
Abstract
Background:
In the United States, healthy behaviors, such as eating fruits/vegetables and exercise, are well below recommended levels, particularly for Hispanics. The COVID pandemic may have exacerbated existing health behavior disparities. The current study examines the impact of COVID social distancing measures on Hispanic parents’ eating and exercise behaviors, and how the impact may differ by socioeconomic status (SES) and distress levels.
Design and methods:
This cross-sectional logistic regression study utilized data from a sample of Hispanic parents in Texas (n = 237). COVID-related questions were collected in Summer 2020. Dependent variables included self-reported changes in exercise and eating behaviors due to the pandemic (i.e. got better or got worse). Primary independent variables included family-SES, neighborhood-SES, and distress due to COVID.
Results:
More than half (60%) of parents reported that their eating and exercise behaviors worsened. Results showed a significant relationship between distress due to COVID and both dependent variables; changes in eating (OR = 1.38, 95% CI [1.20, 1.58]) and changes in exercise (OR = 1.28, 95% CI [1.11, 1.48]). There were no observed differences by SES.
Conclusions:
Results suggest distress due to COVID was associated with worsening of eating and exercise behaviors, regardless of SES. The direction of the relationship between distress and healthy eating and exercise behaviors requires further attention.
Introduction
In March 2020, social distancing measures began in the United States (U.S.) due to the COVID-19 (COVID) pandemic. In the U.S., early-COVID social distancing measures included changes to remote employment with the exception of essential work, closure or virtual implementation of school, closures of public parks and recreation areas, closure of gyms, closure of most small businesses, and changes in capacity and hours of operations of grocery stores and supermarkets. Social distancing measures affected people’s lives across the globe in unforeseen ways, including in regard to exercise and healthy eating behaviors.1,2 Individuals in the U.S. engaged in health behaviors, such as eating recommended daily servings of fruits and vegetables and meeting weekly recommendations for exercise, at low levels prior to the pandemic, and these levels were notably lower among Hispanic individuals compared to their White and Asian counterparts. 3 In Summer 2020, Hispanics in the U.S. had the highest rate of COVID infection, 4 highlighting continued health inequities for Hispanics in the U.S. Although Hispanics are the second largest racial/ethnic group in the U.S., 5 few studies have examined the impact of COVID social distancing measures on eating and exercise with individuals in this demographic group. The current study adds to the COVID literature by examining this relationship among parents of young children, a population that has been uniquely impacted by the pandemic.
Socioeconomic status (SES) as a major contributing factor for racial/ethnic minority disparities in health behaviors (e.g. healthy eating and exercise) is well documented.6,7 The literature indicates that individuals from low-SES households and low-SES neighborhoods tend to show reduced levels of exercise and healthy eating.6,7 Further, racial/ethnic minorities tend to have a higher prevalence of living in neighborhoods which are often less resourced than those of their White counterparts 8 ; disparities may be exacerbated in such neighborhoods due to lack of access to healthy food and lack of safe, affordable options for exercise compared to more affluent households and neighborhoods.9,10 Recent studies found lower individual/family income was associated with worsening health behaviors during the early-COVID social distancing period11,12; however, no studies to date have examined this relationship with neighborhood SES. Examining neighborhood effects is important to continue to understand patterns of health across geographic areas, and to further acknowledge that individual health is influenced by not only individual behaviors, but also by contexts to which individuals belong.
In the U.S., results from various studies using non-nationally representative adult samples suggest decreases in healthy eating and exercise behaviors during the early-COVID social distancing period.13,14 For the purposes of this study, the early-COVID social distancing period is defined as March 2020–August 2020, which is in alignment with other studies described here.11 –18 For exercise, overall, adults showed increases in sedentary behavior and decreases in exercise during the early-COVID social distancing period, regardless of race/ethnicity.15,16 In regard to healthy eating, similar results showing negative impact were found. 17 Two studies found results relevant to parents/caregivers with families. Parekh et al. 18 found that food insecurity was more common among families with children; and Chenarides et al. 11 found that families with more people in the home and lower incomes were eating less fresh produce during this period. Research on the impact of the pandemic on healthy eating has seldom focused on the intersection of being a Hispanic parent of young children.
The direction of the relationship between exercise, healthy eating and distress was unclear prior to the pandemic, and the COVID literature continues to show this pattern. Prior to COVID, some studies found healthy behaviors to be protective against experiencing distress, while others found that health behaviors worsened when experiencing distress. 19 Focusing on COVID, one study found elevated distress to be associated with decreased engagement in healthy behaviors 20 ; while another found that engaging in healthy behaviors (e.g. exercise) was associated with better mental health. 21 For adults overall, Young et al.’s 22 study, of 20,000 adults in the U.S. during the early-COVID period, suggests that adults within the lowest physical activity group (no physical activity) of their sample had the highest depression and anxiety scores compared to all other groups. Evidence also indicates distress significantly increased for parents of young children in the early-COVID social distancing period.23,24 Increased distress was also associated with being a mother (compared to a father), being Hispanic/Latino, and having a lower income.20,23 One study suggested parents’ mental health was particularly affected by having to help their children with distance learning. 24 Alternatively, one study found that having young children in the home during this time was positively associated with mental well-being, compared with having older children. 25 A study from Uruguay found evidence of both situations in their sample, where some parents reporting difficulties managing their children’s behavior, and others reporting that they valued spending more time with their children. 26 As the relationship between exercise, healthy eating and distress is unclear, the current study partly focuses on understanding how distress due to the pandemic affected parent’s health behaviors (i.e. exercise and healthy eating).
The current study centers around two research questions: (1) are family SES and neighborhood SES associated with changes in eating and exercise behaviors during the early-COVID social distancing period within a sample of Hispanic parents of young children in the United States? and (2) how is self-reported distress related to the COVID-19 pandemic impact exercise and eating behaviors within a sample of Hispanic parents of young children in the United States? The current study will provide insights into how social distancing measures due to COVID affected the health behaviors of an understudies and vulnerable group in the United States.
Methods
Sample
The current observational study utilized demographic data collected from parents of pre-Kindergarten students in the fall of 2019 (i.e. baseline; N = 269), and follow-up data related to COVID-19 experiences collected between May-August 2020. To be eligible to participate, parents had to (a) have a child in pre-Kindergarten attending one of the participating schools, (b) be 18 years old or older, and (c) be able speak English or Spanish. The analytic sample included parents who identified as being non-white Hispanic (n = 237, 89% of the 269). The term “parents” in this sample includes anyone (biological-, adoptive-, step-parent, grandparent, aunt/uncle) who completed the survey as the student’s primary caregiver. The sample was 93% female, and the average age was 31 years. The sample consisted of a slightly larger proportion of parents who were married or living with a partner (58%) compared to parents who were unmarried or not living with a partner (42%). The average number of years of schooling completed by parents was 12 (SD = 2.52). The average family income-to-needs ratio was $6273 (SD = $6,510). For example, on average, a family of five people would have a yearly combined income of around $32,000. The average neighborhood poverty rate was 7.8% (SD = 1.78). The Institutional Review Board at The University of Texas at Austin approved study protocols and procedures.
Measures
The survey used in this study was a modified (i.e. shortened) version of a survey that has been used by a collaborating team for over a decade. 27 The original and shortened versions of the survey include well established measures; however, only the measures used in the study will be described below. The survey was only available in English and Spanish. Individual-level characteristics were assessed at baseline and were based on standard sociodemographic questions: gender, age, marital status, education level, and family SES. Family SES was expressed as income-to-needs ratio, which represents a yearly income dollar amount per person in the household.
COVID-19 Exposure and Family Impact Survey (CEFIS). The CEFIS was developed in a rapid iteration process at the onset of the pandemic and was released on April 16, 2020. 28 A native speaker on the development team translated the measure into Spanish. The translation was then back-translated into English by another native speaker on the development team. Only the English version has been validated, using data from 28 studies across the United States. The Impact subscale contains 10 items asking parents to respond to the impact of COVID-19 on different domains (e.g. physical wellbeing—eating, physical wellbeing—exercise) using a four-point Likert scale from 1 (made it a lot worse), 2 (made it a little worse), 3 (made it a little better), and 4 (made it a lot better), or parents could indicate Not Applicable. The subscale also includes two questions measuring distress due to COVID-19 for the participant and participant-reported family distress. The internal reliability of the subscale was found to be excellent (α = 0.92) in a large validation study. 28 In the current sample, internal reliability was demonstrated to be excellent and equal to that of the original study (α = 0.92 for English-language participants and α = 0.91 for Spanish-language participants).
Changes in Eating and Exercise During COVID-19. In the current study, parent responses to two questions of interest from the Impact subscale were used to measure how the COVID pandemic affected certain health behaviors: (a) “In general, how has the COVID-19 pandemic affected. . .” “your physical wellbeing—exercise?” and “your physical wellbeing—eating?” These responses were dichotomized to capture overall positive or negative impact. Responses 1–2 were recoded to 0 (made it better) and 3–4 to 1 (made it worse).
COVID-19 Related Distress. COVID-related distress was measured using the question that pertained only to the participant’s experience (not the family): “Overall, how much distress have you experienced related to COVID-19?” This question used a 10-point scale with 1 defined as no distress and 10 defined as extreme distress.
Census tracts were used as approximations of neighborhoods to cluster participants based on residential addresses provided at baseline, consistent with past studies. 29 Neighborhood SES was included as a cluster-level covariate. Neighborhood SES was based on the percentage of residents below 100% of the federal poverty line in the U.S. Census Bureau’s 2018 American Community Survey 5-Year Estimates. 30
Statistical analysis
First, we inspected variables for missing values and normality. We used multiple imputation (MI) to handle missing data. Before imputing, we grand-mean centered parent’s age, family SES, neighborhood SES, and education. Twenty imputations were conducted as this is common practice in the imputation literature. 31 The MI model included all the study variables and the following auxiliary variables: parent highest level of education operationalized as seven categories (less than high school to professional [JD, MD]) and household income expressed as a monthly income multiplied by 12 months.
After MI was conducted, we first examined the overall sample characteristics and compared the means to the raw data. Hierarchical linear models were used to test if multilevel models were appropriate. Null models were conducted to estimate intraclass correlation coefficients (ICCs) for both dependent variables. The null models indicated that there was insufficient proportion of variance related to neighborhoods to warrant the use of multilevel model building and it was determined that the more appropriate analysis was a single level logistic regression.
Logistic regression was performed to investigate associations of family and neighborhood SES variables with impact on a) healthy eating and b) exercise during early-COVID social distancing measures. First, unadjusted models were run for each variable. These models consisted of one independent variable and one dependent variable. This was done for both dependent variables. Then, all variables were entered together in a model that regressed impact on eating on all independent variables. This was also done with impact on exercise as the dependent variable. Using the SAS PROC MIANALYZE function after using the SAS PROC LOGISTIC function on the imputed dataset provided one set of fixed effects for all 20 imputations. To get the odds ratios (ORs) and accurate 95% confidence intervals (CIs), the beta estimates and the 95% CIs associated with those beta estimates were exponentiated. The analysis was generated using SAS software version 9.3.
Results
Table 1 presents means and SDs or frequencies and percentages for all individual- and neighborhood-level variables included in analyses. The majority of parents (60%) reported a negative impact of the pandemic on their physical wellbeing, such that it had worsened both their eating and exercise. The average distress due to COVID-19 score was 5.27 (SD = 2.67).
Descriptive characteristics of all study variables, n = 237.

M = mean. SD = standard deviation. Family SES: household income/number of people in the household. Family SES represents the dollar amount of yearly income per person; considering the average is $6430, a family of five people would have a yearly combined income of around $32,000.
As shown in Table 2 (Logistic Regression Models for COVID-19 Impact on Eating Behaviors) and Table 3 (Logistic Regression Models for COVID-19 Impact on Exercise Behaviors), the analysis showed a significant relationship between distress due to COVID-19 (OR = 1.38, 95% CI [1.20, 1.58]) and changes in eating, and a significant relationship between distress due to COVID-19 (OR = 1.28, 95% CI [1.11, 1.48]) and changes in exercise. In the current study, for changes in eating, a one-point increase in distress score was associated with a 38% increase in the odds of healthy eating behaviors worsening, holding all other variables constant. For changes in exercise, a one-point increase in distress score was associated with a 28% increase in the odds of exercise behaviors worsening holding all other variables constant. There were no other significant findings in the final models.
Logistic regression models for COVID-19 impact on eating behaviors.
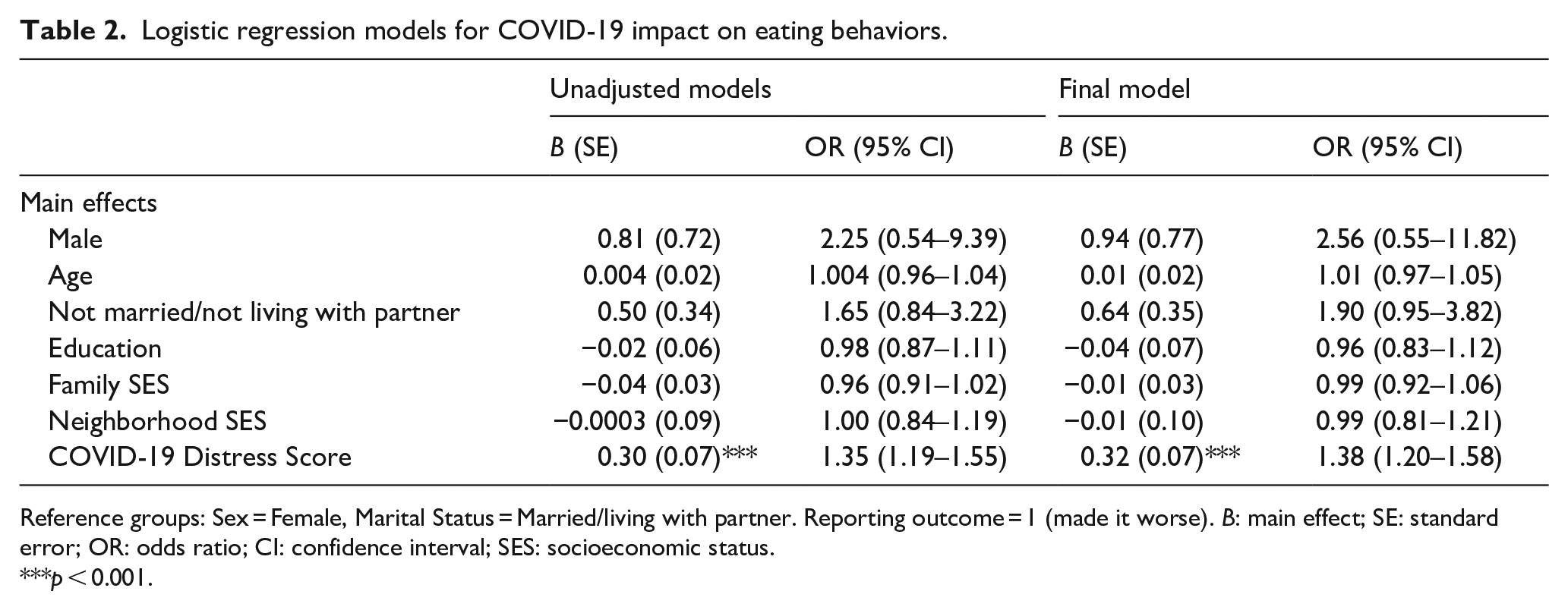
Reference groups: Sex = Female, Marital Status = Married/living with partner. Reporting outcome = 1 (made it worse). B: main effect; SE: standard error; OR: odds ratio; CI: confidence interval; SES: socioeconomic status.
***p < 0.001.
Logistic regression models for COVID-19 impact on exercise behaviors.
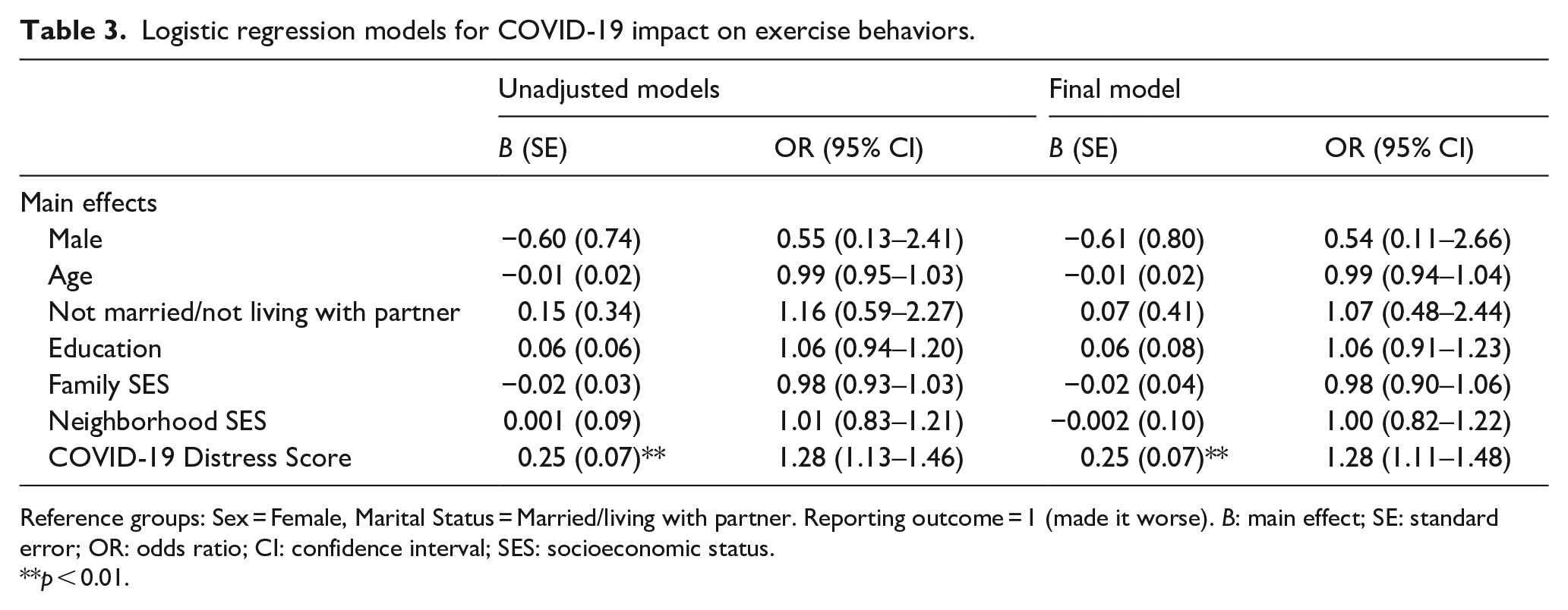
Reference groups: Sex = Female, Marital Status = Married/living with partner. Reporting outcome = 1 (made it worse). B: main effect; SE: standard error; OR: odds ratio; CI: confidence interval; SES: socioeconomic status.
**p < 0.01.
Discussion
The purpose of the study was twofold as it aimed to answer (a) if family SES and neighborhood SES were associated with changes in eating and exercise behaviors during the early-COVID social distancing period and (b) how self-reported distress related to the COVID-19 pandemic impacted exercise and eating behaviors, within a sample of Hispanic parents of young children in the United States. In the current study, more than half of the parents reported that their eating and exercise behaviors worsened during the COVID-19 pandemic. The study did not find family SES or neighborhood SES to be significantly associated with changes in eating and exercise behaviors during the early-COVID social distancing period. However, strong associations were found between self-reported distress related to the COVID-19 pandemic and exercise and eating behaviors.
These negative impacts on healthy eating and exercise are consistent with existing literature.1,2,32 As previously noted, COVID-19 social distancing measures relevant to this study included working from home (unless you were considered an essential worker), closure of schools, closure of public parks and recreation areas, closure of gyms, closure of most small businesses, and changes in capacity and hours of operations of grocery stores and supermarkets. During the summer of 2020 in Texas, most daycare and camp-related businesses were either closed or operating at limited capacity. 33 Additionally, families may have been hesitant to have their children return to in-person activities outside the home. Increased childcare demands meant that parents potentially had less time to engage in healthy behaviors, such as exercise. Greaney et al.’s 16 study on informal caregivers suggested that caregivers living in the same house as the person they provided care for were more likely to report decreased exercise during this period. Prior to the pandemic, Hamilton and White 34 found that many parents described the difficulties of being active with their children and that parents did not prefer to be active with children. They also found that parents reported a decline in exercise after initially having children, 34 and the early-COVID-19 period may have resembled the initial period after having a child due to the increased childcare demands in the home. While Hamilton and White 34 also found that partner roles (i.e. mother or father) were considered most influential on exercise behaviors, there were no significant findings for gender associations in the current study. Overall, not having the time or a place to go may have negatively impacted parents’ exercise behaviors. Given the evidence from the pre-COVID literature, future studies should continue to examine gender differences. It is likely that there was not enough power due to small group samples to detect gender difference.
There are also various potential reasons for the reported negative impact on healthy eating. In families where parents were not considered essential workers, they may have experienced loss of employment. With the large number of unemployment benefit requests, it took individuals longer than usual to receive benefits 35 ; thus, families in the United States could have experienced food insecurity early in the pandemic. The literature provides evidence that food insecurity was more common among families with children 18 and that families with lower incomes were eating less fresh produce during this period. 11 Another possible factor for the reported negative impact on healthy eating is the restricted availability and access to food while social distancing measures were in place due to limited hours of grocery stores, fear of going to the grocery store, and bulk buying from uncertainty of future access. 36 The COVID literature suggests that families’ healthy eating may have been impacted by several factors, that were not captured in the current study, such as food insecurity and decrease in consumption of fresh food.11,18 The literature also suggests that food insecurity is indirectly associated with poor nutrition through poor mental health, 18 which aligns with the current study’s finding that high levels of distress were associated with negative changes in healthy eating.
The relationship between family SES, neighborhood SES and changes in healthy behaviors was not significant in the current study. This is unexpected as the literature suggests that individuals with higher family and neighborhood SES engaged in healthier behaviors during social distancing.11,12 Some of the benefits that higher SES may offer, such as increased access to healthy food and more opportunities for exercise (e.g. access to a gym or personal trainer), compared to less affluent households and neighborhoods,9,10 may not have been as protective during the early social distancing period as it may be during non-restrictive normal periods. It may also be the case that distress due to the pandemic attenuated these relationships because it was an unprecedented time for everyone, regardless of SES. Neighborhood SES and health behavior changes due to the pandemic have not received much attention to date. Future studies with samples that cover wider SES disparities may be able to detect SES effects.
The current study found that greater COVID-19 related distress was associated with worsening healthy behaviors, although as mentioned in the introduction, the direction of this relationship is unclear. Schultchen et al. 19 suggest the relationship may be reciprocal. Some studies reported that exercise helped lower stress from the pandemic, while others reported that individuals who were more stressed engaged in less physical activity during this period.2,37 Most evidence points to the importance of exercise to cope with distress; though, the literature and the current study also suggest that distress may be preventing one from exercising in the first place.2,21 As it relates to eating, some studies suggest increases in distress during the pandemic were associated with a greater desire to consume comfort foods. 38 Distress during the pandemic was also linked to increased alcohol consumption paired with decreased healthy eating. 39 It is important to put the sample into context as well. Evidence exists to suggest that distress significantly increased for parents of young children and Hispanics/Latinos in the early-COVID social distancing period.20,23,24 For Hispanic parents of young children, increased COVID rates in Hispanic communities, paired with increased childcare demands due to business closures and restrictions may have left them feeling particularly distressed.4,23,24 Overall, this period of considerable barriers and stress may have been exacerbated for parents of young children who may have limited “child-free” time and sleep, as well as difficulties in managing work-life balance, which all could have affected health behaviors. 40 Though the direction between distress and health behaviors, in general, is not clear, findings from this study offer insights when put into context of the literature, which indicate that improving one outcome may improve the other. Distress due to an unprecedented event such as the pandemic may be difficult to prevent; thus, future research should examine how public health efforts can increase positive health behaviors to stop the cycle between poor mental and poor health behaviors.
Strengths and limitations
There were several strengths as well as limitations with the current study. The findings represent mostly Hispanic mothers of young children. This was a small, non-nationally representative sample and Hispanic mothers/caregivers of young children may have faced challenges related to having young children in the home that other adult groups may not have faced during this time (e.g. no children in the home). There was little variability in neighborhood poverty and family income, which could have attenuated SES effects. Family SES variables were only collected at baseline and information regarding changes in SES during the pandemic could allow for further comparisons. We relied on participant retrospective report of changes in behaviors. There was missing data for income and the dependent variable; however, a rigorous imputation method was conducted. Additionally, we conducted an examination of variance across multiple levels of data. Future studies should examine the resiliency of Hispanic adults who did not report worsening behaviors and factors associated with positive or no change in behaviors.
Conclusions
Parents should continue to be encouraged to increase physical activity in order to reduce stress, which may also help reduce poor eating behaviors. However, health professionals who may be providing this advice (e.g. social workers, primary care physicians) must also acknowledge that the COVID-19 pandemic is a challenging time for everyone, especially parents. Individuals may be stuck in a cycle of not exercising and eating poorly because of stress from any number of issues related to the pandemic (e.g. contracting the virus, family members dying, loss of job, managing work and kids at home, etc.). Outlets promoting simple ways to exercise at home, such as exercise videos, meditation, and yoga, often do not consider the realities of home life with working from home, distance-learning, and keeping up with everyday household responsibilities and activities. Providing families with safe and culturally appropriate avenues for being physically active and promoting healthy eating is necessary for helping parents recover from the setbacks they may be facing with their health. Targeting mental health practices to support parents to overcome pandemic-related distress may additionally lead to improved physical health behaviors.
Footnotes
Acknowledgements
We are grateful to the families who participated in this research, and to our colleagues at CCISD and NYU for their partnership. We also thank Dr. Nate Marti for consulting on the statistical approach.
Author contributions
Conceptualization, C.E.V., E.J.C., and C.C.; methodology, C.E.V. and C.C..; software, C.C.; validation, C.E.V. and K.E.H.; formal analysis, C.E.V.; investigation, C.E.V.; resources, E.J.C. and S.K.B.; data curation, C.E.V, K.E.H., and M.J.M.; writing—original draft preparation, C.E.V.; writing—review and editing, K.E.H., M.J.M, C.C., E.J.C, and S.K.B.; super-vision, C.C., E.J.C., and S.K.B; project administration, E.J.C and S.K.B.; funding acquisition, E.J.C. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Morris L. Lichtenstein Jr. Foundation. The funder had no influence on the design of the study, data collection, analysis, and interpretation of data in writing the manuscript.
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of [masked for review]. Informed consent was obtained from all participants involved in the study.
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Significance for public health
COVID-related research is abundant; however, fewer studies have examined the intersection of COVID social distancing measure, social determinants of health, and racial/ethnic inequities. This study examines this intersection by reporting on how eating and exercise behaviors of Hispanic parents of young children were impacted by early-COVID social distancing measures. This study further examined how the impact may have differed for parents with different family and neighborhood socioeconomic status (SES) and by self-reported distress due to the pandemic. The results suggest distress due to COVID was associated with worsening of eating and exercise behaviors, regardless of SES. The significance for public health is two-fold: (1) this is an understudied population in public health research and (2) this contributes to the literature that indicates parents struggled with their physical and mental health during the COVID and those struggles may have long-lasting effects that are pertinent for public health efforts to target.
Availability of data and materials
The datasets used and/or analyzed during the current study will be available from the corresponding author on reasonable request at the termination of the study.