
Abstract
Background:
The COVID-19 pandemic changed care delivery. But the mechanisms of changes were less understood.
Objectives:
Examine the extent to which the volume and pattern of hospital discharge and patient composition contributed to the changes in post-acute care (PAC) utilization and outcomes during the pandemic.
Research design:
Retrospective cohort study. Medicare claims data on hospital discharges in a large healthcare system from March 2018 to December 2020.
Subjects:
Medicare fee-for-service beneficiaries, 65 years or older, hospitalized for non-COVID diagnoses.
Measures:
Hospital discharges to Home Health Agencies (HHA), Skilled Nursing Facilities (SNF), and Inpatient Rehabilitation Facilities (IRF) versus home. Thirty- and ninety-day mortality and readmission rates. Outcomes were compared before and during the pandemic with and without adjustment for patient characteristics and/or interactions with the pandemic onset.
Results:
During the pandemic, hospital discharges declined by 27%. Patients were more likely to be discharged to HHA (+4.6%, 95% CI [3.2%, 6.0%]) and less likely to be discharged to either SNF (−3.9%, CI [−5.2%, −2.7%]) or to home (−2.8% CI [−4.4%, −1.3%]). Thirty- and ninety-day mortality rates were significantly higher by 2% to 3% points post-pandemic. Readmission were not significantly different. Up to 15% of the changes in discharge patterns and 5% in mortality rates were attributable to patient characteristics.
Conclusions:
Shift in discharge locations were the main driver of changes in PAC utilization during the pandemic. Changes in patient characteristics explained only a small portion of changes in discharge patterns and were mainly channeled through general impacts rather than differentiated responses to the pandemic.
Keywords
Introduction
The COVID-19 pandemic dramatically changed the landscape of care systems and service delivery.1-5 Due to rapid responses to the pandemic such as allocating labor and physical resources to treat COVID cases as well as health concerns about patient safety and risk of infection, the non-COVID care utilization declined across all service categories, for example, emergency department (ED) visits, 6 hospitalizations,7,8 outpatient care,9-11 preventive, and wellness visits.3,4 Further, studies showed disproportionate changes by service area, diagnosis, elective status, or care categories, for example, higher reduction in elective care (than non-elective care), surgically complicated cases (than uncomplicated), and preventive or maintenance care (than other care concerns).1,2,7,8
Less attention has been given to post-acute care (PAC) so far.11-13 Post-acute care provides patients with continuous recovery after hospital discharge. Though considered more discretionary than hospital care, PAC is critically important to prevent cognitive and functional deterioration, especially among the aging population. It is estimated that 41.7% of Medicare patients used PAC after being discharged from hospital.12,14 Cost-wise, PAC accounts for more than $60 billion in annual care costs among the Medicare fee-for-service beneficiaries and represents the highest cost growth category.14-16 Among the very few studies on PAC utilization during the COVID-19, findings suggested as high as a 51% decline in PAC admission volume among the general population, compared to a 46.5% decline in hospitalization.5,12 The monthly spending on PAC declined by 55% in skilled nursing facilities (SNF), 41% in home health agencies (HHA) and 32% in inpatient rehabilitation facilities (IRF).12,17-19
Various factors jointly contributed to changes in PAC utilization during the pandemic. These factors include the volume of non-COVID hospital admissions/discharges, hospital discharge patterns (to home and across all PAC facilities), and the composition of patients. It is unclear how these factors explained the changes in PAC and the related care outcomes.
First, while it is known that the non-COVID hospital admission declined and the hospital discharge patterns changed during the pandemic, 14 we do not know to what extent each of these factors contributed to the overall PAC utilization (ie, admission volume) changes. For one thing, as most PAC utilization was initiated from hospital care, a large portion of volume decline in PAC resulted from decreased inpatient admissions for non-COVID cases.7,8 Further, any additional changes in PAC admissions beyond the rates of inpatient admission changes depended on a combination of factors and hence could be ambiguous. For example, hospitals may shorten the length of stay for non-COVID and/or less complicated cases and move care toward PAC to reduce the burden and free up care capacity for COVID cases.15,18 But due to health concerns and risk of infection,13,20 patients may choose to use less PAC overall or choose to use more or less of certain types of PAC facilities (eg, home health or skilled nursing facilities).12,17,18
Second, changes in patient composition also resulted in changes in PAC utilization (ie, admissions across PAC facility types), especially via hospital discharge patterns (ie, to home vs various types of PAC facilities). The changes in hospital discharge patterns and the overall PAC utilization during the pandemic could come from at least 3 sources: (1) changes that can be explained by the patient demographics and clinical characteristics in general (eg, sicker patients need more intensive treatment)6–8; (2) changes that can be explained by the differential effects of patient-level characteristics during the pandemic relative to the previous period (eg, patients living alone were even more likely to use PACthan those who were living with others during the pandemic than before)21–25; (3) changes during the pandemic that are independent of patient characteristics (eg, changes in care delivery and practice).15,18 These sources of variation and the relative contribution to the overall PAC utilization changes are not well understood.
Third, we expect that changes in PAC utilization will result in changes in patient health outcomes and future healthcare costs both short- and long-term.5,21,22 Yet, there has been very limited research on this relationship thus far. Short-term responses in health outcomes may include changes in mortality and hospital readmissions.7,21,26 Long-term health outcomes could include physical and cognitive functional deterioration in the remainder of the life span due to missed or delayed detection or treatment in the corresponding post-acute care settings.27–29 These short- and long-term health outcomes will further lead to the projected changes in care costs, with significant social and economic implications for the patients, families, caregivers, 30 and the whole care sector and subsectors.17,18,27,29
The objective of this study is to assess the contributing factors such as the volume of non-COVID hospital admissions/discharges, the discharge patterns, and the patient composition to the changes in post-acute care utilization among the 3 common PAC types: home health agencies (HHA), skilled nursing facilities (SNF) and inpatient rehabilitation facilities (IRF) within the aging population during the COVID-19 pandemic. The study also aims to investigate the changes in clinical outcomes, for example, 30- and 90-day mortality and readmission rates while considering the changes in both volume and patterns of hospital discharge as well as the patient composition. Results from the study will provide patients, providers, and care systems with valuable insights on the magnitude and sources of changes in PAC utilization and care outcomes for non-COVID cases during the pandemic, which are important evidence to help mitigate the pandemic impacts and improve care delivery in the post-pandemic era.
Methods
Data source
This study used Electronic Health Records (EHR) and Medicare claims data to identify all non-COVID hospital discharges for patients 65 years or older who were assigned to an upper Midwestern care system in the US, an Accountable Care Organization (ACO) participating in the CMS Medicare Shared Savings Program during the study period from March 2018 to December 2020. The pre-pandemic period was defined as March 2018 to February 2020. The pandemic period was defined as March 2020 to December 2020. The care system (the ACO) included 7 hospitals and 146 outpatient clinics. On average, the ACO served about 21 000 to 22 000 Medicare fee-for-service beneficiaries each year, among whom 90.3% were 65 years or older.10,31
Study sample
The study sample included all index hospitalizations with non-COVID diagnoses in the care system (the ACO) during the study period for beneficiaries who were 65 years or older and alive at the time of discharge. We focused on individuals who were enrolled in Medicare fee-for-service program during the index hospitalization, and continuously enrolled in at least 30 days of primary medical coverage after discharge. The unit of observation was an index hospitalization. An individual patient may have more than 1 index hospitalizations, each of which had a different primary diagnosis code from the others. Readmissions (ie, hospitalizations with the same primary diagnosis codes as a previous index hospitalization), if existed, were not counted as additional index hospitalizations in the study sample. This study was approved by Institutional Review Board in the University of Wisconsin—Madison.
Key variables
The primary outcome variables included hospital discharge locations, 30-/90-day readmission and all-cause mortality. Discharge locations included the 3 common post-acute care types (ie, home health agencies (HHA), skilled nursing facilities (SNF) and inpatient rehabilitation facilities (IRF)), home, hospice, and others (eg, critical access/acute care hospitals, psychiatric and long-term care hospitals), which were jointly obtained from the discharge destination codes in Medicare Provider Analysis and Review (MedPAR) data file, EHR, and the subsequent claims. For readmission, we used the 30- and 90-day hospital readmission measure developed for CMS by the Yale School of Medicine Center for Outcomes Research & Evaluation.32-34 All-cause mortality also followed the 30- and 90-day frames for comparison purposes. We also reported other time frames to help compare the overall trends and the dynamics of changes over time. These time frames included 31 to 90, 91 to 180, 181 to 270 days mortality and 31 to 60, 61 to 90 days readmission.
The primary independent variable was an indicator of whether the index hospitalization happened during the pandemic versus the pre-pandemic period as determined by the admission date.
Covariates
We selected individual characteristics based on data availability and the Andersen’s Model of Health Care Utilization 35 including predisposing factors (age, sex, and race/ethnicity), socioeconomic factors (Medicare & Medicaid dual coverage ever, disability entitlement ever, patient residence in a rural area) and need characteristics (major diagnostic categories—medical/surgical complicated/non-complicated, indicator of elective procedure, patient Hierarchical Condition Category (HCC) score, and number of hospitalizations in the 12 months prior to the index hospitalization). This information was compiled from Medicare Beneficiary Summary File and EHR data from the care system.
Statistical analysis
We first compared the trends of monthly hospital discharge volume and percentage of discharges to each location between the 24 months of the pre-pandemic period and the 10 months of the pandemic period. We also compared the descriptive statistics of the patient composition in terms of predisposition, socioeconomic, and need factors prior to and during the pandemic. Comparison of the trends and patient composition across years could suggest whether it was appropriate to combine the 2 years’ pre-pandemic period for comparison with the pandemic period in the regression analysis.
We used multinomial logistic regression models to predict the hospital discharge location, with discharge to home with no PAC services as the reference category. We used logistic regression models to predict the likelihood of readmission and mortality in the corresponding time frames. For both groups of the outcomes, the primary predictor was a binary indicator of the pandemic period relative to the pre-pandemic period.
To identify the sources of changes during COVID-19, 3 model specifications were run for each outcome measurement. The first model was unadjusted with only the pandemic time frame as the independent variable. This model captured the overall changes during the pandemic regardless of reasons. The second model was fully adjusted for patient demographics, clinical conditions, admission categories and month and hospital fixed effects to isolate changes due to patient composition shift during the pandemic. Month and hospital fixed effects were coded as 2 sets of dummy indicators to absorb the potential seasonal and hospital level variations. The third model added the interactions of the pandemic timing indicator with all patient-level characteristics and the fixed effects to capture any differentiated responses to the pandemic across patient subgroups, hospitals, and time of the year if any. The differences in the estimated changes of outcome variables before and during the pandemic across the 3 models would suggest the source and the relative share of variation that contributed to the outcome changes during the pandemic.
Further, to estimate the relative changes of mortality and readmission rates prior to and during the pandemic across all discharge locations, additional analysis was performed by partitioning each discharge location category. All statistical analyses were performed using STATA SE 16.0. The predicted probabilities of discharge locations, mortality and readmission rates were calculated using the STATA margin command and were reported as the primary outcomes.
Results
Sociodemographic and clinical characteristics
Our sample included 9448 Medicare beneficiaries with an average age of 78 years old, 56% female, 95% white, 13.6% with Medicaid coverage and 6.9% with disability entitlement. About 70% of the sample lived in the urban areas, 18% in suburban and 12% in rural areas. The average HCC score was 2.9. Sociodemographic characteristics were similar across the time frames studied (Table 1).
Summary statistics of patient characteristics and main outcomes.

Standard deviations (SD) in parentheses. Entries are percentage points unless otherwise noted. Unit data observation is an index hospitalization.
There were 17 909 unique hospital discharges, with some beneficiaries had more than 1 index hospitalizations. The clinical composition for the index hospitalizations changed between the pandemic and the pre-pandemic periods. During the pandemic, there were a greater proportion of hospitalizations in the medical complicated (31.3% vs 26.3%) and surgical (both complicated and non-complicated, 6.2% vs 5.9% and 8.8% vs 7.4%) categories. Medical non-complicated, musculoskeletal surgery, or other procedures were proportionally less frequent during the pandemic. There were also fewer hospitalizations classified as elective procedures during the pandemic (14.1% vs 16.5%). The average payment and length of stay (LOS) per episode of hospitalization were both higher ($13 793 vs 12 524, 4.6 vs 3.9 days) during the pandemic. All results were significant at the P < .05 level (Table 1).
The annualized decline in hospitalization during the pandemic relative to the previous 2 years was 27.0%. The largest decline occurred during the first 3 months after the pandemic began (March–May 2020). In June 2020, the hospitalization rate started to stabilize, but had not recovered to the pre-pandemic volume by the end of the study period (December 2020) (Figure 1).

Monthly discharge volume and percentages by location.
Discharge patterns
The percentages of hospital discharge to alternative locations were relatively stable across years before the pandemic. About 57% of the discharges were to home, 21.5% to SNF, 15% to HHA, 2.5% to IRF and the remaining 4% to hospice or other facilities. During the pandemic, there were more discharges to HHA (20%), slightly more to IRF (3.3%) or others (5.4%), and less to SNF (17.6%) or home (53.7%). After adjusting for patient sociodemographic and clinical characteristics, results showed significantly more discharges to HHA (mean difference 4.6%, 95% Confidence Interval (CI) [3.2%, 6.0%]) during the pandemic than before and fewer discharges to SNF (−3.9%, 95% CI [−5.2%, −2.7%]) or home (−2.8%, 95% CI [−4.4%, −1.3%]). Percentages of discharges to IRF or hospice were also higher during the pandemic than before, but the changes were at a smaller magnitude (IRF 0.71%, 95% CI [0.11%, 1.30%]; Hospice 1.45%, 95% CI [0.75%, 2.16%]). Changes in discharges to other locations were insignificant (Table 2).
Predicted percentages of discharge location (0-100).
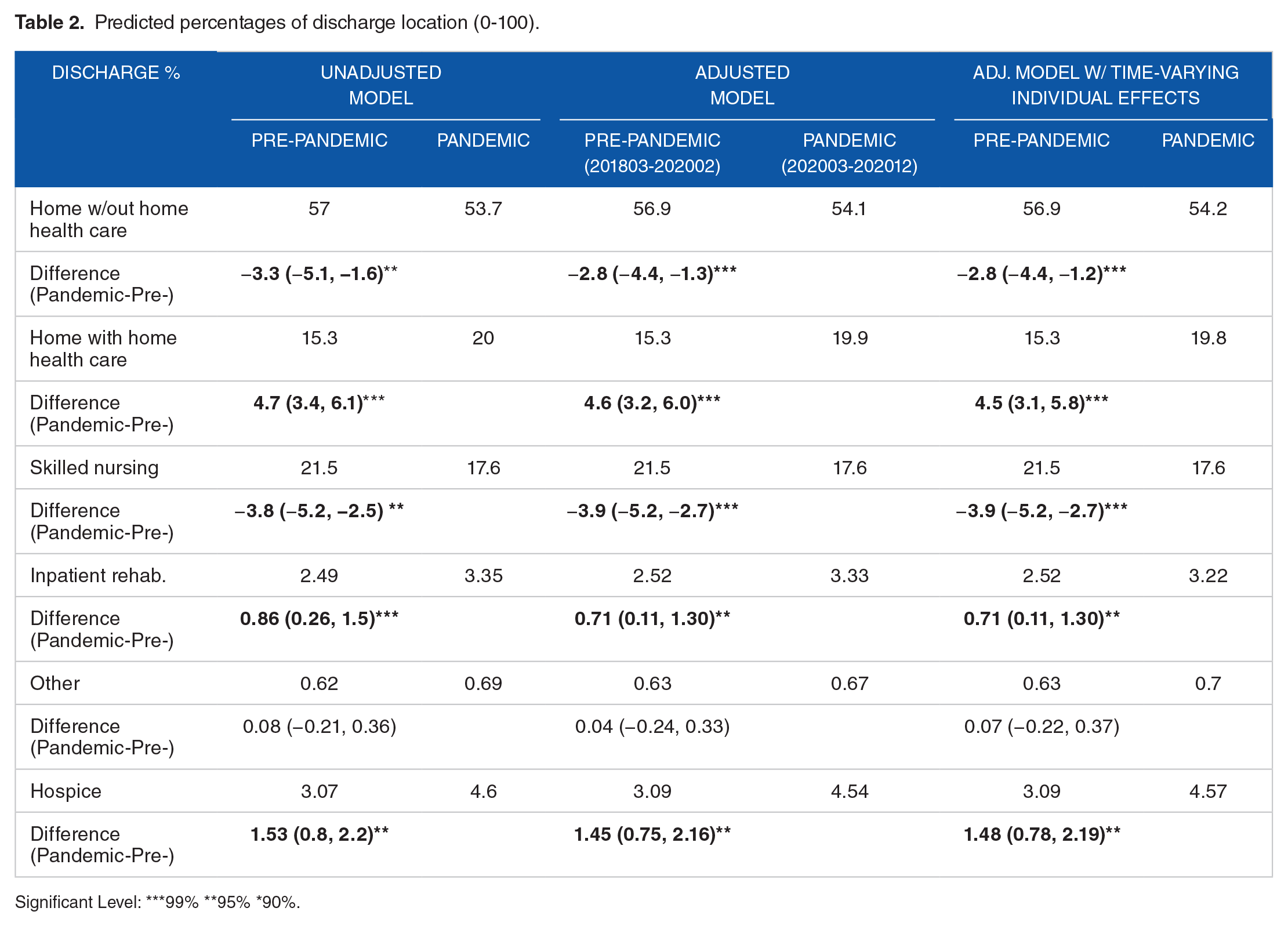
Significant Level: ***99% **95% *90%.
Comparing across the 3 model specifications, results suggested that changes in patient composition explained at most 15% of the changes in the relative discharge patterns (eg, mean differences for home discharge with and without adjustment for patient characteristics were 2.8% vs 3.3%, implying 15% = 1%-2.8%/3.3% of the changes being explained by patient characteristics.). Further, the predictive power of patient characteristics was mainly concentrated on home versus non-home discharges but had little to no influence on discharge patterns across PAC facility types. In addition, the association between patient characteristics and discharge patterns was mainly channeled through the general relationship regardless of the time rather than the differentiated relationship during the pandemic from before (Table 2).
Care outcomes—Mortalities and readmissions
Mortality at 30- and 90-days after discharge were 4.4% and 8.8%, respectively, before the pandemic. There was an absolute increase in 30-day mortality during the pandemic of 2.2% (95% CI [1.4%, 3.0%]), representing a 48% relative increase. Similarly, there was an absolute increase in 90-day mortality of 3.3% (95% CI [2.2%, 4.4%]), representing a 35% relative increase. The magnitude and statistical significance of these differences remained after controlling for patient demographic and clinical characteristics. The differences in mortality rates between the pandemic and the pre-pandemic period started to shrink for the 91 to 180-day interval (1.2%, 95% CI [0.37%, 2%]) and became comparable beyond 180 days (−0.36%, 95% CI [−1.07%, 0.36%]) (Table 3).
Predicted mortality and readmission rates in percentage points (0-100).

Significant Level: ***99% **95% *90%.
Readmission rates were not significantly different between the pandemic and the pre-pandemic period regardless of risk adjustment. The fully adjusted readmission rates during the pandemic were 13.7% for the 30-day rate and 23.4% for the 90-day rate, relative to 14.1% and 24.5% before the pandemic (Table 3).
For both mortality and readmission rates, adding patient characteristics or interactions terms to the model did not substantially change the estimated results. These results suggested that changes in patient composition explained the changes in care outcomes before and during the pandemic very minimally (Table 3).
Predicting outcomes by interacting the pandemic time indicator and the hospital discharge location category, results showed that average mortality and readmission rates increased monotonically as more intensive post-acute care was used (eg, home vs HHA, SNF, IRF). However, comparing before and during the pandemic period, significant differences in 30- or 90-day mortality rates were mainly concentrated among those patients who were discharged to home or to SNF (Table 4).
Predicted 30- and 90-day mortality and readmission rates by discharge location (0-100).

Discussion
This study compared PAC utilization, mortality, and readmission rates after non-COVID hospitalizations during the COVID-19 pandemic in 2020 with that of the preceding 2 years among Medicare beneficiaries 65 years or older who were served by an Accountable Care Organization. There was a 27% annualized decline in non-COVID-19 hospital discharges. Changes in the relative hospital discharge pattern mitigated the overall decline in HHA admissions but exacerbated the decline in SNF admissions. Thirty- and ninety-day mortality rates increased and primarily among those discharged to home and to SNF. Readmission rates did not change significantly. Patients admitted during the pandemic had comparable sociodemographic attributes but worse clinical factors than those admitted before the pandemic. Changes in patient composition accounted for at most 15% of changes in hospital discharge patterns and less than 5% of the changes in mortality rates. Further, the patient composition effects on PAC utilization and outcomes were channeled through the general relationships rather than differentiated responses during the pandemic. Overall, these results suggested that the changes in PAC utilization, mortality, and readmission rates following non-COVID hospitalizations during the pandemic were mainly due to changes in system operation or care practice rather than patient composition.
Our results suggest that the impacts of the COVID-19 pandemic on care delivery and outcomes appear to have been a cumulative process. From the start, patients who were admitted for inpatient hospitalization were found to be less healthy and more medically ill during the pandemic than before. This is a finding consistent with many other studies in the field.7,8,11 But the sociodemographic characteristics before and during the pandemic were still comparable at the hospital admission stage (Table 1). However, when it turned to hospital discharge, decision to use post-acute care and the related care outcomes, influences from the sociodemographic factors started to stand out.7,21
To mitigate the pandemic impact and to address the potential disparities in care delivery and quality outcomes in the long run, more empirical evidence on hospital discharge patterns, the relative efficiency of using alternative types of PAC facilities as well as groups of available PAC facility choices for specific regions and/or subgroups is needed to help the providers, patients, and caregivers make better informed decisions. As a general trend of moving PAC services away from institutional settings,29,36,37,38 the feasibility and accessibility to different facility options is also a practical concern.18,27,30 For example, there are fewer home health agencies in rural than urban areas, rural patients may find it more restricted when making PAC choices.24,25 While all SNFs across the country experienced higher number of case outbreaks during the pandemic,13,20 for some rural patients, SNF might be the only option if any PAC service was needed.17,18,24,25,36 For some patients and families, professional supports were critical when caregiving at home was not an option.11,26,29 Recently developed telemonitoring service might be a solution to the geographic disparities in access to home-based services.18,27,28,30 Regardless, a patient-centered customized roadmap on possible discharge options and expected outcomes will help the interest parties to make complicated medical decisions.
Limitations
This study has a few limitations. First, the study used hospital discharges from a single healthcare system. While this may limit the generalizability of out finding,16,39 focusing on a single healthcare system provides richer clinical data to present a more comprehensive picture of pandemic impacts. Second, our sample size limited the ability to stratify the sample and investigate the differentiated pandemic impacts among subgroups of patients.7,8,21,22 The sample was also predominately white (95%). Third, our study was observational, and we cannot make causal inferences between PAC utilization and outcomes. Leveraging the regional-level data on the prevalence and severity of the pandemic over time could help with causal inferences.2,20 Fourth, this study focused on PAC utilization at the extensive margin, that is, use PAC or not, and general outcomes such as all-cause mortality and readmission. Further research on utilization at the intensive margin (eg, therapy time, length of stay and cost per episode of care, etc.) and service-specific outcomes (eg, functionality improvement, etc.) will provide additional perspectives in the field,11,26,28,40,41 especially given the fact that post-acute care and hospital readmissions are the 2 major drivers for cost variations overall.16,40,42-44 Fifth, as with many studies that used administrative data, this study lacks information from patient perspectives. Additional insights that consider patient and family needs will help to improve patient-centered care services and quality. Sixth, while we controlled for observable factors at patient or admission level we cannot control for unobservable ones, which might also be “worse” during the pandemic than before. Last, with the COVID-19 pandemic lasting over years and going to an end, it would be better to have post-pandemic data to show the trend back to the pre-pandemic levels.
Conclusion
This study highlights major changes in PAC utilization and mortality, but not readmission rates after non-COVID-19 hospital discharge during the pandemic. We investigated possible contributing factors, including changes to the absolute hospital discharge volume, relative discharge patterns, and the patient composition. Our results suggests that changes in hospital discharge patterns were the main drivers of changes in PAC utilization and care outcomes. While changes in patient composition accounted for up to 15% of changes in PAC utilization, most of the changes were attributable to other reasons, such as impacts from the pandemic leading to changes in practice patterns and care delivery, etc.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by research grants P30 AG017266 (Drs. Cao, Wang, Mullahy and Smith) from National Institute on Aging to the Center for Demography of Health and Aging at the University of Wisconsin–Madison; AAI2989 (Dr. Cao) from the Wisconsin Alumni Research Foundation (WARF); and an institutional award (Dr. Liu) from Research to Prevent Blindness, New York City, New York, USA to the University of Wisconsin-Madison’s School of Medicine and Public Health, Department of Ophthalmology and Visual Sciences.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors meet the criteria for authorship stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals. Study concept and design: Cao, Wang, Mullahy and Smith. Acquisition of data: Cao and Smith. Analysis and interpretation of data: all authors. Drafting of the manuscript: Cao and Wang. Critical revision of the manuscript for important intellectual content: all authors.
Sponsor’s Role
The sponsors had no role in design and conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript.