not a member also got the same prescription paper. The pharmacist received the prescription paper and gave the medication to the one who pay out of pocket (not a member of CBHI) but he refused me and said it was not available. As a result, I went to buy from a private pharmacy it is really saddening or embarrassing anyways
Another FGD participant also pointed out that both CBHI members and others were not treated equally and explained the following “I get disappointed most of the time when I went to kenema pharmacy to get the service. The problem is that pharmacists who work there did not treat CBHI members and others who are not members equally. For example, during my previous health center visit, I got the service and the doctor gave me a prescription paper to get medication from the health center but the prescribed drug was not available in the health center. Then I went to kenema pharmacy to get the prescribed drug. When I told the pharmacist that I am a member of CBHI his facial expression was changed and not happy to serve me with respect. However, when another customer who paid for the medication comes he treated him happily with respect”
Lack of laboratory and other diagnostic services in the permitted public health facilities (theme 4)
The majority of the FGD discussants reported the lack of laboratory and other diagnostic services in the permitted public health facilities also another challenge, one of the FGD participants explained the following; “the problem in the health centers is that most of the laboratory services were not available even at the hospital level. I observed the same problem sometimes if the laboratory services were available the long cue makes it impossible to get the service on time. To get some diagnostic services like ECG we have to wait for a month or more. If you seek timely service, you are forced to get the service at private health centers and it’s really costly for us”
Health professionals lacked awareness about the CBHI scheme (theme 5)
Strikingly the discussants witnessed that health professionals lacked awareness about the CBHI scheme in accordance with this one of the FGD participants commented the following; “I don’t think even the pharmacists who are working in kenema pharmacies understood the costs incurred by CBHI members get reimbursed from CBHI scheme. The government should create an awareness creation session about the CBHI scheme for them as they are making us unsatisfied with the service we get from CBHI”. Similarly, another discussant also explained his experience as follows: when I went to hospitals I wait long hours in card rooms, and the attitude of health professionals towards CBHI members is not positive. I remembered this one time when I brought my child to the hospital and the card room lady and the health professional gave me different orders mainly because I am a CBHI member.
With regard to this one of the FGD participants forwarded the following recommendations: “in addition to what has been said the problem at kenema pharmacy should not be forgotten. I think the government should create awareness for them so that they understood the case and provide the service equally for CBHI members and others who are not members of CBHI. In addition, another participant also suggested that the government needs to work hard on the attitude of health professionals, particularly pharmacists working at kenema pharmacy.”
Tight payment schedule (theme 6)
The premium payment modality is also another challenge for the beneficiaries owing to the low economic status of the beneficiaries the payment schedule was not convenient as explained by the FGD participants in relation to this one of the FGD participants motioned the following: “I am not against the amount of the fee that I pay but the problem is the fixed time payment modality because it is hard to find and pay this amount of money at once. If the payment could be made on a two times basis it would help a lot to cover the premium fee without stress”
Discussion
This study aimed to assess the satisfaction of CBHI members and associated factors among households who are members of the CBHI scheme. In this study, the level of satisfaction with the CBHI scheme was found to be 46. 3%. The finding of this study was somehow similar to the previous studies conducted in Sheko 54.7% of the members of the CBHI scheme were satisfied with the scheme. 4 Another study conducted in the Anilemo district Hadiya zone in southern Ethiopia also reported that the magnitude of household satisfaction with the CBHI scheme was 54.1%. 29 However, another study done in the Damotwoyde district of the Wolyta zone in SNNP reported that the satisfaction of members toward the CBHI scheme was found to be 91.4%. 23 The possible reason for this discrepancy might be due to the difference in the socio-demographic characteristics of the respondents, the tools used to measure the satisfaction level of households, and the time difference of the study. For instant, our study used 17 standardized questions using a five-point Likert scale to assess the overall household satisfaction level. Whereas the study conducted in the Sheko and Damotwoyde districts of the Wolyta zone in SNNP used only six questions scale to assess the overall satisfaction level.4,23 This is one of the possible reasons for the discrepancy because asking more questions about satisfaction may probe more problems with CBHI enrollment.
In this study households whose age lies between 40 and 49 years were less likely to satisfy with the CBHI scheme compared to households aged greater than 50 years (AOR = 055, 95% CI; 0.31, 0.96). The finding of this study is in line with the previous studies conducted in northern Ethiopia, 10 Nigeria, 30 and Turkey. 31 This might be attributed to the difference in the expectation of the service and the frequency of getting the service, older people get more frequent illnesses compared to younger people. When the frequency of visiting the health facilities increased and getting the service without paying out of their pocket the likelihood of satisfying with the service also increased as illustrated in the previous study. 23
Households who think a presence of valid CBHI management regulations were two times more likely to satisfy with CBHI enrollment compared to their counterparts (AOR = 1.96, 95% CI: 1.12, 3.46). The result of this study was similar to the previous studies conducted in the Damotwoyde district of the Wolyta zone in SNNP. 23 The possible reason might be households who have a better understanding of the regulations of the CBHI scheme have a higher chance of satisfying with the service 23
In accordance with the previous studies,10,23 in this study households who agreed that sick family members received the correct prescribed drug during their recent visit were more likely to satisfy with the CBHI scheme compared to their counterparts (AOR = 1.77, 95% CI: 1.08, 2. 93). The possible reason as mentioned by Addise et al. 29 might be due to households who enrolled and did not get the right prescribed drugs in a public health facility were obliged to pay additional costs for private pharmacies which might be the causes of dissatisfaction with the CBHI scheme.
Study participants who got immediate care during their visit were five times more likely to satisfy with the CBHI scheme compared to their counterparts (AOR = 4.95, 95% CI: 2.72, 8.98). The finding of this study was in agreement with the previous studies conducted in Rwanda 32 households who received immediate and respectful care during the recent visit were more likely to satisfy with the CBHI scheme. It is known that participants who got immediate care during visiting health facilities will have a better level of satisfaction
Households who agreed that the permitted health facilities have adequate medical equipment were more likely to satisfy with the CBHI scheme compared to households who didn’t agree (AOR = 1.65, 95% CI:1.02, 2.69). The finding of this study is scientifically plausible because households who assumed to get proper treatment with adequate medical equipment have a better chance of satisfaction with the program compared to those who were not agreed with the adequacy of medical equipment.
Apart from these study participants who believed that the permitted health facilities have adequate qualified personnel was more likely to satisfy with the CBHI scheme compared to their counterparts (AOR = 1.89, 95% CI; 1. 12, 3.20). Study participants who believed in the qualification and competency of health professionals found in the permitted public health facilities were more likely to satisfy with the service they got from those health facilities.
Moreover, the qualitative part of this study pointed out the shortage of drugs in the permitted health facilities, the absence of kenema pharmacy in their nearby place, disrespect and poor attitude of health professionals, lack of laboratory and other diagnostic services in the permitted public health facilities, health professionals lacked awareness about CBHI scheme, and tight payment schedule are the major challenges of CBHI implementation.
This study was conducted in all sub-cities of Addis Ababa with a mixed study design hence this could be considered as a strength of the study. Concerning the limitations of the study, the quality of the data might be affected since data collection was done during the covid-19 pandemic, and self-reported data may attenuate the association observed between the factors and the outcome variable.
Conclusions and recommendations
Conclusions
Health service equity and quality are important indicators in achieving universal health coverage goals. To achieve these goals, establishing a sustainable community-based healthcare financing system is indispensable. Understanding the level of client satisfaction toward community-based health insurance was one of the major factors to ensure the sustainability of the CBHI program. This study revealed that less than half of the study participants were satisfied with the CBHI scheme in Addis Ababa. Study participants who agreed with the presence of valid CBHI regulations, households who think they got the right prescribed drug during the recent visit, CBHI members who agreed that the permitted public health facilities have adequate medical equipment, households who believe that the permitted public health facilities have adequate qualified health personnel, and study participants who got immediate care during health facility visits were more satisfied than their counterparts. Apart from these, the FGD discussants deliberated the challenges of the program implementation such as shortage of drugs, disrespect and poor attitude of health professionals, lack of laboratory service, the absence of kenema pharmacy in their nearby place, health professionals lacked awareness about the CBHI scheme and a tight payment schedule
Recommendations
The government of Ethiopia has implemented CBHI in order to insure universal health coverage. Hence, in order to improve service provision and the satisfaction level of CBHI members, the following measures need to be considered.
✔ Addis Ababa health bureau should work on availing medications, and medical equipment required both at health centers and at hospitals and consider building Kenema pharmacies in the nearby distances to CBHI members
✔ This study found that CBHI members who were well aware of the regulations were more satisfied. Therefore, the bureau together with sub-city and woreda should work to create awareness among members and to improve the way CBHI clients are treated both at hospitals and at health centers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.