
Abstract
The COVID-19 epidemic affected both acute hospitals and post-acute care, which experienced various degrees of overcrowding. We evaluated all the patients admitted to a post-acute care facility during the second wave of the epidemic to detect features possibly associated with social frailty. We analyzed the socio-demographic characteristics and comorbidities of the patients and the pattern of their previous hospitalization as available in their discharge letter. In addition, we evaluated their clinical features and tests on admission to post-acute care. We found that COVID-19 patients without social problems had distinctive features. Those with a higher need for specific pharmacological treatments during their stay in an acute hospital were less likely to be admitted to post-acute care for concomitant social problems (p < 0.05 for all types of medication). They were also more likely to be native (p = 0.02), obese (p = 0.009), and with hypertension (p = 0.03). Patients with social problems usually stayed longer and were less frequently discharged home with a negative swab (p = 0.0009). In COVID-19 patients, recognition of distinctive features predicting that their need for a longer hospital stay is due to social problems can lead to more appropriate discharge and to more appropriate use of post-acute care.
Introduction
Post-acute care has been implemented in many countries to reduce the length of stay in acute hospitals, while continuing to deliver patients the assistance they need. It is known to reduce hospital readmissions, 1 to improve the performance status of elderly patients 2 and to be a primary area to attempt cost containment. 3
The duration of hospital stay is dependent not only from the comorbidity of patients, but also from social determinants. These are known to have considerable weight, to be a contributing cause of comorbidities, and to require specific interventions.4,5
Post-acute care includes different settings of care: skilled nursing facilities, rehabilitation, low-intensity wards, and at home patient care. In Lombardy, low intensity wards for patients discharged from acute hospitals are called sub-acute care units.
The present COVID-19 pandemic has had a profound impact on the Health Systems all over the world. Hospitals have been confronted with a dramatic increase in the need of beds, initially in the acute and intensive care area. Concomitantly almost all the wards have been involved, also for the need to discharge stabilized patients from the intensive units making beds readily available.
Post-acute care providers have been no exception. Moreover, it has been proposed a role for them in preventing avoidable hospital admissions and in operating as post-acute COVID units. 6 Another important issue with potential bearing on post-acute care, long-term care, and rehabilitation care is the fact that COVID-19 patients discharged from acute hospitals can continue to have clinical problems more than 28 days after the onset of infection and up to many months later, as demonstrated by various studies.7,8
This is what happened also in Lombardy.
In this scenario, factors at play in the delicate phase of discharging patients from acute hospitals to post-acute care can be crucial. On one hand, social factors affecting admission, length of stay, and discharge could be partially different from those we usually take into consideration. 4 On the other, not many studies are available on this subject, in spite of its relevance.
On this basis we investigated the potential relevance of three social determinants for patients discharged to a subacute care unit and we evaluated if they are associated with specific socio-demographic factors or with peculiar clinical features during their preceding hospital stay.
Design and methods
Patients and statistical analysis
We studied all the 114 patients admitted to a 16-bed post-acute care ward in Monza, Italy, from October 26th to December 16th, that is, during the second wave of COVID-19. We collected administrative, demographic, clinical and social data, and data of the preceding period in an acute ward, including pharmacological treatments, which are essential to avoid missing an important part of the patient’s real conditions. 9 More in detail, for each patient we collected all information from the available data source, which was represented by the discharge letter and, for some, by previous personal clinical documentation. Information on age, gender, nationality, marital status, and co-pathologies was recorded. Clinical data relating to the period in the acute hospital included length of stay and the need for these treatments: dexamethasone, remdesivir, antibiotics, oxygen, and mechanical ventilation. All the patients were on anticoagulation with low molecular weight heparin, except two, who already were on direct oral anticoagulants for other medical conditions before becoming infected. On admission to post-acute care, we also analyzed and recorded the signs and symptoms of patients, their need and type of administration of oxygen therapy, and the results of chest x-ray and of a panel of blood tests.
The length of stay in the post-acute ward and the outcome at discharge was also evaluated.
We considered an admission as motivated by social aspects in the presence of one of the following:
Isolation impossible at home
Hospital acquired asymptomatic COVID-19
Absence of the usual caregiver (either because infected or for fear to become infected)
If one of these took place during the period spent by a patient in sub-acute care (typically, discharge made impossible by the sudden unavailability of the caregiver) the period was split into days with clinical motivation and days with social motivation.
Categorical variables were summarized as absolute and percent frequencies, and compared between groups through the Chi-square test or the Fisher exact test, were appropriate. Continuous variables were reported as mean and standard deviation, or median and interquartile range, and compared between groups through the T-test or the Wilcoxon rank sum test, where appropriate. All analyses where conducted using the version 9.4 of the SAS package (SAS Institute. Inc. Cary, NC, US).
Results
Table 1 shows the data of the two groups of patients before their admission to the sub-acute care ward. As can be seen, the only relevant demographic feature to predict social problems was nationality, with immigrants being at higher risk.
Characteristics of 114 patients admitted to post-acute care after a COVID-19 hospitalization.
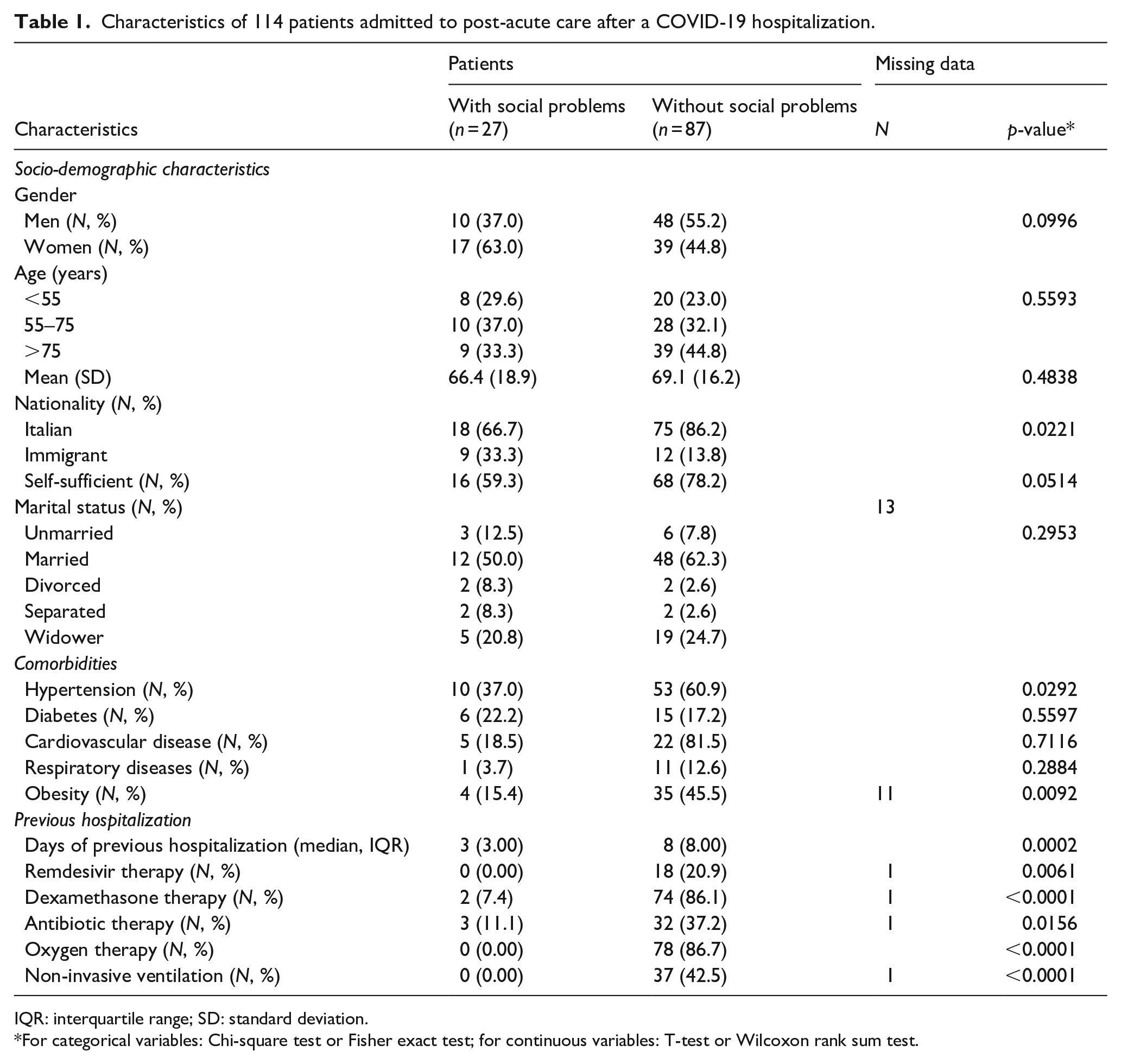
IQR: interquartile range; SD: standard deviation.
For categorical variables: Chi-square test or Fisher exact test; for continuous variables: T-test or Wilcoxon rank sum test.
Comorbidities were equally distributed in the two groups, with the exception of obesity (comprising all patients with Body Mass Index > 25) and hypertension.
Data of the previous stay in an acute care setting were more interesting: the length of stay had been shorter for patients with potential social problems while all pharmacological treatments had been more frequent in the other group.
Table 2 shows the main features of patients on admission to the sub-acute care ward. No differences were seen for symptoms, while patients unlike to be burdened by a social component had more frequently a pathologic chest x-ray and needed oxygen therapy, more frequently with a Venturi mask. Their blood tests showed some differences as well, with white blood cell count, alanine aminotransferase (ALT), and cholesterol being significantly higher.
Clinical and laboratory features of 114 patients admitted to post-acute care after a COVID-19 hospitalization.
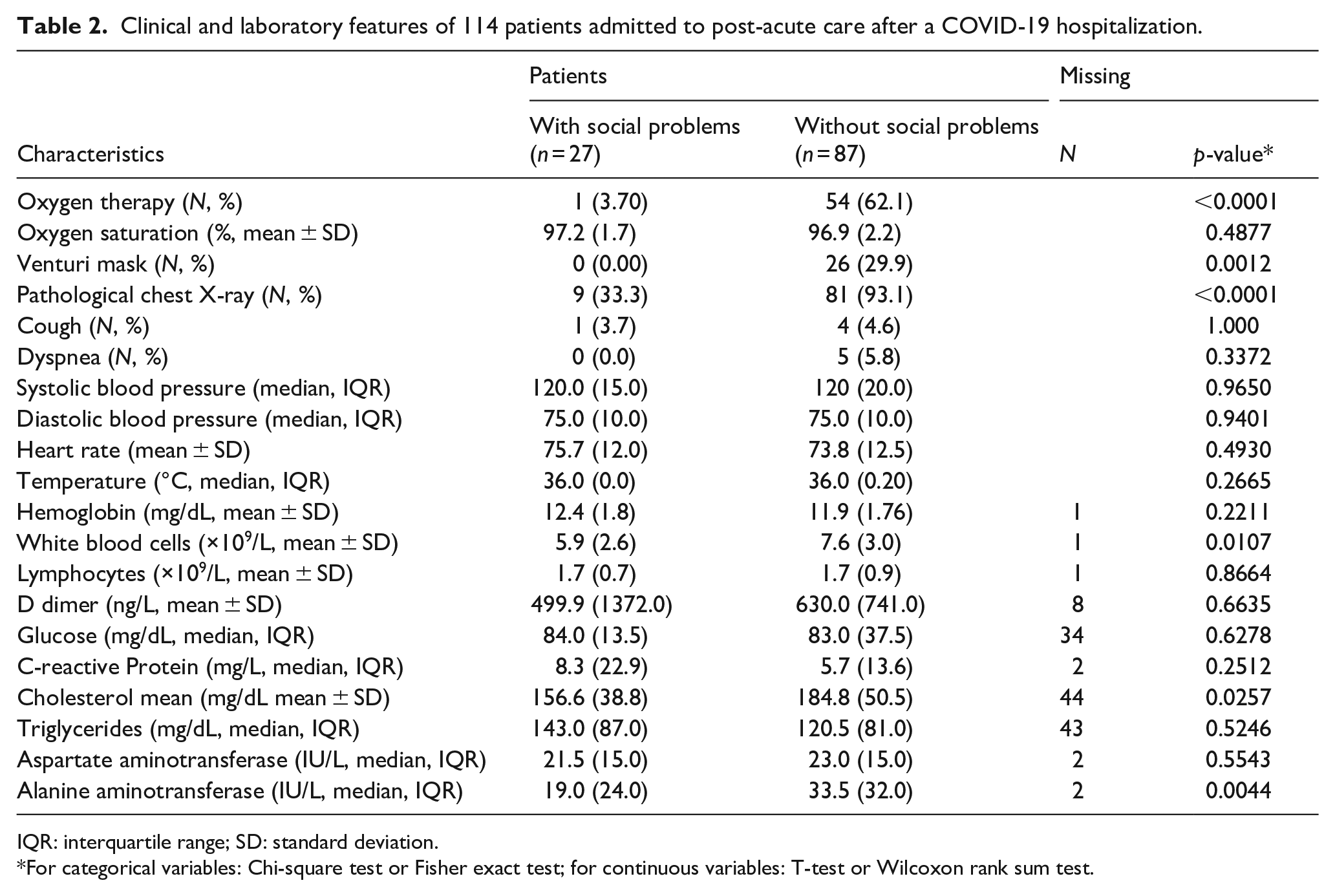
IQR: interquartile range; SD: standard deviation.
For categorical variables: Chi-square test or Fisher exact test; for continuous variables: T-test or Wilcoxon rank sum test.
Finally, we noticed that patients whose admission was partially determined by social aspects, stayed longer (median 17 days, IQR 16 vs 11, 9; p = 0.007). Their stay accounted for 784 of the cumulative 1760 days spent by all COVID-19 patients in the post-acute ward in that period.
Since the cost of a subacute care bed is 190 €/day this meant an expense of 148,960 € for patients with social problems.
Finally we observed that while the rate of discharge home of patients with a positive swab was comparable in the two groups, that of patients with a negative swab was significantly lower for patients with social problems (26/67 vs 5/47; p = 0.0009).
Discussion
The aim of this study was to identify distinctive features possibly predicting social problems in some COVID-19 patients discharged from acute hospitals to post-acute care. We found that patients who had had a more severe disease were less frequently burdened by social problems. This was confirmed also by the evaluation on admission to post-acute care, as demonstrated, for example, by a worse chest x-ray and a more frequent need for oxygen therapy in patients whose transfer was not conditioned by social determinants.
We are aware that our study has some limitations, the major being the relatively small number of patients; this is due to the fact that though we enrolled all the patients admitted during the second wave, the ward had only 16 beds.
Therefore, we think that our findings should be considered only as preliminary indications, in the case a comparable event takes place again, though our study is the first to evaluate social problems in COVID-19 patients discharged to post-acute care.
Among pre-existing factors, a significant difference was noted only for nationality and two comorbidities (hypertension and obesity) which are known to be associated with a more severe course of the disease. 10
Obesity seems to be especially important since it is associated with an increased risk of exacerbations also from other viral infections of the respiratory tract. 11 Hypertension, as other comorbidities, could be associated with more severe COVID-19. 12
In a general context, the incidence and prevalence of multimorbidity is higher in socially disadvantaged individuals. 13 This was not true for our COVID-19 patients.
Not being an Italian native can be relevant because it might imply lower socio-economic status and problems in respecting adequate isolation in overcrowded households.
The main significant difference between patients with and without social problems was the need for COVID-19 medications during the preceding hospital stay. This was true for all treatments, including oxygen and non-invasive ventilation. It appears that preceding vigorous treatment is typical of those patients in whose discharge to sub-acute care social factors have no relevance.
It is interesting to note that also in this setting the analysis of pharmacological treatments is very useful to obtain a complete description of the real conditions of patients, as we have demonstrated for other situations.9,14
Analyzing data available on admission to the post-acute unit, we found that the need for oxygen, the presence of a Venturi mask, and a pathologic chest X-ray were more frequent in patients with no social problems. This was not unexpected.
Symptoms and vital signs were comparable in the two groups.
Laboratory tests showed some differences. Total white blood cell count was higher in patients without social problems but the absolute lymphocyte count was identical. These patients also had higher ALT and cholesterol. The first finding could imply a more severe form of COVID-19 with liver involvement, or pre-existing liver disease, 15 or be a consequence of anti-viral medications. The role of cholesterol in COVID-19 is still debated. 12
Taken together, our findings seem to indicate that patients with a more severe disease have a lower risk of concomitant social problems when discharged to post-acute care. On the contrary, being non-native, a lower burden of comorbidities, and especially a smoother course of the disease requiring less medications, seem to be predictive of a social component that has a role in the admission to post-acute care.
During this pandemic, hospitals had to face an enormous strain. Emergency departments were rapidly crowded by patients with COVID-19 requiring admission 16 and the need rose to make many more beds quickly available. 17 This also entailed a reduction in admissions of non COVID-19 patients, especially for elective procedures. 18 Even in Countries that did not suffer bed shortage in absolute terms, some hospitals experienced a certain degree of overcrowding due to uneven distribution of bed utilization. 19 In some areas, a confluence of COVID-19 epidemic and pre-existing comorbidities in the context of social disadvantage has made the situation even worse. 20
Moreover, this pandemic has prompted a revision of the criteria used to discharge patients to sub-acute care and has strengthened the cooperation between acute and post-acute settings of care.6,21 New criteria are now being proposed to make this collaboration more straightforward. These underline the fact that collaboration of different sectors of healthcare must become the norm and that the same solution does not fit all situations. 22 It is therefore evident that more studies covering different aspects of this area of collaboration are urgently needed.
In this context, early recognition of patients with more social than clinical problems could allow more appropriate and possibly less expensive solutions and save acute and post-acute beds for both COVID and also non-COVID patients. Indeed, the latter exist also during pandemics and, for post-acute wards a special problem is represented by “high-cost” patients needing an enhanced and more resource consuming level of post-acute care. 23 This need could hardly be met if a part of the beds is dedicated to patients with predominant social conditions.
In this context, our study could be a contribution of some help in the field of collaboration across healthcare sectors.
Footnotes
Authors’ contributions
GF and SGC designed the study and wrote the manuscript; GP and MF performed the statistical analysis; CP collected the data; GC and AER contributed to the interpretation of the results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Italian Ministry of Education, University and Research (“PRIN” 2017, project 2017728JPK).
Ethical approval
Since the study is retrospective, an authorization protocol number by the local ethics committee was not required. All data were completely and permanently anonymized. All procedures were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Significance for public health
COVID-19 patients discharged from acute hospitals can continue to have clinical problems usually referred to as “long covid,” but they can also have a significant burden of new or pre-existing social problems.
Our study demonstrates that these social problems were frequent in patients discharged to post-acute care. These patients had some distinctive features, one of them being a lower need for pharmacological treatments during their stay in acute wards.
A method to identify these patients, as that described in our study, can lead in the future to more appropriate discharge, increased availability of beds, and less expensive solutions. This appears to be extremely important in periods as the COVID-19 pandemic, when a dramatic shortage of hospital beds is experienced by many countries.
Availability of data and materials
The data used to support the findings of this study are available from the corresponding author on reasonable request.