
Abstract
Objectives:
The COVID-19 pandemic rapidly impacted communities, however there is limited information about the beliefs, behaviors, and trust in government responses of populations across the country. It may be especially useful to understand state-based and regional differences that people reported early in the pandemic, to inform national and regional public health policies and communication strategies. This paper reports on correlates of perceptions of state and federal policies and prevention practices in six states with varying trajectories of COVID-19 cases and deaths, during the first major wave of the pandemic.
Methods:
A cross-sectional survey of COVID-19 policies, perceptions, and behaviors in six states (three in the northeast/mid-Atlantic and three in the southeastern United States), was conducted in April 2020 using an online platform of research volunteers. The survey asked about demographics; use of and belief about the effectiveness of preventive behaviors; experience with COVID-19 testing, diagnosis, quarantine, and hospitalization; risk behaviors and perception; opinion of local, state, and federal government guidelines and information; sources of information; and scales measuring time perspective and collectivism/individualism.
Results:
Responses from 1476 adults in six states showed that the most often-practiced prevention practices involved social distancing, and that reactions to federal government policies differed regionally and by political party affiliation.
Conclusions:
These findings improve understanding of how Americans view government responses to the pandemic, and their prevention practices, early in the pandemic. These data will help to create more effective public health policies to control the pandemic and achieve public support for control measures.
Introduction
The COVID-19 pandemic rapidly impacted communities both locally and globally. Since the first case was reported in the United States in late January 2020, COVID-19 rapidly affected the media, healthcare, business, and politics. COVID-19 is unique with respect to its clinical presentation and course, its communicability, and its sociobehavioral impact, especially regarding mitigation and containment. With no single effective treatment or a vaccine on the immediate horizon during the first year of the pandemic, mitigation and containment efforts were central to efforts to control the spread of the virus. 1 Despite efforts of public health officials and the media to share timely and accurate information about COVID-19, there have been many controversies and, frequently, misinformation was disseminated.2–4 The rapid evolution of the pandemic, and of government and business responses to the crisis in its first year,5,6 underscore the importance of research to optimize disease control efforts.
Although there has been wide coverage of the pandemic and related issues in the mass media and social media, there is limited information about how various sub-populations across the US are reacting to the pandemic in terms of their behaviors, risk perceptions, and knowledge. Further, as shown in two recent studies, it is important to examine the role of political affiliation and orientation in framing responses to the pandemic.7,8 Public opinion polls found that Republicans were much more likely to consider COVID-19 “made-up” and to believe conspiracy theories.4,9 An event history analysis of early social distancing policies across 40 states found that the most important predictors of policy adoption were political in nature, with Republican governors and supporters of President Trump being slowest to adopt social distancing measures. 10 In contrast, a prospective observational study concluded that both the number of infections and deaths were powerful predictors of issuing stay-at-home orders, explaining 60%–80% of the variance in governors’ decisions. 11
Researchers, public health experts, and policymakers disagree on the best strategies for controlling the spread of COVID-19. However, little is known about individual attitudinal and behavioral responses to the pandemic. This study, grounded in concepts from the ecological model that posit multi-level influences on behavior, 12 assessed background characteristics, attitudes, and behaviors related to prevention and governmental response to the early months of the COVID-19 pandemic in six states.
The states included in this survey were three in the Northeast region – New York, New Jersey, and Pennsylvania – and three in the Southeast – Florida, Georgia, and Alabama. These states were of interest because of the stark contrast between the two regions in the early months of the pandemic: high numbers of cases and fatalities occurred in the Northeast, while fewer cases emerged in the Southeast. 6 Likewise, state and local policies for shutdowns and stay-at-home orders were earlier and more restrictive in the Northeast, and less so in the Southeast. Thus, we were interested in assessing differences in perceptions of government leaders’ reactions during the first year of the pandemic as well as differences in preventive behaviors between these regions.
A better understanding of Americans’ view of government responses to the pandemic, and their prevention practices, is vital for creating public health policy moving forward and effectively communicating important information. Analyses from this study will help to fill this gap in public health knowledge. The aims of this paper are to: (1) describe initial findings from the baseline COVID-19 Policies, Perceptions, and Behaviors Survey; and (2) report on findings about correlates of perceptions of state and federal policies and prevention practices in six states with varying trajectories of COVID-19 cases and deaths.
Methods
Survey design
The survey was developed by the authors and conducted in April 2020, about 1 month into the rapid increase in COVID-19 cases and deaths that spurred widespread stay-at-home orders and business closures in much of the world. This was the first of three surveys conducted in the same sample over a 1-year period in order to help understand policies, behaviors, and experiences at different time points during the COVID-19 pandemic, and changes over time.
Participants and sample recruitment
Participants were recruited through ResearchMatch, 13 an online registry of volunteers for medical and public health research. Any adult registered on ResearchMatch who is 18 years of age or older, could read English fluently, was capable of giving informed consent, and resided in Alabama, Florida, Georgia, New Jersey, New York, or Pennsylvania at the time of the survey was eligible for this study.
After IRB approval was received, ResearchMatch contacted potentially eligible participants via email to invite them to participate in the study. Next, ResearchMatch notified the research team with contact information for eligible volunteers who indicated their interest in participating in the survey. Eligible volunteers were then emailed by the research team a personalized link to the survey instrument. The survey was hosted on the Qualtrics platform (Qualtrics, Provo, UT) and could be completed on either a computer or a smartphone. Participants completed an informed consent form that was embedded into the survey instrument before accessing the questions.
Measures
The survey used items and measures from previous surveys, adaptations of published measures, and original items created for the COVID-19 epidemic context. 14 The instrument included 36 items about a range of topics, including: demographics; use of and belief about the effectiveness of preventive behaviors; personal or close relationship experience with COVID-19 testing, diagnosis, quarantine, and hospitalization; risk behaviors and perception; opinion of local, state, and federal government guidelines and information; sources of information; and scales measuring depression, 15 time perspective, 16 and collectivism and individualism. 17 The survey took 10–15 min to complete. Questionnaire items and constructs are provided in Supplemental Appendix A.
Statistical analysis
This analysis focuses on describing survey respondents’ background characteristics and on examining factors associated with perceptions of state and federal policies and prevention practices during the early months of the pandemic in the United States. The main outcome variables are perceptions of (1) federal government reactions to the pandemic, (2) state and local government reactions to the pandemic, and (3) the frequency of practicing 10 recommended prevention or mitigation behaviors.
Independent variables and covariates include demographic characteristics; self-rated health and comorbidities; personal and friend/relative experience with COVID testing, diagnosis, quarantine, or hospitalization; and two personality features hypothesized to be related to perceptions and behaviors of interest: long-term time perspective (how much one focuses on the present vs the future) and collectivism (the tendency to consider other people when making decisions or taking action).
After removing duplicates or respondents who had moved out of the states included in the study, descriptive statistics were computed for all variables. Composite measures were calculated for outcome variables which had high internal consistency as measured by Cronbach’s alpha (α): reactions to federal policies (three items, α = 0.81); reactions to state and local policies (two items, α = 0.78); preventive behaviors (10 items, α = 0.72). Composite measures for independent variables and covariates were also computed and showed excellent internal consistency: personal COVID experience (four items, α = 0.70); friend/relative COVID experience (four items, α = 0.81); long-term time perspective (13 items, α = 0.86); and collectivism score (six items, α = 0.84).
Bivariate analyses focused on examining differences across states to inform the multivariate models. Next, to answer the main research questions regarding correlates of perceptions of policies and prevention practices, logistic regression models were used for all three outcome variables.
Models were fit using SAS version 9.4. (SAS Institute, Cary, NC). The GENMOD procedure was used for fitting generalized linear models using logistic regression with ordinal multinomial responses for all outcome variables. There were two separate models for outcome of the federal government and state/local government reaction scores and for prevention behaviors. Independent variables in Model 1 were age, gender, race, education level, marital status, employment status, household income, and political affiliation. Model 2 included variables from Model 1 plus comorbidities, general health rating, self-reported experiences with COVID, COVID experiences with friends or relatives, and the scores for long-term perspective and collectivism. Full models are included as Supplemental Material.
Results
Response rate and description of sample
The ResearchMatch registry contacted 32,728 people in the volunteer pool who met the eligibility criteria. A total of 2115 people agreed to release their contact information to the research team and all were emailed personalized links to the survey. Of the 2115 agreeing to participate, 1566 completed the survey within 3 weeks, for a response rate of 74.0%. Thirty-eight cases were dropped due to incomplete data, 12 were duplicates, and 40 no longer resided in one of the six study states, leaving a total of 1476 participants (94.3% of the 1566 surveys received and 69.8% of all 2115 surveys sent out) for analyses. The sample includes between 117 and 566 respondents from each of the six states (Figure 1).
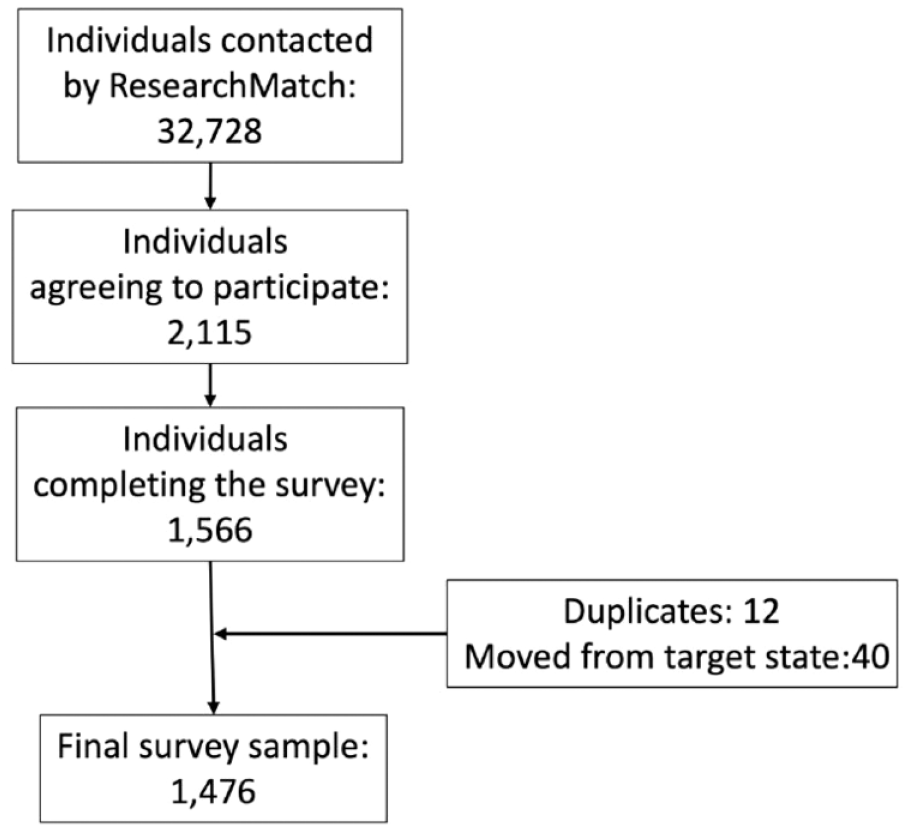
CONSORT diagram illustrating recruitment and selection of subjects participating in the survey.
Table 1 shows respondents’ background characteristics and other analytic variables by state. The average age of participants was 48.5 years SD 16.8); they were nearly 80% female and 84% non-Hispanic White. Most respondents were college graduates or higher, but 24.3% had only some college or less. About 41% reported household incomes less than $75,000, and self-identified political affiliations were predominantly Democrat (52%), with 23% Independent and 15% Republican. Respondents from Florida were significantly older and more often White and retired. Respondents from the southeastern states (Alabama, Florida, and Georgia) were more often Republican and those from the Northeast were more often Democrat or Independent.
Respondents’ background characteristics, COVID-19 experience, prevention behavior, and belief about government policies across six states (N = 1476).

Main outcome variable distribution and differences across states
On a scale of 1–7 (too limited to too extreme, respectively), mean reactions to the Federal Government Reaction to COVID were 2.7 (SD 1.4) and 3.5 (SD 1.2) to State/Local Government Reaction. Respondents from the northern states more often felt the federal government reaction was somewhat limited, and that the state/local government reaction was more strict, compared to respondents from the southern states.
The mean Prevention Behavior score, measured on a scale of 1–5 (never to always or almost always) was 3.8 (SD 0.6); the score was significantly higher in the northeastern states than in the southeastern states (Table 1). The most frequently practiced prevention behaviors at the time of the survey were avoiding social gatherings (97.3%), staying home as much as possible (93.1%), keeping a safe distance from people (90.1%), and handwashing (89.3%). The least-practiced prevention behaviors were cleaning or disinfecting surfaces and objects (61.6%), not touching face/eyes/nose (44.2%), wearing a mask (30.5%), and wearing gloves (18.1%).
Factors associated with the federal and state government reactions to COVID-19
Table 2 shows the final models examining factors associated with perceptions of the federal government reaction and state/local government reaction. With respect to federal government reaction, respondents viewed the federal government reaction as most strict, but this was not statistically significant. The most significant predictor of this outcome was political affiliation, with Republicans reporting that the federal government reaction tended to be too extreme or restrictive (means: Republican = 4.32 (SD 1.21), Democrat = 2.10 (SD 0.91), independent = 3.00 (SD 1.34)). For state and local government reactions, compared to NY, the southeastern respondents rated their governments’ reactions as significantly less extreme, as did those with poorer self-rated health, more self-reported personal experience with COVID-19, and longer-term time horizon perspectives. Men and Republicans rated their states as overly strict, even when controlling for other background characteristics.
Final logistic regression model of respondents’ demographics, self-rated health, COVID-19 experience, and personality associated with reactions to federal government and state/local government policies. (N = 1476).
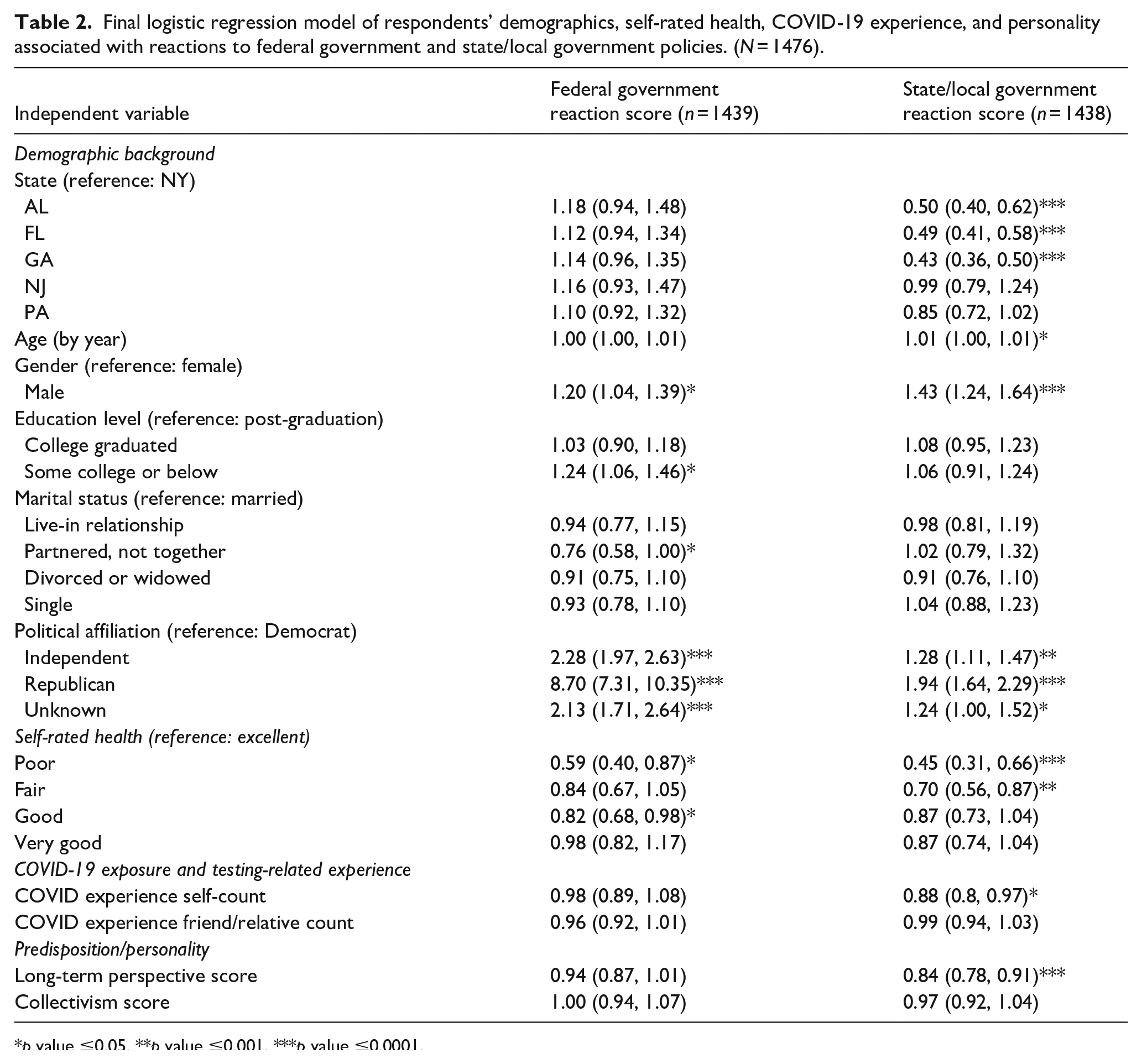
p value ≤0.05. **p value ≤0.001. ***p value ≤0.0001.
Factors associated with COVID-19 prevention behaviors
Table 3 shows the final models examining factors associated with prevention behaviors. Both Model 1 and 2 showed that respondents from Florida and Alabama and men practiced prevention less often, while Blacks more often took preventive precautions, comparing to White/Non-Hispanic White (means: Black = 3.96 (SD 0.60), Non-Hispanic White = 3.80 (SD 0.55)). In Model 2, respondents with comorbidities were less vigilant, while those with personal or friend/relative COVID experience, those with longer-term time horizon perspectives, and with a collectivist orientation more often took preventive actions.
Final logistic regression model of respondents’ demographics, self-rated health, COVID-19 experience, and personality associated with composite prevention behavior scores (N = 1476).

p value ≤0.05. **p value ≤0.001. ***p value ≤0.0001.
Model 1 includes age, gender, race, education level, marital status, employment status, household income, and political affiliation.
Model 2 includes variables from Model 1 and plus comorbidity, general health rate, COVID experience self-count, COVID experience friend/relative count, long-term perspective score, and collectivism score.
Discussion
We surveyed 1476 individuals in six states, three in the Northeast and three in the Southeast, respectively. This was the first such study to investigate geographic differences within the US in terms of policy and prevention related to COVID-19. Our goal was to elucidate respondents’ perceptions of state and federal policies and patterns of prevention-related behaviors as they relate to mitigation and containment of the COVID-19 pandemic. In comparing the two regions, we found that there were modest demographic differences in age, race, marital status, income, and employment; there was no difference with regard to gender. At the state level, these differences were more pronounced, and political affiliation was significantly different across the states, as shown in Table 1. Even though the distribution of political affiliation was unbalanced, with only 15% of respondents identifying as Republican, it is useful to consider political polarization in addition to geographic location with respect to the two main foci of this study: public health policy and prevention.
Reactions to policy
In our study, respondents’ reactions to federal government policies differed regionally and by party affiliation. Those in the southern states as well as Republicans overall reported that these policies were more restrictive than did northern respondents and Democrats. In addition, respondents from the northern states felt that the federal government response was not as restrictive or extreme as those from the southern states. In terms of state or local government reaction to the pandemic, respondents from the southern states felt that the policies were not as extreme or restrictive, compared to those from the northern states. However, there was a gender and party affiliation polarity in this construct, with men and Republicans reporting that the response from state or local governments was “extreme.” This finding aligns with a study on political polarization that demonstrated that Democrats are more likely to accept policy from experts than Republicans, who would rather hear messages that suggest, rather than mandate, preventive actions to be taken during the pandemic. 18
Successful policy response to a pandemic requires widespread acceptance of accurate and credible information. Scientific fraud and conspiracy theories fuel lack of belief in science, and “expert advice” is often seen as driven by opinions and attitudes rather than fact; public skepticism is widespread. 3 A report 9 from the Pew Research Center suggests that skepticism about the pandemic’s origins and the way it is being addressed is rooted in the polarity of individual’s reliance on information sources, specifically that those relying on the White House for information are most likely to view the pandemic and policies addressing it with skepticism. In addition, Republican governors and governors of states with a preponderance of supporters of President Trump enacted control and prevention policies more slowly than those at the other end of the political spectrum. 10 However, regardless of political affiliation, leaders have responded with control policies as the number of cases increased 11 in a dose-response pattern. Our findings suggest that the dominant political affiliation of the geographic area is vital to consider when designing messaging to gain more widespread support for policies aimed at mitigating the spread of the virus.
Prevention attitudes and behaviors
Prevention behaviors were markedly different between southern and northern states, with the latter practicing more behaviors that are known to reduce the spread of SARS-CoV-2. Chief among the prevention behaviors reported by respondents in the Northeast were social distancing, whether by avoiding social gatherings, staying home, or keeping a physical distance from others. This finding comports with that of a recent national study that found a significant association between party affiliation and social distancing. 19 Our multivariate models showed that prevention behaviors were less commonly practiced by men in general and by respondents from two southern states (AL and FL). Blacks and those with experience with COVID, either directly or through a relative or friend, were more likely to engage in preventive behaviors. In contrast to another study, 20 we found that age, adjusted for the covariates in either Model 1 or 2, was not associated with preventive behavior. In another study, it was found that those who believed they could prevent the spread of SARS-CoV-2 were more likely to engage in social distancing, while those who believed that social distancing was difficult, or were working in environments where distancing was difficult, were less likely to distance. 21 As of early July 2020, after this survey was completed, 86% said they had worn a mask when outside their home, but with party affiliation polarity: more Democrats (98%) than Republicans (66%) work a mask outside. 5
There are several limitations to our study. First, the survey was administered to subjects identified through an established research subject registry 13 that relies on volunteers to sign up for possible participation in a wide range of health-related research projects. While this resource is a valuable tool for researchers who seek to draw a sample of subjects from across the United States or within a geographic region, as we did, these volunteers may not be representative of the region where they live. In addition, those in the registry who do agree to participate in the study might not be representative of the complete pool of volunteers. In addition, our study used a convenience sample, which further limits the generalizability of the results. However, given these caveats, we feel that the sample was representative of the ResearchMatch participants in the states we investigated. In particular, ResearchMatch does not suffer from the problems that some other subject registries and anonymous surveys encounter, such as duplicate subjects or responses, or imposter subjects.
Another limitation is that the survey is cross-sectional, and cannot reflect or assess the rapidly changing landscape of policy and prevention behaviors, nor can any causal inference be established. We recognize that even over the observation period of this study, policies about social distancing, mask-wearing, and other mitigation procedures were quickly adopted, changed, or even abandoned. We did not analyze time-specific state policy data that could be coupled with subject responses to ascertain the granular effects of policies on perceptions and preventive behavior.
In addition, subjects were required to access the survey online, and thus needed access to a computer. It is possible that even though they had registered on ResearchMatch, perhaps using a computer in their office or other location than home, they might not have access to a computer at the time of the survey, given that many throughout the US were staying at home. This may have introduced additional response bias. There is the possibility of social desirability bias as well, especially regarding preventive behaviors. Perceptions or experience with avoiding close contact when walking, or other anti-social behaviors, could bias responses in favor of false positives, where respondents could say they kept socially distant frequently when in fact they seldom did.
Finally, the pandemic is now over 2 years old, and one could argue that the observations made here are outdated and of little value to public health practitioners and researchers. We contend that this study offers valuable information for the public health community as they prepare for the next pandemic, or even the next surge of COVID-19 cases. Specifically, this information could help public health workers as they craft messaging and policies, and enact procedures to mitigate the spread of disease in advance of an outbreak. As such, this study could add meaningfully to the development of a toolkit that was unfortunately not in evidence in the earliest phases of the COVID-19 pandemic.
Conclusion and recommendations
Although our findings indicate that there are significant regional differences with regard to perception of public policy and of preventive behaviors, our study raises as many questions as it answers. For example, we do not know what the temporal effects of policy change are on preventive behavior adoption and practice, and once adopted, we do not know how long preventive behaviors persist. Understanding these relationships is critically important to designing and implementing strategies to protect the public’s health, for this and future pandemics. Strategies to increase the adoption of preventive behaviors, including message framing and repetition, description of behaviors, and alignment of behavior with existing habits have been proposed as useful in the fight against COVID-19. 22 However, many of these are classic public health strategies, and it is important to consider additional strategies that are mandated by the special and fast-moving circumstances associated with a pandemic like COVID-19. More research is needed in this regard, and among others, one research question that needs to be answered is the impact, in the near and long term, of policies on preventive behaviors, adjusted for perceptions of policy and of the pandemic itself. Given the ability to identify and catalog policy data at the state, county, or municipal level there is an important and potentially fruitful line of investigation that should be pursued in the future by way a series of natural experiments. The COVID-19 pandemic marked a major uptick in the importance of state policies for the public’s health. 23 It would be interesting to see how these behaviors and attitudes change, or not, in response to the stimulus of a policy change. Other important questions include the effects of isolation, loss of employment, loss of social support and capital, and of information obtained from social and broadcast media on the perception of policies. While beyond the scope of the study reported here and are just now being investigated by others,4,24 we suggest that these questions are important and potentially fruitful avenues for research as we progress through the pandemic and beyond.
Supplemental Material
sj-pdf-1-phj-10.1177_22799036221102178 – Supplemental material for Correlates of attitudes toward COVID-19-related public health policies and prevention practices in six states
Supplemental material, sj-pdf-1-phj-10.1177_22799036221102178 for Correlates of attitudes toward COVID-19-related public health policies and prevention practices in six states by Karen Glanz, Jade Avelis, Pui L Kwong and John H Holmes in Journal of Public Health Research
Footnotes
Acknowledgements
We are grateful for the assistance of Samantha Marks and Claudia Caponi.
Author contributions
The authors contributed equally to the research and the preparation of this manuscript. Contributions included conceptualization and design of the study and this manuscript, drafting and revision of the manuscript, and final approval of the manuscript. All authors agree to be accountable for all aspects of this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a pilot grant from the Leonard Davis Institute for Health Economics, University of Pennsylvania.
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of the University of Pennsylvania (protocol 842862).
Patient consent for publication
Not applicable, as no identifiable or patient-level data are presented.
Informed consent
All subjects in this study were consented prior to participation.
Availability of data and material
Fully deidentified data are available upon request in writing to the corresponding author.
Significance for public health
This research contributes to a better understanding of Americans’ views of government response to the pandemic, which are vital for creating and communicating public health policy. The results of the survey revealed that the most often-practiced prevention practices involved social distancing, and that reactions to federal government policies differed regionally and by political party affiliation. Some of these patterns persisted when the COVID-19 vaccines became available and affect approaches to dealing with COVID-19 in 2022. The burden of COVID-19 tracked with state level policies, reversing the initial trends as states with stricter policies saw morbidity and mortality decrease and the more permissive states experienced sharp increases in disease and death, underscoring the importance of observing public health policies and reactions to them. As noted above, this study offers valuable information for the public health community as they prepare for the next pandemic, or even the next surge of COVID-19 cases.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.