
Abstract
Home health and home care (HH&HC) agencies provide essential medical and supportive services to elders and people with disabilities, enabling them to live at home. Home-based care is an important alternative to facility-based care, especially for infection prevention during the COVID-19 pandemic. The majority of the HH&HC workforce is comprised of aides, who also are vulnerable to COVID-19. There are limited data on the COVID-19 experience of HH&HC agencies, clients and aides. A survey of Massachusetts HH&HC agency managers was conducted June 1 to 30, 2020 to assess the impact of COVID-19 on agencies, clients, and aides early in the pandemic and to identify needs for future pandemic planning. Of the 94 agencies with completed surveys, most (59.6%) provided services to clients with COVID-19 and 3-quarters (73.7%) employed aides who tested positive for COVID-19, were symptomatic, and/or quarantined. Most agencies (98.7%) experienced a decrease in demand for home visits, reflecting clients’ concern about infection, family members assuming care duties, and/or aides being unavailable for work. Simultaneously, managers’ workloads increased to develop more extensive infection prevention policies, procedures and workforce training and sourcing scarce personal protective equipment (PPE). The COVID-19 pandemic imposed substantial new infection prevention responsibilities on HH&HC agencies, clients, and aides. Specific HH&HC needs for future pandemic planning include complete information on the infection status of clients; ready access to affordable PPE and disinfectants; and guidance, tools, and training tailored for the industry. HH&HC should be incorporated more fully into comprehensive healthcare and public health pandemic planning.
Keywords
Introduction
Home health and home care (HH&HC) agencies provide home-based medical and supportive services that can be important alternatives to hospitals and nursing homes, especially during a pandemic, 1 yet HH&HC has often been overlooked in healthcare pandemic planning.2-4 Most HH&HC clients (also called patients or consumers) are ≥65 years with increased risk of severe illness from COVID-19. HH&HC aides, the industry’s largest occupational group, provide direct care in clients’ homes and have increased COVID-19 risk from work and from community experiences of social and health inequities.2,4 Massachusetts HH&HC agency managers were surveyed during June 1 to 30, 2020 to assess the impact of COVID-19 on agencies early in the pandemic and to identify industry and workforce needs for future pandemic planning.
Methods
A survey of Massachusetts HH&HC managers was conducted to assess COVID-19 impacts experienced by their agencies, workforce, and clients during the early phase of the pandemic (March 1-June 30, 2020). All study protocols and materials were approved by the University of Massachusetts Lowell Institutional Review Board, approval number 19-112-QUI-XPD. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants, as part of the electronic survey process. To further minimize risk the survey was anonymous and therefore contained no personal identifiers.
The anonymous online survey administration also was designed to encourage agency managers to be candid. The survey link was sent in a cover email to managers in 274 agencies, the majority of all of the HH&HC agencies in Massachusetts, by the leadership of the 2 major industry associations and by the state elder services association that contracted their services. Survey instructions specified that it was to be completed by 1 manager per agency. Friendly reminder emails, including the survey link, were sent 1 and 2 weeks later by the industry and elder services leadership. The survey contained 28 items, some with sub-items, in closed-ended multiple choice format with a final open-ended option to capture experiences not directly queried. The survey was self-administered on a smart phone, tablet, or computer, requiring 15 to 20 minutes to complete, and was managed using Qualtrics survey software (version 2019; Qualtrics Institute, Provo, UT, USA).
Survey question responses were checked for completeness and internal consistency. The results for each survey item were calculated as the percent of valid responses for that item and its 95% confidence interval. All data quality control and analyses were performed using SAS statistical software (version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
A total of 116 surveys were returned (response rate 42%). Of these, 22 surveys had substantial amounts of missing information and were eliminated from further analyses. Final analyses were performed on 94 surveys, which had responses to nearly all survey questions. These completed surveys were from agencies that collectively employed 14,272 aides and provided care to 46,633 clients in the month prior to the pandemic shut down. Services to these clients were funded through a wide range of healthcare and social assistance programs, including those based on Medicare/Medicaid reimbursement, other healthcare insurance and private pay.
Most agencies (80.9%) reported that the number of hours of visits by aides to clients declined, for several reasons (Table 1). Virtually all agency managers (98.7%) reported that clients canceled visits due to concern that aides would expose them to the coronavirus and a majority (64.5%) reported that family members assumed direct care tasks that had been provided by aides pre-pandemic. A majority of agency managers (65.8%) reported that home visit hours also decreased because aides employed by their agency were COVID-19 positive, symptomatic, and/or in quarantine. About 3-quarters of agency managers (73.7%) reported that aides were concerned about going into homes and being infected by clients and a majority (61.8%) reported a decrease in client visit hours due to aides not working because they received unemployment or family leave benefits. During the same period, nearly all respondents (85.1%) reported an increase in managers’ time spent developing new policies, procedures, and training, and 2-thirds (67.0%) reported an increase in time spent scheduling.
COVID-19 Pandemic Impacts on Home Health and Home Care Agencies, Managers, Aides, and Clients, a Massachusetts USA, March to June, 2020.
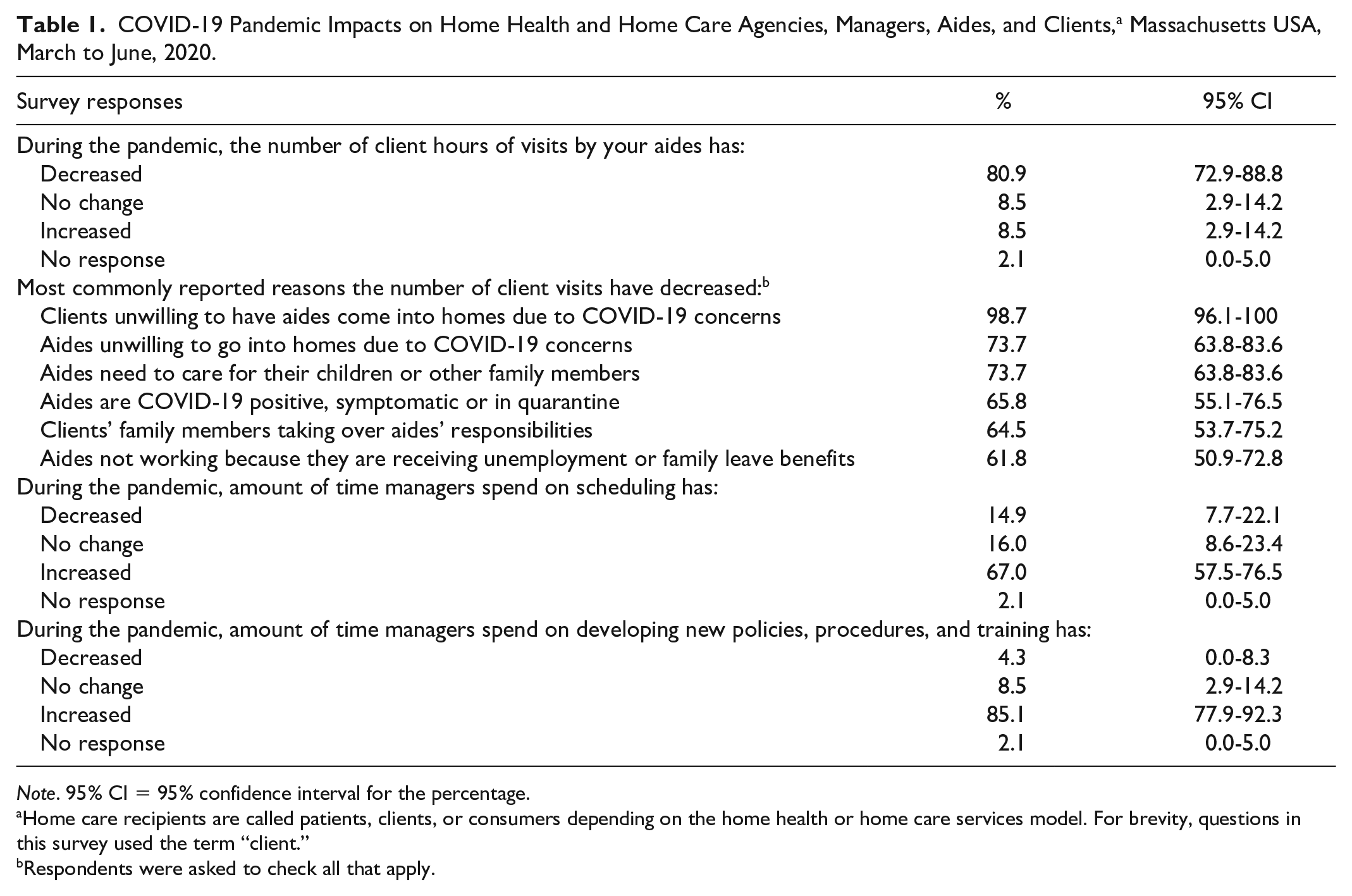
Note. 95% CI = 95% confidence interval for the percentage.
Home care recipients are called patients, clients, or consumers depending on the home health or home care services model. For brevity, questions in this survey used the term “client.”
Respondents were asked to check all that apply.
A majority (59.6%) of managers reported that their agencies had provided aide visits to clients who tested positive or had COVID-19 symptoms (Table 2). Only half (53.8%) reported that their agency always received information on the COVID-19 status of a client, while 39.8% reported that their agencies only sometimes received this information. About 3-quarters of managers reported that aides employed by their agencies had tested SARS-CoV-2 positive or had symptoms (76.3%) and nearly all managers (90.3%) reported that some aides were required to quarantine, thus removing them temporarily from the workforce. More than half (56.5%) of the respondents reported that aides employed by their agency also worked in nursing homes or assisted living facilities.
COVID-19 Exposure and Illness in Home Health and Home Care Clients a and Aides, Massachusetts USA, March to June, 2020.
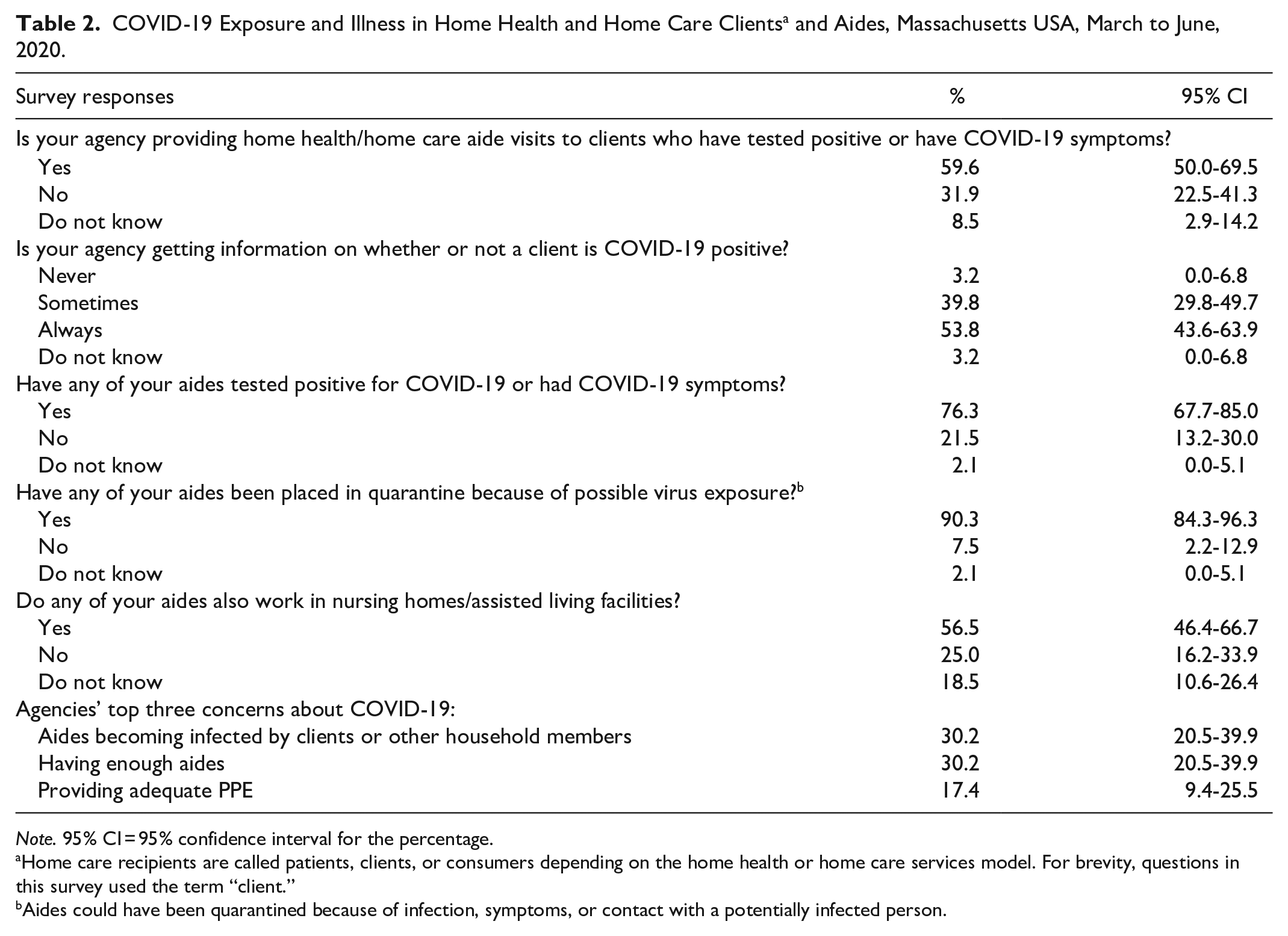
Note. 95% CI = 95% confidence interval for the percentage.
Home care recipients are called patients, clients, or consumers depending on the home health or home care services model. For brevity, questions in this survey used the term “client.”
Aides could have been quarantined because of infection, symptoms, or contact with a potentially infected person.
Home health and home care agencies needed access to the full complement of healthcare personnel PPE (Table 3). The great majority of agencies (85.4%) had policies in place requiring use of N95 respirators by aides who provided direct care to clients with COVID-19. Approximately a third (31.3%) of agencies reported they were not currently able to purchase N95 respirators. In addition to difficulty procuring PPE, barriers to infection prevention included inadequate training on fit-testing N95 respirators (23.7%), lack of client-provided cleaning and disinfection supplies (65.4%); difficulty applying infection control protocols in the highly variable home work environment (59.3%); and staff difficulty interpreting rapidly evolving COVID-19 guidance on safe practices (52.1%).
COVID-19 Infection Prevention Challenges of Home Health and Home care Agencies, Massachusetts USA, March to June, 2020.
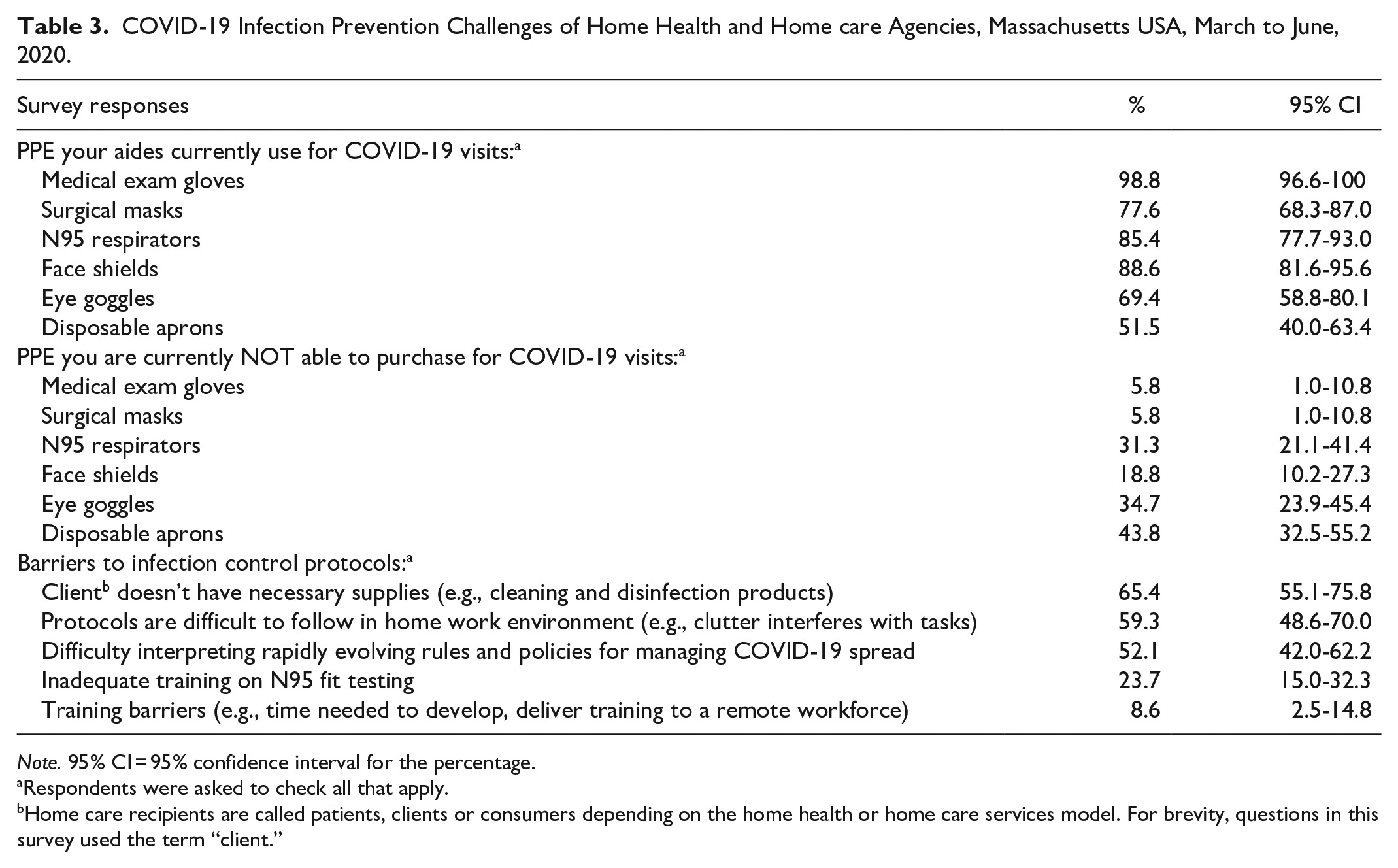
Note. 95% CI = 95% confidence interval for the percentage.
Respondents were asked to check all that apply.
Home care recipients are called patients, clients or consumers depending on the home health or home care services model. For brevity, questions in this survey used the term “client.”
Discussion
Both HH&HC clients and aides are populations vulnerable to COVID-19 infection. The pandemic imposed substantial new infection prevention responsibilities on agencies, clients, and aides. Pre-pandemic, only medical exam gloves were typically used during home visits. 5 However, as the pandemic began, agencies provided care to clients with COVID-19 and needed to develop more extensive infection prevention procedures and quickly procure a range of healthcare PPE, including N95 respirators. Despite the COVID-19 patient care provided by HH&HC agencies, early pandemic healthcare guidance, PPE, and educational and training resources were focused mainly on hospitals and nursing homes.2-4 As a result, HH&HC managers spent time adapting guidance issued for facility-based healthcare to home-based care settings. For example, because aides’ work remotely in private homes, procedures for storing/donning/doffing/disposing PPE differ from hospitals. When the pandemic occurred, instructional videos, webinars, and written guidance related to respiratory protection and other PPE were developed by government and research agencies for hospital and nursing home personnel but often did not include home health nurses and aides. The omission of HH&HC from pandemic guidance and resources reflects a more general invisibility2,3,6 of the industry and its workforce within the medical establishment, even though home healthcare is one of the fastest growing industries 7 and HH&HC aides are among the fastest growing jobs in the USA. 8
Agency employers were concerned about protecting their workforce, especially because the agencies did not always get information about whether a client had COVID-19 or symptoms and because there is already a national shortage of aides 9 and high aide job turnover. 10 Due in part to low wages and inconsistent working hours, aides often need to work more than one job 11 ; in this study more than half of the agencies employed aides who also worked in nursing homes. It was reported that aides too were concerned about being infected at work. Additionally, aides are vulnerable to community SARS-CoV-2 exposure due to their experience of social and economic inequities that present infection risks, such as housing where distancing is impossible.2,4
The findings in this survey are consistent with several recent studies.4,12,13 A case series study also documented COVID-19 illness among clients in home care. 12 A qualitative study of home care worker experiences in New York City 4 and a national survey 13 also found similar challenges for HH&HC agencies responding to the pandemic including aides providing direct care for COVID-19 positive patients, a reduction in client visit requests related to fear of infection from aides, and HH&HC managers experiencing difficulty procuring PPE.
A limitation of this study is that the analyses were based on responses from 94 agencies, however these represented all types of HH&HC programs that provided services to nearly 47,000 clients and employed more than 14,000 aides. Additionally, only Massachusetts agencies were surveyed and conditions in other states may differ.
Conclusion
In the early phase of the pandemic, HH&HC agency managers experienced new, substantial challenges in order to maintain services while keeping clients and aides safe from COVID-19. Specific needs to improve future pandemic resilience include more complete information on the infection status of clients; ready access to affordable PPE; and guidance, tools, and training from government and research agencies that are tailored for the industry and its workforce. The impacts of COVID-19 found in this study highlight the need to incorporate HH&HC more fully into future healthcare and public health pandemic planning.
Footnotes
Acknowledgements
Appreciation is extended to the HH&HC agency managers, industry associations, and government stakeholders for assisting with distribution of the survey to their members.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sama, Quinn, Galligan, Karlsson, Gore, Kriebel, Markkanen, and Lindberg received salary from grant number R01OH008229 from the National Institute for Occupational Safety and Health (NIOSH)/Centers for Disease Control and Prevention (CDC). NIOSH had no role in study design, collection, analysis and interpretation of data, writing the report, or the decision to submit the report for publication.
Prentice, Osei-Poku, and Carter declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the Betsy Lehman Center for Patient Safety and by grant number R01OH008229, from the National Institute for Occupational Safety and Health/Centers for Disease Control and Prevention. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Centers for Disease Control and Prevention.