
Abstract
Background:
Therefore, the objective of this study was to elucidate caregivers’ experiences of ordinary homes as a working environment in home care and home health care during the COVID-19 pandemic. At the beginning of the pandemic, hospital care was in focus and the care of older adults was criticized around the world.
Design and methods:
Semi-structured qualitative interviews were conducted in two municipalities in Sweden between March 2020 and May 2021. One large municipality (population 155,000) with experience of care recipients with COVID-19, and a smaller municipality (population 32,000) were included; both had a focus on preventing the spread of the infection. A total of 27 participants working in home care were interviewed; these were occupational therapists, physical therapists, nurses, and assistant nurses. The interview material was analyzed using content analysis.
Results:
The interviews provided a comprehensive insight into the complex work environment in municipal home care during the pandemic. The staff had to deal with constantly changing information and new guidelines. They were also given new tasks and work routines that demanded more planning and were time-consuming. The staff experienced higher workload and pressure during the pandemic and did not have enough time to recover.
Conclusions:
During a pandemic situation, the information must be comprehensive and gathered in one place, and the managers must ensure sufficient staffing levels, time for reflection, and support for prioritization. The managers must also ensure the mental health of staff and meet their needs for recovery, both at and outside work.
Introduction
Internationally, as well as in Sweden, the number of elderly people in the population is increasing, 1 and thus the need for care in the older adult’s home environment is also increasing. One of the most important tasks in current and future health care is to proactively address the challenges related to the marked shift from hospitals to primary care and home care.
This is a challenge, as care and nursing within these sectors of care have historically been described as neither attractive nor safe. 2 In municipal care, assistant nurses, occupational therapists, nurses, and physical therapists provide interventions to older adults with diverse diagnoses and needs in the home if they cannot get to the health center. Some older adults have lifelong needs, others are discharged quickly, and sometimes the whole family is cared for. 3 Home care offers support in various daily activities, such as help with food shopping and cleaning, and support with personal hygiene, clothing, or meals, 4 while home health care rehabilitation and medical interventions. Both home care and home health care make it possible for older people to continue to live at home despite multiple diagnoses that require advanced care. When care is transferred from being offered at the hospital to the older adult’s home environment, a different care focus is required; the adjustment places high demands on a good and safe working environment for the staff. 5
The COVID-19 pandemic has affected citizens of all ages, including older adults who receive municipal care in their own homes. People affected by COVID-19 may need medical care in the acute phase, sometimes hospitalization, and then a period of rehabilitation at home. This put demands on the experience and skills of the staff, on staffing levels, and on the physical work environment. 6
During the early phase of the pandemic, there were shortcomings in protecting the older adult population in Sweden. 7 Crisis management is based on the principle that every person shoulders his/her their responsibility, which means that the government sets recommendations that citizens in the society/municipalities are expected to follow. When the pandemic broke out, there was a lack of awareness about how prepared the municipalities were for a crisis. Deficiencies have emerged in communication channels between authorities and the municipal home care service and home health care. It has also emerged that difficulties arose because care is fragmented, with the regions (health centers and hospitals) providing doctors and specialist care while the municipalities are responsible for general care of older adults. Since the management of home care and home health care is monitored from an authority perspective, it is important to explore how the staff themselves experienced their work environment and their opportunities to follow guidelines during the pandemic.
The aim of this study was therefore to describe health care professionals’ experiences of their work environment in home care and home health care during the COVID-19 pandemic.
Design and methods
A qualitative interview study 8 was conducted with staff in home care (assistant nurses) and home health care (licensed staff: occupational therapists, physical therapists, and nurses).
Setting
The study was conducted in two municipalities in Sweden, of which one was a smaller municipality (approximately 32,000 inhabitants), where assistant nurses, nurses, occupational therapists, and physical therapists worked. The other was a larger municipality (approximately 155,000 inhabitants), where assistant nurses, occupational therapists, and nurses worked, divided into three health care teams and 15 different home care teams from different parts of the municipality.
Population and procedure
A purposive sampling strategy 8 was used: first, information about the study was sent out to the managers of the units in the two municipalities, who in turn informed potential participants. The inclusion criterion was staff in municipal home care or home health care who could be interviewed in Swedish. Of those staff members receiving the invitation to participate in the interview, 35 accepted. Of these, three people did not meet the inclusion criteria, two declined when the interviewer called, and three did not answer the call (Figure 1).

Flow chart showing the selection of participants and the total number of participants after dropout.
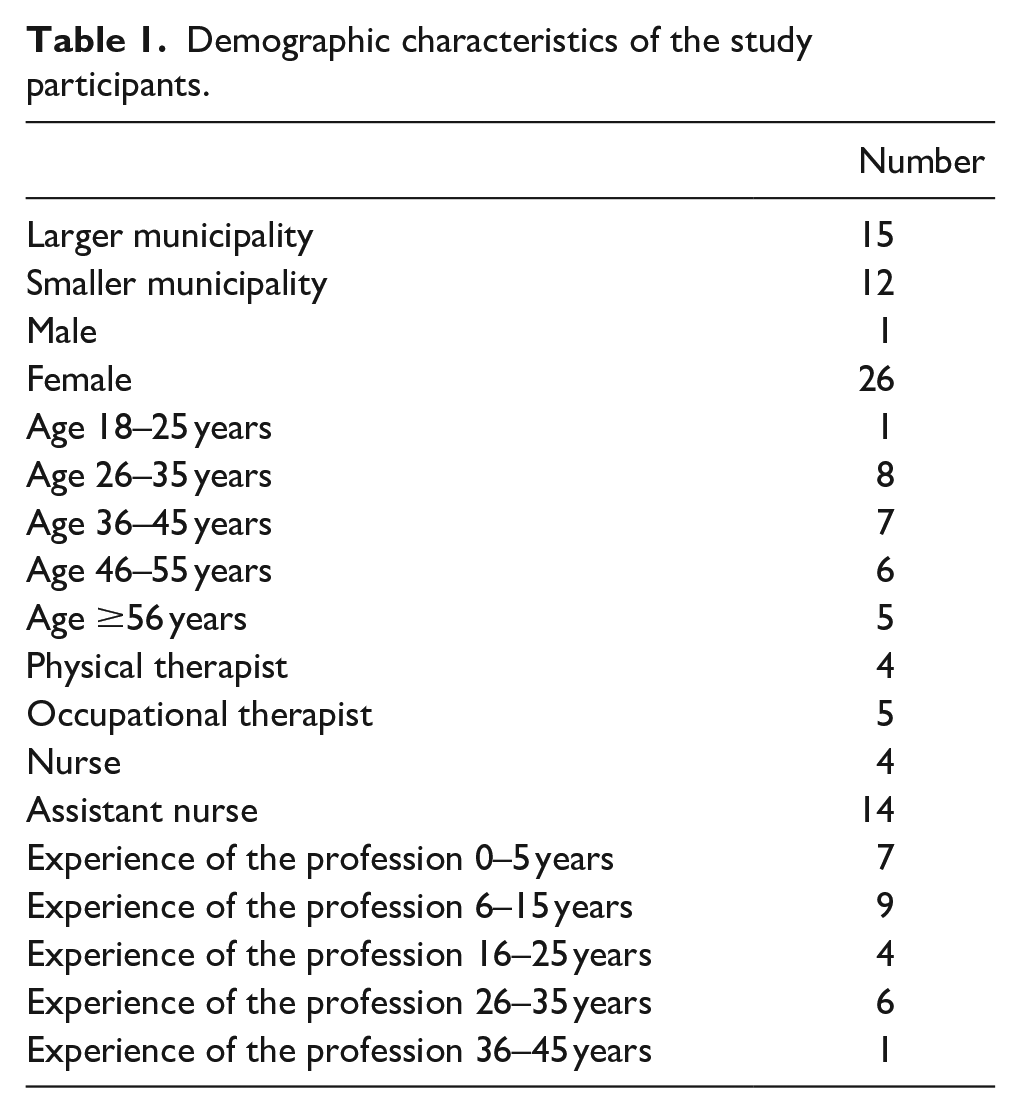
Thus, a total of 27 employees with different professions participated: assistant nurses, nurses, occupational therapists, and physical therapists (Table 1). There was an even distribution of participants from the two municipalities. Semi-structured telephone interviews were conducted by a professional interviewer between March 2020 and May 2021. The interviews were based on a question guide that focused on the physical work environment in ordinary homes, what it was like to carry out care and nursing interventions with older adults in the home, how pandemic guidelines and recommendations affected the staff, and how the staff described their physical and psychosocial health when they were at work. The interviews lasted 15–30 min. Background information was obtained during the telephone interview, with questions about the participant’s age, gender, and education, and whether they worked in home care or home health care.
Demographic characteristics of the study participants.
Data analysis
The interviews were transcribed by a professional transcriber and analyzed with content analysis according to Graneheim and Lundman, 9 with a focus on the manifest content. The authors listened to the interviews and read the transcripts several times to familiarize themselves with the content. Thereafter, the analysis was performed in several steps. The text was divided into meaning units that corresponded to the purpose, and the surrounding text was included to maintain the context from which the meaning units came. These were condensed to make them easier to handle. The condensed meaning units were coded and grouped into subcategories according to their content. Overall categories were then formed, based on the similarities and differences between the subcategories. The data analysis was performed interactively by the first and last author followed by reconciliation in collaboration with the author group. Examples of the analysis procedure are described in Table 2.
An example of the analysis process.

Ethical considerations
The Swedish Ethical Review Authority approved the study (approval no. 2020-05222). The target group for the study is vulnerable, based on their position of dependence as employees in municipal health care, which is why special emphasis was placed on stressing that participation was voluntary and confidentiality was assured.
Results
The analysis of the results showed that it was not possible to distinguish between the physical and psychosocial work environment; they constantly affected each other. Furthermore, it emerged that the two municipalities were in different stages of the pandemic when the data collection took place, which means that different perspectives on working in a pandemic were captured. The smaller municipality had not had any older adults with COVID-19, but rather focused on preventing the spread of infection, while the larger municipality had gone through the first wave when the interviews were conducted.
The analysis generated five categories and 12 subcategories, which describe the participants’ experiences of the work environment in older adults’ homes during the COVID-19 pandemic. The categories concerned handling a large amount of information during the pandemic, adapting their working methods, making extra efforts, being worried about the infection, and finding that their recuperation was affected.
In the quotations below, the following abbreviations are used: AN, assistant nurse; RN, nurse; OT, occupational therapist; and PT, physical therapist.
Being able to interpret and handle comprehensive information and different guidelines under constant change
The staff received written and practical information about updates to guidelines, but they did not always comply with the guidelines. The participants had been informed about the infection situation and were given support for managing and interpreting all the information.
Dealing with the tidal wave of information is risky and time-consuming
The written information about what the health personnel were supposed to do was given in various ways. In some units, particular staff members were designated to read and disseminate the latest information, and the safety representatives shared information from trade unions. The municipality disseminated central information via its website. Another way to access information was through links to the Communicable Diseases Unit and the Public Health Agency via the medical records system. One nurse said:
There is a link to another information page via the medical records system, but the link isn’t updated at the same rate as the information. So the managers send an email (. . .), but then you have to find that email to get the latest update. (RN 4)
The pandemic meant a large flow of information for everyone. The participants said that they were overwhelmed with emails, in which there could be small changes in the guidelines. To improve the work environment, the manager marked what had changed in the information. However, the staff lacked information about which activities were in operation and which services they could offer the older adults. They felt inadequate when they noted an increase in mental ill health among the care recipients. At meetings, employees received practical information and were shown how to use protective equipment, which was clearer than just reading the instructions. They were also given training on COVID-19, they were tested on basic hygiene and shown films on handling protective equipment to ensure their competence. It was time-consuming for the staff but they perceived it as good to be able to update their skills. The advantage of digital training was that they could rehearse and bring themselves up to date quickly when needed. To get information about the spread of infection in the municipality, the staff had a review of the infection situation at the unit every morning and afternoon. At the daily meetings, the content of the day’s home visits was prioritized with the support of the manager, something that was perceived as valuable, especially at the beginning of the pandemic. At these meetings, it was also verified that everyone had been informed in the event of an infection. Nurses and unit heads had a great responsibility, but it was not clear who they should inform. “It is always a problem when you get a positive [case], how the infection tracking should be done and who you are supposed to notify.” (RN 4)
Despite the fact that the staff received information, they did not always comply with the routines during the pandemic. The difficulties were often attributed to a lack of communication and rapidly changing routines. There was a risk of missing information if the group did not meet every morning for the exchange of information about what was currently happening. Licensed staff said that communication about the spread of infection was lacking and that the assistant nurses did not always use face masks in a correct way and worked in private clothes. Rehabilitation staff had discussions with managers about whether protective equipment should be used in training temporary staff in patient transfers. The routines were interpreted differently. “The managers didn’t give support, they think we should carry on as usual as long as everyone was healthy.” (PT4)
Receiving support in handling and interpreting information about guidelines
The unit managers were described as available, they supported their staff and encouraged them to talk, and they were involved in everything that happened. They tried to support the staff in interpreting routines and telling them how to do things in practice. Some participants felt that they were doing well on their own, while others felt an increased need for support from the manager. The need for support depended on their relationship with the manager: if a good relationship was lacking, the employee preferred to turn to colleagues for support and information.
Balancing and adapting a work situation in constant change
Work methods in the home care premises were changed to be able to maintain physical distance and good hygiene, but it affected the encounter with the care recipient negatively.
Having to change working methods to reduce the spread of infection and at the same time protect the older adult’s home environment
During the pandemic, guidelines and routines gradually changed and the participants commented that it took too long before the restrictions were tightened. Routines for disinfecting shared surfaces such as sinks, computers, telephones, and keys were clarified. The new guidelines for the home care environment meant that staff were expected to wear work clothes throughout the work shift and use face masks in the office when there were several colleagues on the premises. To maintain distance from each other, colleagues spread out around the tables and were not allowed to walk between different group rooms on the premises. To limit the number of staff members in the unit, changing rooms were converted into workrooms, breaks were staggered, and some staff members chose to eat in their office. Meetings were held digitally, which saved time; it was easy to just connect to the Internet to participate. But the social environment at work was affected:
Some have chosen to go for a walk, or do something else. We take turns to eat, so we don’t sit together any more and eat, which I think is very boring and a pity because it is the social part that you want. (OT5)
In the smaller municipality, the participants said that the routines for driving a car were changed: to maintain distance, no more than two colleagues were allowed in the car, one sitting in the back while the other sat in the front; both should wear face masks. Carpooling meant more planning, as they needed cars with rear seats. To maintain good hygiene in the car, the gear lever and steering wheel was disinfected after each trip. The cars were also equipped with disposal bags and extra sets of protective equipment, in case staff members forgot to bring their own.
The working environment at the homes of the older adults could be deficient because it is also a home environment, where the employee needed to adapt to those who lived there. The staff were required to be resourceful and at the same time respect the older adult’s home environment. Many said that they did not do anything different in the home environment as a result of the pandemic, but activities were conducted where the care recipient was located; it was not possible to be in other rooms. However, in connection with widespread infection in a household with many family members in a small area, activities had to be conducted outside the home so as not to risk the spread of infection.
According to the guidelines, there should be sterile surfaces in connection with cleaning of protective equipment. Sometimes it could be difficult to find good countertops, as they could be made of wood, be dirty, or have grooves; in these cases, plastic trays were bought to facilitate disinfecting the visor. Often, a place was prepared in the hall, and sometimes the kitchen was used. The kitchen might be located at the far end of the home, which meant that the employee had to walk through the entire house without protective equipment before or after the intervention with the older adult.
Adopting new strategies for safe care
During the pandemic, the employee would always wear protective equipment in the older adult’s home, but in the beginning there was no equipment. Some units, but not all, planned extra time for handling protective equipment during visits. The routines for the protective equipment were interpreted differently and changed rapidly. There were differences in which protective equipment was used and how it was handled, whether it was put on in or outside the home, and where the material was then disposed of or cleaned. Using the protective equipment caused physical problems in the work environment. Participants said that they needed to manage it outside the home and it could be cold to clean the equipment in the cars in winter:
In the winter we go in short sleeves (. . .). We don’t wash at their home, so we have had water in the car and soap and sanitizer and then minus 17 degrees on top of that. It has been really difficult. (AN10)
It also emerged that when the staff members used face masks, their spectacles misted up and slid down, which meant a greater risk of touching their faces. It could be difficult to administer eye drops when the visor misted up. Using protective equipment also meant that mobility decreased. It was difficult for them to get down on the floor to adjust aids when wearing full protective equipment.
The protective equipment also affected the encounter with the older adult. All professionals emphasized that the care recipients commented that it was difficult not being able to see who was behind the mask. They could become anxious and had difficulty recognizing the staff:
They do not see our mouths, they only see our eyes and they can’t keep track of us in the same way (. . .). Now everyone merges into one, so I understand that those with dementia who live at home may find it uncomfortable when we put the visor on. (PT3)
The protective equipment also affected the encounter if someone had a hearing loss. Communication became more difficult and took more time when the older adult could not read the employee’s lips and facial expressions. Face masks and visors blocked much of the sound during conversations, which meant having to repeat themselves several times and to raise their voices or shout to be heard, so they sometimes took off their equipment and kept their distance while talking instead. It became even more difficult to communicate if the older adult had a different mother tongue. Other strategies the staff used were to speak slowly and clearly and to repeat information. Despite this, misunderstandings arose and the older adult sometimes ended the conversation when they could no longer bear straining to hear. One participant described similar difficulties for care staff with hearing loss, as both the older adult and the employee’s colleagues had face masks during home visits. This employee therefore chose a visor instead of a face mask, so that lipreading was possible.
New measures required planning and more time
The staff in both home care and home health care were given new tasks that required more planning, and other measures were dropped. Quick decisions were required, which made collaboration with primary care unclear.
The spread of infection meant new tasks
Many participants felt that they carried out their work in the same way as before the pandemic. However, the physical therapists said that they were preparing new care programs for exercise and repositioning, taking account of COVID-19, and that they had to take courses in breathing exercises to be prepared. They said that the exercises needed to be dosed in a new way and that oxygenation was monitored when the older adult had had COVID-19.
At the hospital, isolated areas were used for infectious diseases, and therefore the nurses were given the responsibility for creating a clean and contaminated side in the hall of the older adult’s home to reduce the risk of spreading the infection. The nurses gave everyone who had COVID-19 Fragmin injections and they performed polymerase chain reaction (PCR) tests to a greater extent than before the pandemic. The nurses administered more drips and carried out more medical interventions because more of the older adults were more ill. This affected the nurses’ work environment when they needed to cycle with equipment, such as drip stands. It also emerged that licensed personnel were given responsibility for taking care of the central stock of protective equipment that was distributed to other units, which was time-consuming. During the pandemic, those over the age of 70 were advised not to go to stores or environments where there was a risk of crowds, which meant more work for the assistant nurses. “It is clients who have received approval for assistance during this period, due to these reasons, who receive help with shopping.” (AN5)
When the canteens at the retirement homes closed, the assistant nurses helped to deliver the food to the homes of those who used to eat in the canteens. Relatives were advised not to visit their relatives. However, the assistant nurses felt that they could not meet the needs of the older adults that arose when they were alone after a long time in isolation and missed spending time together.
Planning the working day to be ready for the unexpected
The pandemic affected how licensed staff planned their days, to be ready for the unexpected and to have time to plan for visits. “You cover all the time and rebook your patients. You say that you’ll be in touch (. . .) You have it completely open in your calendar and book more for each day.” (PT2)
The participants planned all transfers during home visits and consciously kept their distance unless close body contact was required. Before the home visits, the staff member called and asked how the older person was feeling. In case of cold symptoms, the nurse made a quick visit for sampling, and in the case of positive results, an assessment was made as to whether there was a need to move the care recipient to the COVID ward. If an older adult was suspected of being infected, the assistant nurses chose to postpone cleaning and laundry tasks while waiting for the test results. Occupational therapists and physical therapists waited or postponed visits except for urgent matters to meet the older adult’s basic needs and visits to facilitate the staff’s work environment when infection was confirmed. The occupational therapists said that they also reviewed the supplies at the units to be ready if they needed to quickly bring aids the same day when an older adult fell ill and remained at home. “What aids should we have in stock? (. . .) And then we ordered electric backrests for the bed for our storeroom, because COVID patients’ breathing is often affected.” (OT2)
This affected their work environment because they did not have a car or time to wait for home delivery but had to carry and transport heavy aids on a bicycle cart.
Care recipients with COVID-19 needed urgent visits, which meant that other things were planned out. One nurse said that the delegations were extended automatically and preventive measures such as health interviews, risk assessments, and drug reviews were canceled. It also emerged that the older adults planned their care and prioritized visits by the home care service or a nurse, declining rehabilitation visits to reduce the number of people in their home.
Unclear collaboration between primary care and home health care generated more work
At the beginning of the pandemic, all citizens over the age of 70 were advised to self-isolate. In order for them not to have to go to the health center, older adults were referred to home health care. The health center did not take into account that it meant increased costs for the older adult, and the home health care service did not cope with the sudden increase in enrolled patients. It also emerged that older people wanted home health care in order not to have to go to the health center.
The nurses said that they were quick to vaccinate their enrolled patients. Thereafter, the health center and the municipality agreed that they would help vaccinate older adults who only received, for example, alarms or help with shopping. The municipality then had to start up its own vaccination team, something that took time from their regular work, as one nurse explained about the intensive process to quickly vaccinate as many as possible. Health declarations had to be sent to the health center that prescribed the vaccine before the injection could be given. “I don’t think they understood how much work it would actually be with this when they said yes at the beginning.” (RN3)
Worry about becoming infected and passing on the infection
The staff’s worries varied and they had different ways of managing their concern. Care recipients and relatives were also worried, which affected the staff’s work environment.
The staff handled their concerns in various ways
It was clear that the participants saw the risk of becoming infected as part of their work. “In November I got infected, but I’m not really worried, it’s more natural because of my work, I can’t do much more.” (AN9)
Several participants said that they did not experience anxiety for their own sake; however, they were concerned about infecting someone else or bringing the infection to the older adults. Their anxiety was greatest in the beginning when everything was new and they thought about how many were infected and how many died. The mass media contributed to their worries and they could no longer follow the news. Their anxiety also increased when they were physically close to the older adult or to colleagues who had sudden symptoms. Nevertheless, the participants agreed that they became calmer with knowledge and experience of the pandemic.
To deal with staff concerns, managers were quick to initiate infection tracking, share information from the employer, and offer support conversations. In the smaller municipality, there were quick tests at the workplace that they could choose to use in connection with each work shift, which were perceived as providing security. The participants said that they were given a telephone number that they could call to talk, but felt it could be difficult to talk to a stranger about the fear of taking home the infection; most participants preferred to talk to their colleagues or acquaintances. They also pointed out that they talked so much about COVID-19 that they finally had to decide that they would talk about something else to support their well-being. The longer the pandemic lasted, the more they followed the hygiene guidelines and kept their distance automatically, which meant that they relaxed and their anxiety decreased. It also decreased as more people in the community were vaccinated.
The older adults and relatives became anxious and made demands on the staff
The protective equipment contributed to a feeling of security for the staff in their work at the older adults’ homes. But the care recipients’ worry increased when the local newspaper wrote that staff did not use protective equipment correctly. “I feel really sorry for the patients where a lot of home care staff are running around who don’t give a damn about this protective equipment. (. . .) They are then really vulnerable because they still need to receive help.” (RN4)
Relatives were worried and wanted answers to questions about protective equipment. They checked that the care staff took care of their basic hygiene, demanded that they disinfect door handles before touching them, and that they wore face masks. Some relatives bought protective equipment themselves for the staff, even before the restrictions came. To instill confidence, the staff clearly showed that they used hand disinfection and explained how they worked with protective equipment.
Not all care recipients adapted to everyday life after infection
The participants said that relatives could not or did not want to visit the older adult during the pandemic, which worsened the cooperation with relatives who normally contributed greatly to the care of their close family member. The staff respected the fact that relatives were concerned about their loved ones; the staff tried to maintain normal relationships and limited the number of staff who came to the home. Relatives called to receive information, which sometimes resulted in the visits being carried out, even though they had initially canceled the visit.
The opposite also emerged, that some relatives did not keep their distance during home visits, or that they visited their family member in the company of friends without protective equipment. It did not feel right to the staff when everyone else was being careful. “Some relatives are inconsiderate (. . .) They have no respect. But we have no right or obligation to tell them so, as it is their parents’ home.” (AN8)
Participants said that the infection sometimes came via relatives. But there were also participants who said that assistant nurses infected the older adult, which angered the relatives because they had struggled with isolation.
Opportunities and effective strategies for recuperation varied
The participants’ recovery varied during the pandemic: some had functioning strategies in place already, while others had difficulty recuperating between shifts.
Having strategies for recuperating and gaining energy
Participants who already had strategies could recuperate even during the pandemic. They felt that they had a balance between rest and work and could stop thinking about work when they were at home. Many of those who experienced good recuperation linked it to active leisure time with pets in an outdoor environment. They tried to see the positive in everyday life and gained energy from supporting the older adults who were otherwise alone. The staff were not allowed to hug the care recipients but were able to provide physical contact during nursing. “It feels so important. And that they get to look you in the eyes and talk to you, it also gives you energy that you get to be the person who can give it.” (AN5)
Putting duties first and not having time to recuperate
Common to all professions was that everyone supported their colleagues. Some worked extra shifts, worked overtime or were called in during their free time, with no time to recuperate between shifts. It emerged that assistant nurses with symptoms were encouraged to work because it was difficult to get temporary substitutes. When there were no substitutes, planning needed to be compressed and the stress increased. The assistant nurses say that they were calm with the care recipients, and that the stress hit them as soon as the door to the person’s home was closed. When the staff members were tired, there were more conflicts in the work groups. Licensed staff felt that they could make priority lists and plan to reduce stress, but felt that it was worse for the assistant nurses.
However, licensed staff said that they had a great responsibility, which meant more to think about and that they worked under great pressure for a long time. It was not enough to get support from colleagues who gave piecemeal help; this did not reduce the responsibility. Instead, the consequences came afterward when their regular colleagues returned.
When XX came and helped me and took over the responsibility, then I felt very tired, it was too much for me, when I woke up on the weekend my heart started beating at once, I got a really high pulse and I felt that two days of recuperation, that’s not enough. (RN1)
A woman said that when her colleague returned and she relaxed, her brain did not work in the same fast way as before and every little change felt burdensome to take on. The participants found that they thought about work and had difficulty sleeping. They reported prolonged fatigue due to the flexibility required to cover for each other.
Participants commented that the focus was on the work instead of on the employee’s health. One assistant nurse said that they needed to adjust their days off according to the schedule, and their requests for leave were often denied. Assistant nurses also said that the manager stated that the work comes first, which was tough to hear as an employee. But there were also participants who said that it could be stressful to be at home, especially for single parents, as it meant a financial impact because of the loss of salary. Absence also generated feelings of guilt because they knew that their colleagues had a higher workload.
Another aspect that affected their recuperation was that the protective equipment gave them headaches and increased fatigue. They felt it was nice to be spared the equipment when they were off duty.
When the focus returns to finances, staff stress increases
During the pandemic, the managers understood that the work took longer, and they planned more time in service between visits to create spaces in the schedule. They also had greater acceptance of work that could not be carried out, when visits were not made. However, the participants felt that, when the new routines became normal practice, the pandemic was forgotten, which meant that the organization largely focused on the finances again. “Now I don’t mean my manager but my manager’s manager. They’re on to us, it’s about finances a lot now, now it’s kind of forgotten, this [pandemic].” (AN3)
The assistant nurses said that, when the extra travel time was removed, their stress increased with the lack of staff. The staff saw that there was no plan or resources, which made them experience the situation as unsustainable, and several said that they were considering resigning.
Discussion
The purpose of the current study was to describe care staff experiences of the work environment in home care and home health care during the COVID-19 pandemic. The results show that, despite the strained work environment, the staff had a strong commitment to the older adults’ situation and health.
The uncertain work situation during the pandemic meant that staff in home care or home health care received new information all the time. It became a working environment problem to handle all information that was communicated in different ways. The results also show that the lack of knowledge early in the pandemic created anxiety among the staff, and they appreciated having close contact with their unit managers to handle information and prioritize tasks. Previous studies have shown that unit managers need to take greater responsibility for managing information 10 and finding creative solutions with the support of technology to create a good working environment. 11 Everyone needs to get the same updated information with clear expectations in order to create a good working environment. 12 This is in line with other research2,13 suggesting that the working environment will be better if the employees can manage changes and, together with the manager, define their needs and make decisions about their work. Furthermore, the organization must show appreciation by offering initiatives that generate positive feelings of being on the same path toward the goals, so that the employees can find the energy to persevere. 13
Home care can be seen as a complex care context with a large geographical spread and different home environments, which makes it difficult to create care environments for controlled interventions. Thus, studies are needed to describe this context. 2 The results of our study therefore contribute important insights into the handling of challenges in a variety of care environments in the form of ordinary homes of older adults during the COVID-19 pandemic.
In home care, the employee often works alone with the older adult, and in situations of great tension, care staff do not always have time to deal with their emotions. In our study, it emerged that they appreciated the support of a manager who was actively involved. They also emphasized that support from colleagues is important for feeling in control and that the workload has to be manageable. Previous studies have shown that transformative leadership, where managers and employees interact, increases well-being and job satisfaction. 14 Thus, feedback is of great importance for the employee to develop in a positive and safe working environment. 15 The manager needs to be there to talk to, to support staff with feedback and reflection.10,12,14 To be able to do this, the unit managers need skills for such conversations, as well as a leadership style that inspires and stimulates the employees.
The results of our study show that the working environment of licensed staff was greatly affected during the COVID-19 pandemic, when a great deal of responsibility fell on them, with long-term consequences. This is similar to previous studies focusing on intensive care, which recommend that recuperation in the workplace should be provided to protect the health of the staff. In situations with a high workload, the organization has a responsibility to ease the burden by making and communicating decisions about how the staff should work instead of placing that responsibility on them. 10
Our results showed that the employees were stressed and several had considered quitting when they could no longer bear it. Their stress increased further with the focus on time and finances. Previous research has shown that factors that create stress are a loss of control and self-determination, role conflicts, and a fear of missing something, 16 factors that in our study were shown to be exacerbated during the pandemic. Strategies for managing stress can include taking help from each other and being in the moment, 17 something that the participants in our study also described as important. Since it is a great challenge to be able to staff a growing need for home care and home healthcare, it is important to safeguard existing staff. The work environment in particular should be examined, as it affects the employee’s attitude to work. 13 Previous research has identified the following important factors for employees choosing to stay in their workplace: a reasonable workload, the opportunity to influence their working conditions and schedule, training in order to be confident with their work tasks, and support from their employer and colleagues. 18
The results of our study show that the older adults refrained from accepting visits, isolated themselves at home, and ceased to have activities outside the home. In order to maintain patient safety for the activities that cannot be canceled, certain visits could be replaced by technology, such as electronic pill dispensers that give a signal to staff who can call to remind an older adult who forgets to take their medication. 11 Digital meetings can also be an alternative for having prompt contact without physical visits. 19 This gives the employee the opportunity to decide their own workplace and it saves travel time, thus easing the workload. Digital training groups for older adults who are isolated has also been shown to give good results, both in terms of physical ability and quality of life. 20
With regard to methodological limitations in our study, the time when the data collection was carried out is important for the result. In the smaller municipality, the interviews began before the spread of infection accelerated, and it became clear that, apart from protective equipment, the employees were working as usual. When data collection began with the employees in the larger municipality, they had already had the first wave of COVID-19 and many experienced the consequences of having worked for a long time in a stressful work environment. This can be seen as a shortcoming, as not all participants had had experience of working with older adults who had had COVID-19, but it can also be seen as a strength, since several perspectives on working in a pandemic were thus captured.
The interviews were conducted by an external person who was not involved in the project. One advantage was that the person did not influence the interviews through personal experience of care work but instead had extensive experience of conducting interviews. If a person with experience of care work had conducted the interviews, more in-depth follow-up questions could have been asked. However, the topic was well covered by the use of a structured interview guide, with several reconciliations between the interviewer and the last author. Djerf-Pierre and Wängnerud 21 highlight the fact that women have a greater level of worry than men when it comes to social risks and threats in society. Only one man participated in our study, which means that the male perspective may have been missed. However, it was a representative sample for home care, which has a female-dominated workforce.
Conclusion
The working environment for all the professions was affected by the pandemic but in different ways. The rehabilitation staff canceled many visits, while the nurses had an increased workload. In the event of future crises, information should be gathered in one place to quickly find the relevant information. The organizations need to ensure that staffing is adapted to the workload and that recuperation is safeguarded, both within and outside the workplace. Handling protective equipment correctly took time, and this needs to be resolved for the assistant nurses, whose time is planned by someone else. When an entire group of citizens in society is recommended to stay at home, it means that they need more support from assistant nurses for activities outside the home; thus, they also need to have the resources in terms of time and staffing. When future homes are built, the space in the hall needs to be large enough to enable the handling of protective equipment, and it is an advantage if the kitchen is adjacent to the entrance.
The results of this study show what it was like to work during a pandemic. Future studies should also examine unit managers’ experience of the working environment during the pandemic and employees’ experiences of how it could have worked differently. There is also reason to further explore mental illness and the consequences of the lack of recuperation from a long-term perspective.
Footnotes
Acknowledgements
We would like to give our most sincere thanks to the employees who participated in this study.
Author contributions
H.W. and C.P. planned the initial study protocol. A professional interviewer conducted the interviews. All authors participated in the analysis. S.T. and C.P. had the major responsibility for the analysis process and writing the manuscript. All authors contributed to the writing of the final version of the manuscript and agree with the content of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by AFA Insurance (award no. 200226).
Ethical approval
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article. The Swedish Ethical Review Authority approved the study (approval no. 2020-05222).
Significance for public health
In the context of the transition to close care as well as the aging-in-place trend worldwide, this study illuminates how the working environment was affected by the COVID-19 pandemic, based on individual structured interviews with health care professionals working in home care and home health care. The findings show that the pandemic demanded a high degree of flexibility, quick decisions, and changed routines. These experiences can be used by employers to prepare for future crisis situations and support their staff. Sweden has an aging population, and an increasing amount of advanced care is offered in the care receivers’ home. Therefore, these findings should be considered in the architectural design of future housing intended for older adults to provide a good working environment for the care staff.
Availability of data and material
All data generated or analyzed during this study are included in this published article.