
Abstract
Background:
This study advances health disparities research by documenting the racial/ethnic disparities in children’s health insurance coverage and health insurance adequacy under the implementation and revisions of the Affordable Care Act between 2016 and 2018 in America.
Design and methods:
Combining the nation-wide repeated cross-sectional data from 2016 to 2018 Children’s Health National Survey (NSCH), we examined the changes and trends of health insurance coverage and health insurance adequacy among children age 0–17 across different racial/ethnic groups from 2016 to 2018. Multivariate logistic regression models stratified by race-ethnicity were further analyzed to examine the association between children’s health insurance adequacy, their health insurance coverage, and their socio-demographic background factors.
Results:
Our analyses indicate that generally children’s enrollment in Medicaid or other government aided health care programs had been increasing whereas children’s enrollment in the employer-based had been decreasing from 2016 to 2018. At the same time, the number of children who said that they always had adequate health insurance to meet their health care needs has slightly dropped from 2016 to 2018, except for AIAN children. Our analyses further revealed that the risk of inadequate health insurance appears to be stronger for children in disadvantaged situation, socially and economically.
Conclusions:
The ACA has contributed to expanding childhood health insurance coverage. But racial/ethnic disparities continue to exist in children’s health insurance coverage and health insurance adequacy. To achieve equity in childhood health care, more outreach and appropriate programs are needed for children who are socially and economically disadvantaged.
Introduction
The Affordable Care Act (ACA) has been implemented as a national policy in the U.S. since 2014 to improve population health and health care quality. Committed to expanding the health care insurance coverage, shifting the focus of health care delivery from treatment to prevention, and reducing the costs for health care,1–3 the ACA also offers the promise of promoting equity in health outcomes and health care access. 1
The ACA has initiated several mandates to execute its mission such as the implementing of different types of marketplaces for people to purchase health insurance. 3 The uninsured rates in the U.S. have significantly declined following the implementation of the ACA.4,5 An analysis of data from the National Health Interview Survey has evidenced that the uninsured rates among adults age 18–64 in the U.S. have dropped from 18.9% in 2014 to 12.8% in 2015. 5 Some other studies tracking the changes in health care insurance coverage and health care access with nation-wide data have also vindicated the rapid increase in health care insurance rates among the adult population in the U.S. under the ACA.3,6–8
The contribution of the ACA in deducing the disparities in health insurance coverage for adults in different social groups has been documented.1,5,9 The ACA has called for the Medicaid expansion to include all poor and near-poor Americans under age 65, which brings benefits disproportionally to individuals living in or near poverty. 10 For example, the absolute health insurance coverage gap between people in households with annual incomes below $25,000 and people in households with annual incomes above $75,000 has narrowed down significantly from 31% in 2011 to 17% in 2015. 3 And the uninsured rates among adults age 18–64 living in poverty or near poverty have dropped from 40.0% in 2013 to 26.2% in 2015. 5
Racial/ethnic disparities in health care, featured with the persistent challenges and disadvantages for minority people to access health insurance and health care, has been a long-standing feature of the U.S. health care system and a prevailing priority for policymakers. 11 As of 2010, nonelderly Hispanics, American Indians, and Alaska Natives (AIAN) had the highest uninsured rates, with nearly one in three lacking health care insurance. 4 The ACA has expanded the Medicaid coverage and made new health insurance options available to uninsured individuals in low- and middle-income households, which has led to large gains in health insurance across all racial/ethnic groups since 2014, particularly for minority people.1,10 For instance, the uninsured rates for Hispanic people dropped from 32.6% in 2010 to 19.1% in 2016. 4
Some flaws of the ACA have been discussed. The ACA holds individuals to be responsible for any bills that are not covered by the insurance, which have been heavily criticized. 12 In addition, the ACA requires that individuals should obtain for-profit insurance coverage to purchase goods and services from for-profit pharmaceutical companies, hospitals, and doctors’ office, 10 which has also been reproached for its potentially adverse impact with the rising cost of the premium and the limited choices of pricey plans. 9 Numerous bills to alter the ACA have been proposed or even have been filed to repeal and replace the ACA since its implementation.9,12,13 The Trump administration had issued several executive orders to drumbeat the ACA during its tenure.14,15 All these have impaired the stability and implementation of the ACA initiatives and consequently the healthcare adequacy, directly or indirectly.
The ACA’s health insurance outreach and enrollment efforts are primarily targeted at adults rather than children. But the spillover effects from the reforms initiated by the ACA will ultimately compromise the health care of children in an unanticipated way, creating both promises and challenges for children’s health care.16,17
Children’s health care has largely been a successful story in the U.S, with the health coverage from Children’s Health insurance Program (CHIP) since 1997 and aids from several other public programs.18,19 But significant racial/ethnic disparities in children’s health care access have long been acknowledged, with minority children being more likely to be uninsured and to experience inadequate health care access and services.20–22 And certain disparities in childhood health care are particularly marked for specific racial/ethnic groups. For example, Hispanic children and Native American children always have higher uninsured rates. African American children and Native American children are more likely to have inadequate health insurance to meet their medical needs. 20 African American children and Hispanic children are more likely to lack consistent health insurance coverage.19,23
The implementation of the ACA, together with the other initiatives and revisions under the ACA, may result in “welcome mat” effect for children’s health insurance coverage and their health care access.16,18 The ACA’s mandate to expand insurance to more parents and extend the insurance coverage of young adults on their parent’s policies to age 26, have been acclaimed for is contribution in improving children’s health care access.24–26 At the same time, the ACA and the relevant reforms also gives rise to new challenges and some potential perils for children’s health care. For example, any modest changes in family income could result in switching to different health plans under the ACA, which may make it hard to maintain the continuity of care for many families.17,18 Further, the existence of different benefit standards and eligibility requirements casts new complexity of eligibility under the ACA, which would finally leave some children in the lurch with no affordable care options.14,17
Inadequate attention, however, has been paid to examine the trends of children’s health insurance coverage and adequacy, given the changes in health care system under the ACA. In particular, the temporal progress in narrowing the racial/ethnic disparities in childhood health insurance over the years. Further, health insurance coverage is often necessary to access health services, but it might be insufficient to meet the health care needs. 19 Whether expanding the health insurance coverage under the ACA has also ameliorated the health insurance adequacy to meet the health care needs of children from different racial/ethnic groups has also been under-examined in current literature.
Aiming to evaluate the wins and losses of children’s health insurance under the ACA, the present study will identify the temporal trends in racial/ethnic disparities of children’s health insurance coverage and children’s health insurance adequacy between 2016 and 2018. It will stretch out the current literature in health care policy by empirically documenting the trends and patterns of children’s health insurance coverage and health insurance adequacy over this time, using the empirical data from 2016 to 2018 National Survey of Children’s Health (NSCH). The findings from this study are likely to be of great interest to researchers, health practitioners, public policy makers, and public health program initiators.
Design and methods
Data and sample
This study optimized the repeated cross-sectional data from the 2016 to 2018 National Survey of Children’s Health (NSCH). The NSCH survey was designed to comprehensively assess multiple aspects of children’s health and health care, and their social and family contexts among a nationally representative sample of American children age 0–17. The NSCH survey was first started in 2003 and was consequently conducted with telephone survey every 3 years in 2007, and 2011/2012, respectively. Since 2016, a revised version of the NSCH was conducted as a mail and web-based survey on a yearly basis. Further information of the NSCH survey and data is available at www.childhealthdata.org.
For this study, the NSCH data from 2016 to 2018 were combined to examine the changes in the key health insurance aspects among children over these 3 years. Because some survey questions’ wording was inconsistent over these survey years and there are some revisions of the variable names, so only items that were the same in the data sets from surveys in these 3 years were included in the combined data set. The sample of the 2016–2018 combined data set is 10,342 children age 0–17, recruited from 50 states and District of Columbia. The combined data set included the adjusted weights to account for combining 3 years data from 2016 to 2018. The estimates from the combined dataset can be used to apply to the average annual or midpoint across 2016–2018.
Variables and measures
Child’s health insurance enrollment
This variable measured whether the selected child was currently insured or not while being interviewed (1 = yes, 0 = no).
Child’s health insurance coverage
The NSCH survey asked about children’s current health insurance coverage and provided a list of possible sources: insurance through employers; Medicaid or other government Aid program; Tricare or other. Three binary variables were used for the child’s health care insurance type (“insurance through employer,” “Medicaid or government aid program,” “Tricare or other”), with a score of “1” being assigned to those who were enrolled in the designated type of the health care insurance and a score of “0” to those who were not.
Child’s health insurance adequacy
It was tapped by asking how often the selected child’s health insurance had met his/her health needs, with dichotomous categories of “1 = always or usually adequate,” and “0 = sometimes or never.”
Child’s health status and sociodemographic controls
This study controlled for children’s health status, and their sociodemographic characteristics, including race/ethnicity, nativity, sex, and age. The responding parent was asked to rate the selected child’s health on a scale from “excellent” “very good” “good” “fair” to “poor.” The five-category response was recoded into three categories of “excellent or very good” “good,” and “fair or poor.” We further constructed dummy variables for child’s health status.
Child’s race/ethnicity in NSCH 2016–2018 datasets included the following seven categories: white alone; black alone; American Indian or Alaska Native; Asian alone; Native Hawaii or other Pacific Islander; other race alone; two or more races. This study recoded the selected child’s race/ethnicity into the five categories of “white,” “black,” “American Indian or Alaska Native (AIAN),” “Asian American & Pacific Islanders (AAPI),” and “other-race.” The “other-race” category included “some other races” and “two or more races.” Child’s nativity (1 = born in the U.S.) and child’s sex (1 = male) were dummy variables. Age was measured as a continuous variable with the specific number of years of age.
Household SES controls
We controlled for children’s household SES characteristics, including the primary household language, parent’s highest education level, and family poverty ratio. Primary household language was a dichotomous variable (1 = English). Parent’s highest education level tapped the highest level of education parents have completed, with three categories: “less than high school,” “high school graduates,” and “some college or more.”
Family Poverty Ratio reflected the ratio of total family income to the family poverty threshold. It was ranged from “50%” to “400% or more,” with higher percentages representing higher socioeconomic status. FPR of “50%” indicates that the selected child’s family was “at or below 50% of poverty level,” while “400%” indicates that the selected child’s family was “at or below 400% of poverty level.”
In addition, we constructed dummy variables for “year of investigation” (2016 as the reference category) to capture any significant changes from 2016 to 2018.
Analytic strategy
The merged NSCH 2016-2017-2018 data were analyzed by descriptive statistics and multivariate regression. First, the 3-year temporal patterns in children’s health insurance enrollment, health insurance coverage, and adequacy of their health insurance program from 2016 to 2018 were graphically presented, with a focus on differences across different racial/ethnic groups and different survey years.
Frequency distribution of all variables used in this study for each racial/ethnic group were then examined to assess the distribution and changes in the key aspects related to children’s health insurance. In addition, logistic regression models stratified by race/ethnicity were analyzed, with the adequacy of children’s health insurance being regressed on the included covariates, to examine the linkage between children’s health insurance adequacy and the included controls for demographic characteristics, and household characteristics. The dummy variables of year of investigation were also included in the regression analyses to capture the significant changes from 2016 to 2018 under the implementation of the ACA.
Results
Descriptive statistics
First, racial/ethnic disparities in children’s health insurance enrollment, health insurance coverage, and health insurance adequacy from 2016 to 2018 are visually summarized in Figures 1 to 3, with the weighted percentages of children for each value of these three variables being presented by children’s race/ethnicity and survey year.

Percentage of children uninsured by race/ethnicity, 2016–2018 (NSCH 2016–2018, N = 102,341).

Percentage of children with adequate insurance by race/ethnicity, 2016–2018 (NSCH 2016–2018, N = 102,341).
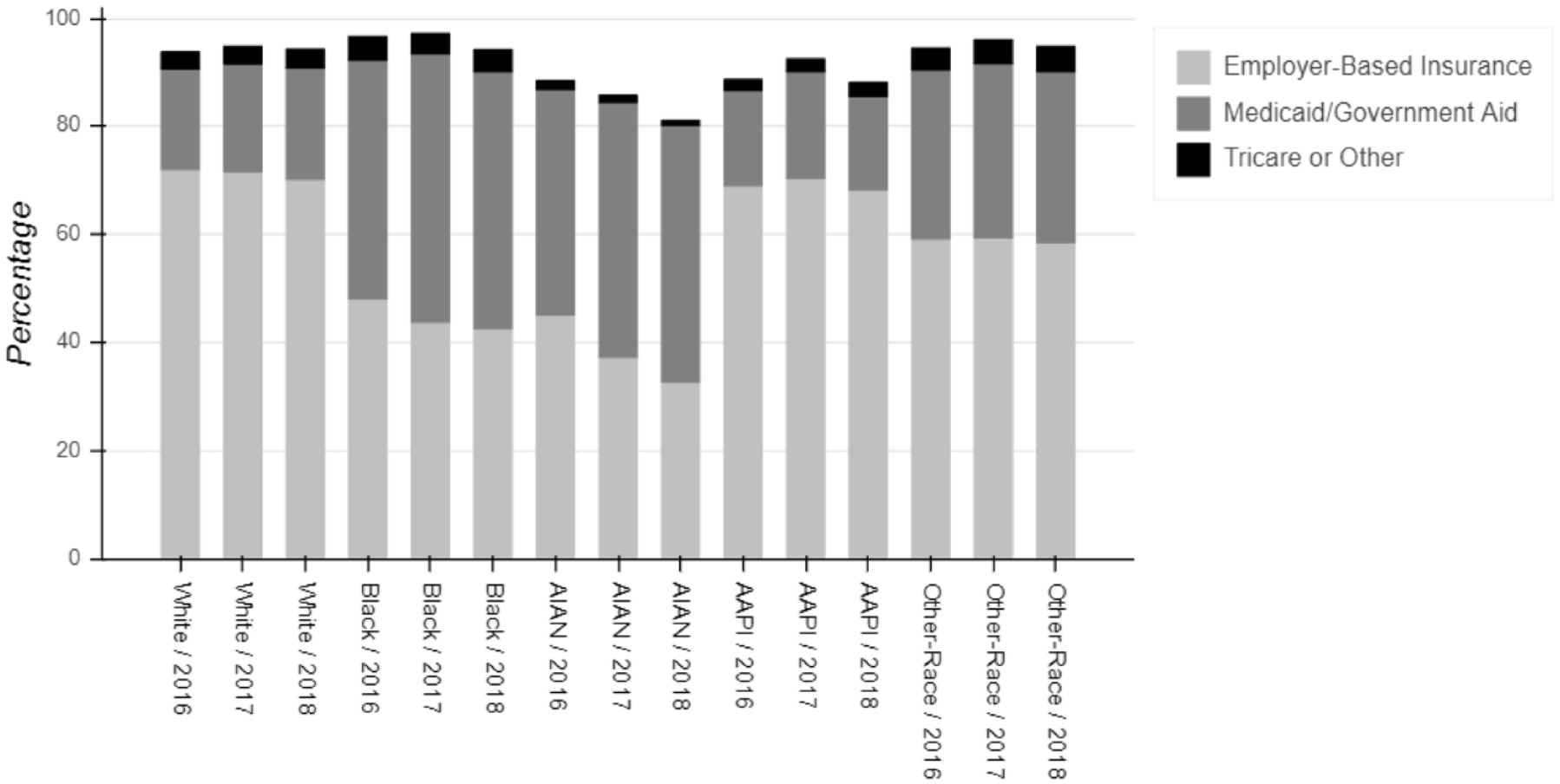
Percentage of children’s health insurance coverage by race/ethnicity, 2016–2018 (NSCH 2016–2018, N = 102,341).
Figure 1 depicts the weighted percentages of children who were uninsured in each race/ethnicity group and survey year. It shows that generally there were a minor decreasing trend and mild fluctuations in health insurance enrollment from 2016 to 2018 among children. The number of children enrolled in health insurance programs slightly decreased year by year between 2016 and 2018 for white, black, and children in other-race groups. Only AIAN and AAPI children reported a marginal increase in health insurance enrollment from 2016 to 2017, which dropped gently again in 2018. Overall, children’s enrollment in Medicaid or other government aided health care programs had been increasing whereas children’s enrollment in the employer-based health insurance had been decreasing over 2016–2018. At the same time, there had also been a minor decreasing of children who said that they always had adequate health insurance to meet their health care needs over this time.
Figures 2 and 3 presents the weighted percentage of children who reported adequacy health insurance by race/ethnicity and survey year and the weighted percentage of children enrolled in different health insurance coverage by race/ethnicity and survey year, respectively. Figures 2 and 3 further illustrate the racial/ethnic disparities in health insurance enrollment and health insurance adequacy, with minority children being in a more disadvantaged position/having been faced more challenges. For example, the uninsured rates increased from 3.1 in 2016 to 4.0 in 2018 for white children, whereas it increased from 5.6 in 2016 to 7.0 in 2018 for black children and 12.8 in 2016 to 15.1 in 2018 for American native or Alaska native (AIAN) children. In 2016, 48.2% of black children were enrolled in employer-based health care insurance but this number dropped to 42.7% in 2018. The same pattern was even obvious for AIAN children with a drop at almost 13% (45.2% in 2016 and 32.8% in 2018, respectively). A minor decreasing of children who reported “always have adequate health insurance” from 2016 to 2018 has also been observed for white children (90.1% vs 89.8%), and black children (88.3% vs 86.9%). However, a marginal increasing of health insurance adequacy was observed for AIAN children from 2016 (83.7%) to 2018 (84.6%) (tabular data for Figures 1–3 available upon request).
Weighted descriptive statistics for all variables included in the study are summarized in Table 1. The results are reported by race/ethnicity to illustrate the disparities between white and other four non-white racial/ethnic groups. According to Table 1, most children (89.9%) agree that their health insurance was adequate to meet their health care needs. But there were significant differences across different racial/ethnic groups. For example, the percentage of children who acknowledged their health insurance adequacy for white, black, AIAN, AAPI, and other-race children was 93.5%, 87.7%, 84.3%, 88.7%, and 88.5%, respectively.
Means (standard deviations) and proportions of dependent and independent variables by race/ethnicity (NSCH 2016–2018, N = 102,341).
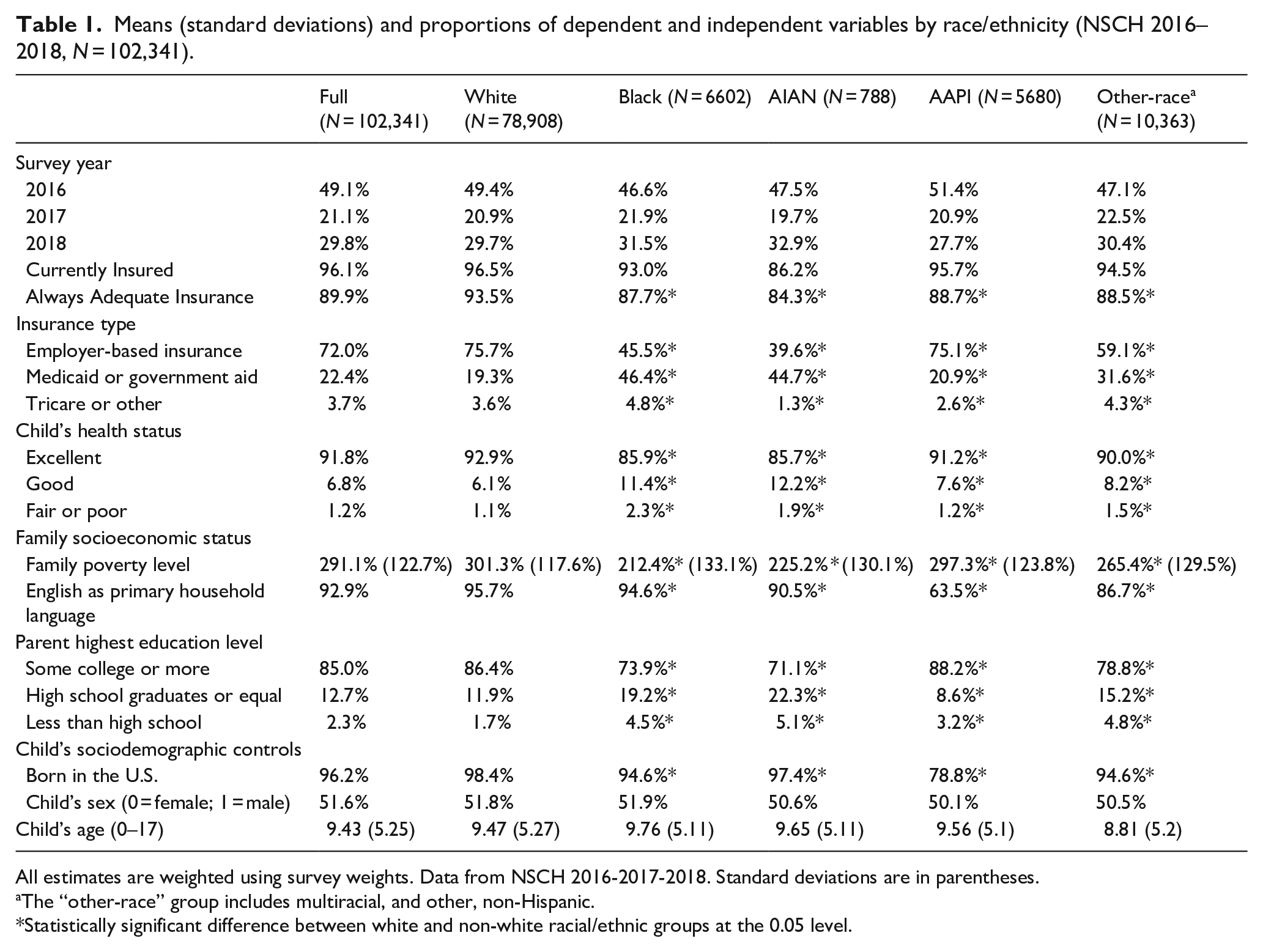
All estimates are weighted using survey weights. Data from NSCH 2016-2017-2018. Standard deviations are in parentheses.
The “other-race” group includes multiracial, and other, non-Hispanic.
Statistically significant difference between white and non-white racial/ethnic groups at the 0.05 level.
There were also significant racial/ethnic differences in children’s enrolled health insurance programs. White children (75.7%) and AAPI (75.1%) children were more likely to be covered by employer-based insurance, in comparison to their counterparts from black (45.5%), AIAN (39.6%), and other-race group (59.1%). More black children (46.4%) and AIAN children (44.7%) were enrolled in public health care insurance programs such as Medicaid or other government-aided programs. Table 1 also indicates significant racial/ethnic disparities in children’s health status. Black and AIAN children reported poorer health status than white children. For example, 92.9% of white children rated their health as “excellent,” compared to 85.9% of black children and 85.7% of AIAN children. More black children (2.3%) and AIAN children (1.9%) rated their health as “Fair or Poor,” compared to white children (1.1%). With respect to children’s nativity, more AAPI children and children from other-race group were foreign born. AAPI children and children from other-race group were comparatively younger than whites, black, and AIAN children.
Children’s household socioeconomic status also varied across race/ethnicity. Black children and AIAN children were more likely to being living in households with lower parental educational level and lower household economic status. For example, less black children (73.9%) and AIAN children (71.1%) have a parent with the highest educational level of at least some college, compared to white (86.4%) and AAPI (88.2%). In addition, white children were more likely to live in economically vital and stable households than other racial/ethnic groups. The average family poverty level for white children was 301.3%, in comparison to 212.4% and 225.2% for black and AIAN, respectively. Living in a household with English as the primary household language was least common for AAPI (63.5%), relative to white (95.7%), black (94.6%), and AIAN (90.5%).
Results from logistic regression analysis
Logistic regression models stratified by race/ethnicity were estimated to examine the association between children’s health insurance adequacy and their health insurance type, as well as the included socio-demographic controls. Table 2 reports the odds ratios and standard errors of having adequate health insurance among children in each racial/ethnic group.
Logistic regression results predicting odds of having adequate health insurance (NSCH 2016–2018, N = 102,341).

All estimates are weighted using survey weights. Data from NSCH 2016–2018.
OR = odds ratio. Standard errors are in parentheses.
The “other-race” group includes multiracial, and other, non-Hispanic.
p < 0.05. **p < 0.01. ***p < 0.001.
The results from Table 2 indicate that only AIAN children reported a significant change in health insurance adequacy over these 3 years. The odds of reporting adequate health insurance for AIAN children in 2018 were almost two times as likely as they were in 2016 (OR = 1.98, p < 0.05). But no statistically significant change had been observed for white, black, AAPI, and other-race group over this time.
The results from Table 2 further illustrate the importance of public health insurance programs such as Medicaid and other government aids, which is significantly associated with the adequacy of health insurance among children across all different racial/ethnic groups examined in this study. Employer-based health care insurance was significantly associated with the adequacy of health insurance for white children (OR = 3.06, p < 0.001), AAPI (OR = 1.66, p < 0.01), and children in other-race group (OR = 1.093, p < 0.001). But not for black and AIAN children. Tricare or other similar type insurance was only significant for white children (OR = 5.04, p < 0.001), and children from other-race group (OR = 2.73, p < 0.001), but not for black, AIAN, and AAPI children.
Child’s household socioeconomic status was included as a covariate. The statistical results indicate that there was a significant relationship between children’s health care insurance adequacy and their family poverty level, which was consistent for all different racial/ethnic groups. Parental education, however, was significantly associated with the health insurance adequacy only for AIAN children and AAPI children. For example, compared to children whose parents only had less than high school education, the probability of having adequate health care insurance for AIAN and AAPI children whose parents had some college level education or more would be approximately 86% and 61%, respectively. Speaking English as the primary household language was significantly associated with the adequacy of health care insurance for white (OR = 1.24, p < 0.01), AIAN (OR = 1.35, p < 0.01), and AAPI (OR = 1.43, p < 0.01).
The impacts from child’s sociodemographic background were also controlled in this study. The results indicate that nativity was important for white, black, and AAPI children. The possibility of having adequate health insurance for native-born white children was 22% higher than those who were foreign-born (p < 0.01). For native-born AAPI children, the possibility of having adequate health insurance was as high as 62% compared to their foreign-born peers. Black boys were more likely to have adequate health care insurance (OR = 1.27, p < 0.05) than their female counterparts. There was a weak but significant association between age and health insurance adequacy for black children (OR = 1.03, p < 0.05). For black children, the older they get, the more likely their health care insurance will meet their health care needs. However, the effect from age worked in the opposite direction for white children and children from Other-race group. White children and children from other-race group were less likely to report an adequate health insurance as they were getting older.
In addition, children’s general health status was significantly related to their health insurance adequacy. Compared to those children who reported “excellent” health, those who reported “good” or “fair/poor” health status generally were less likely to report adequate health insurance, which was consistent for all children regardless of race and ethnicity. For instance, the probability of reporting adequate health care insurance for white children who reported “good” health would be reduced by approximately 55% than their counterparts who reported “excellent” health. For blacks, AIANs, and AAPIs who report “good” health, the probability of reporting not having adequate health care insurance will be reduced by 57%, 61%, 49%, 50%, respectively. If they reported “fair or poor” health, the probability for them to report adequate health insurance would be even lower.
Discussion
We examined the trends in children’s health insurance enrollment and the adequacy of their health insurance between 2016 and 2018 under the ACA and the relevant initiatives procreated from it. Consistent with the existing study, 24 our study demonstrates that the ACA’s mandatory expansion of Medicaid represents a success story of promoting health care access, as reflected in the increasing rates of health care insurance enrollment among children. However, our study also indicates a mild fluctuation in children’s health insurance enrollment, particularly a mild decreasing since 2016–2017 for all children and the comparatively elevated risks for minority children to be uninsured. Such mild drop in this time may be explained as the evidence of the potential harms from the partisan conflicts and misaligned policies in health care reform initiatives, as argued by some scholars.2,24,26
Our study validates the racial/ethnic disparities in children’s health insurance enrollment and adequacy, which has been documented in previous research.19,24,27 Our analyses indicate that white children and AAPI children are more likely to enroll in employer-based health insurance. Black children and AIAN children are mainly covered by Medicaid and other government aided health care programs. Moreover, we find that even under the positive effect of the ACA, the significant gap between different racial/ethnic groups in children’s health care insurance enrollment and health insurance coverage remain existent. Minority children in the U.S. continue to face challenges and disadvantages in health care compared to the majority white. Even among insured children, there are disparities in health care access and health care quality. And such gaps have been increasing since 2016, which is also consistent with the arguments by other studies.19,24
In addition, we find that there were no significant improvements in children’s health insurance adequacy over the 3 years from 2016 to 2018. Proportion of children who reported the health insurance adequacy has been stagnating between 2016 and 2018. One possible reason is the changing dynamics of the health care delivery. The landscape of health care delivery in the United States had been significantly altered with the federal government taking increasing fiscal responsibility for the provision of services, as well as for regulation and even pricing of these services. 2 Such changes also impacted the process for children to get enrolled in appropriate health insurance programs to meet their health care needs. The healthcare reform efforts from the ACA have helped to fight against the inequity in health care by addressing the lack of health insurance of the uninsured groups, which are nonetheless solid steps in the direction of promoting the equity in health and health care. The real equity in health care, however, has not yet come and needs further efforts to achieve.
Our analysis further reveals that minority children continues to face challenges to get sufficient insurance to meet their health care needs, which supports the previously documented racial/ethnic disparities in suboptimal health care as well as in experiencing inadequate health care for unmet health care needs.19,28 For minority children, their enrolled health insurance program probably will not be sufficient for their health care needs. Public health insurance or government-aided programs has provided access to the health care system for the poor, but the character and quality of the services have rendered. 2 Children’s health insurance adequacy is significantly related to their family’s socio-economic status, the immigration experience of their parents and their own nativity. Children from families with lower economic status, from immigrant families and children who are foreign-born are facing elevated challenges of getting adequate health insurance. Those persons who are socio-economically disadvantaged are also medically disadvantaged when it comes to obtaining adequate insurance program and quality services. Some socio-economically disadvantaged groups may not even be aware of their eligibility for relevant health care programs or they may face challenges and barriers in enrolling in such programs due to the insufficient knowledge of the relevant programs or limited language proficiency.19,28–30 More outreaching programs targeting socially disadvantaged children who are at risk for not having adequate health insurance are needed to further consolidate the promises of the health insurance expansion from the ACA.
Limitations
Our study has several limitations. First, as previously indicated, this study analyzed data by combining cross-sectional NSCH data from surveys in 3 years. However, due to the inconsistency of some survey questions’ wording and some revisions of the variable names over these survey years, only items that are the same in all three data sets were included in the 2016-2017-2018 combined data set. Second, our study regrouped the original categories of children’s race/ethnicity and lumped children who reported “two or more races” and “some other races” rather than white, black, AIAN, and AAPI under “other-race” group, which may fail to capture the rapid changes in accessing health insurance for the rapidly growing Hispanic, which have been documented in other studies.31–33 Further, several of racial/ethnic groups in this study had small sample sizes. These all call for caution in interpreting the findings of this study.
Conclusions
This study enriches the empirical evidence to document whether the ACA and the procreated initiatives from it has really turned out that way as expected to improve the racial/ethnic equities in health care. Findings from our study indicate that obtaining affordable health insurance for the uninsured was an historic change but challenges remain for health care equity. The ACA and the relevant health reform efforts have nonetheless brought their contributions to promoting the health care equity by addressing the health insurance enrollments of socially disadvantaged groups. However, racial/ethnic disparities still persistent. Further, the increasing in health insurance enrollment has not yielded the increasing health insurance adequacy among children. Considering the stagnancy of health insurance adequacy among children in recent years even with the increasing of their health insurance enrollment, policy makers should consider extending appropriate and reliable health insurance coverage. Appropriate outreach programs are needed to help socio-economically disadvantaged groups. In addition, further research is still needed to shed light on the underlying mechanisms of underinsurance of insurance and the ongoing monitoring of disparities by health plans.
Footnotes
Author contributions
YYS coordinated the study by requesting and merging the NSCH data, writing and editing the paper, and formatting the manuscript in line with the journal requirements; CBT contributed by coordinating the selection and coding of the variables, and editing the overall paper; RKP contributed by conducting extensive literature review, and editing the literature review part and the overall paper; AM contributed by coordinating the literature review and discussing the findings from this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a faculty research fellowship from The Center for African American Public Policy at Norfolk State University (PI: Yuying Shen).
Ethics approval and consent to participate
This study is based on analysis of a publicly available secondary data. No ethical approval is required.
Significance for public health
Promoting equity in childhood health and health care has long been the national public health priority. The Affordable Care Act (ACA) has been initiated to improve population health and health care in the U.S. Using nation-wide datasets from National Survey of Children’s Health (NSCH), this study advances the public health and health disparities research by documenting the racial/ethnic disparities in children’s health insurance coverage and health insurance adequacy under the implementation and revisions of the ACA between 2016 and 2018. It indicates that the ACA has contributed to expanding childhood health insurance coverage. But the expanded health insurance coverage under the ACA may not be adequate to meet the health care needs of children. In particular, minority children are more likely to be underinsured for their health care needs. To achieve health care equity for children, more outreach programs are needed for children who are socially and economically disadvantaged.
Availability of data and materials
The data used to support the findings of this study are available from the corresponding author upon request.