
Abstract
Background:
To examine the impact of cardiac- and noncardiac-related conditions on the risk of hospital complications and 7- and 30-day rehospitalizations in older adult patients with an acute myocardial infarction (AMI).
Methods and Results:
The study population consisted of 3863 adults aged 65 years and older hospitalized with AMI in Worcester, Massachusetts, during six annual periods between 2001 and 2011. Individuals were categorized into four groups based on the presence of 11 previously diagnosed cardiac and noncardiac conditions. The median age of the study population was 79 years and 49% were men. Twenty-eight percent of patients had two or less cardiac- and no noncardiac-related conditions, 21% had two or less cardiac and one or more noncardiac conditions, 20% had three or more cardiac and no noncardiac conditions, and 31% had three or more cardiac and one or more noncardiac conditions. Individuals who presented with one or more noncardiac-related conditions were less likely to have been prescribed evidence-based medications and/or to have undergone coronary revascularization procedures than patients without any noncardiac condition. After multivariable adjustment, individuals with three or more cardiac and one or more noncardiac conditions were at greatest risk for all adverse outcomes.
Conclusions:
Older patients hospitalized with AMI carry a significant burden of cardiac- and noncardiac-related conditions. Older adults who presented with multiple cardiac and noncardiac conditions experienced the worse short-term outcomes and treatment strategies should be developed to improve their in-hospital and post-discharge care and outcomes.
Introduction
Cardiovascular disease (CVD) adversely impacts patient’s quality of life and is the leading cause of morbidity and mortality in American adults. 1 As the US population continues to age, the prevalence of CVD has correspondingly increased, together with other chronic conditions. 2 –4 There is increasing recognition that individuals with CVD and multiple chronic conditions (MCCs) experience higher levels of health-care use and poorer outcomes than patients without MCCs. 4 –10 Despite the high prevalence of MCCs in patients with CVD, there remains uncertainty as to how different combinations and burdens of cardiac and noncardiac conditions impact their in-hospital and post-discharge outcomes, especially in older adults aged 65 years and older.
There is considerable heterogeneity with existing measures of MCCs and none of these are considered to represent a gold standard of disease classification. Some examples of the most commonly used measures include the Charlson and Elixhauser indices, and simple unweighted counts of diagnoses of chronic conditions. 9 –11 Since clinicians treat individual patients and not measures of MCCs, 12 clinicians need simple and efficient approaches/methodologies on how to best assess, manage, and intervene in patients with MCCs and enhance the short- and long-term outcomes of this vulnerable population.
The two major objectives of this large observational study were to (1) describe the magnitude of previously diagnosed cardiac- and noncardiac-related conditions, and hospital management practices, among older adults hospitalized with an independently validated acute myocardial infarction (AMI); and (2) examine the association between the burden of cardiac and noncardiac conditions and the occurrence of clinically significant in-hospital complications and being readmitted to the hospital. Our overarching study hypothesis was that older adults hospitalized with AMI who present with a greater burden of cardiac and noncardiac conditions will be at greater risk for adverse outcomes than those with a lower burden of previously diagnosed chronic conditions. A secondary hypothesis was that patients who presented with one or more noncardiac conditions, in addition to the cardiac-related conditions examined, would be at increased risk for developing adverse outcomes as compared with those who presented with only cardiac-related conditions. Data from the Worcester Heart Attack Study were used for purposes of this investigation. 13 –16
Methods
The Worcester Heart Attack Study is an ongoing population-based investigation that is examining long-term trends in the clinical epidemiology of AMI among residents of the Worcester, Massachusetts, metropolitan area hospitalized at all medical centers in Central Massachusetts on an approximate biennial basis. 13 –17
Computerized printouts of residents of Central Massachusetts admitted to the three largest teaching and community hospitals in the city of Worcester with possible AMI (International Classification of Disease (ICD, see Appendix) 9 codes 410–414, and 786.5) on a biennial basis between 2001 and 2011 were identified. Cases of possible AMI were independently validated using predefined criteria for AMI, including diagnoses of ST segment elevation myocardial infarction (STEMI) and non-ST segment elevation myocardial infarction (NSTEMI). 18,19 This study was approved by the Institutional Review Board at the University of Massachusetts Medical School.
Trained nurses and physicians abstracted information on patient’s demographic and clinical characteristics, hospital treatment practices, and short-term outcomes through the review of hospital medical records. These characteristics included patient’s age, sex, race/ethnicity, hospital length of stay, and 11 previously diagnosed chronic conditions. These 11 previously diagnosed chronic conditions were selected based on their high prevalence in our study cohort. These conditions were defined as those with a frequency equal to or greater than 3% and were further classified into two groups 20 –22 ; seven cardiac-related conditions: atrial fibrillation, diabetes mellitus, heart failure, hyperlipidemia, hypertension, myocardial infarction, and stroke, and four noncardiac-related conditions: anemia, asthma/chronic pulmonary disease, chronic kidney disease (CKD), and depression. Information on the development of clinically significant in-hospital complications including atrial fibrillation, 23 cardiogenic shock, 24 heart failure, 25 stroke, 26 and dying was collected through the review of hospital medical records. Data on the receipt of three coronary diagnostic and interventional procedures (cardiac catheterization, percutaneous coronary intervention (PCI), and coronary artery bypass graft surgery (CABG)) during hospitalization, and evidence-based pharmacotherapies during hospitalization, 19,27,28 namely angiotensin converting enzyme inhibitors (ACE-I)/angiotensin receptor blockers (ARBs), aspirin, beta-blockers, and lipid-lowering agents, were also collected.
For the present study, a rehospitalization was defined as the patient’s first admission to a study hospital for any reason within 7 or 30 days of discharge after their index hospitalization for AMI during the years under study. Two of the study investigators adjudicated whether the principal reason for readmission was due to either an AMI, CVD (excluding AMI)-related, or non-CVD-related readmission based on the review of information contained in hospital medical records. For the present investigation, and due to sample size limitations and ease of data interpretation, we have focused on all-cause hospitalizations. The composite endpoint was defined as the risk of dying or developing any of the examined important clinical complications (heart failure, stroke, cardiogenic shock, or atrial fibrillation) during hospitalization for AMI.
Data analysis
Based on the sample distribution, we stratified our study population into four groups according to the presence of cardiac- or noncardiac-related conditions for purposes of analysis, namely those with two or less cardiac- and no noncardiac-related condition (group 1), two or less cardiac- and one or more noncardiac-related condition (group 2), three or more cardiac- and no noncardiac-related condition (group 3), and three or more cardiac- and one or more noncardiac-related conditions (group 4). We compared differences in the baseline demographic and clinical characteristics, hospital management practices, and development of in-hospital complications and post-discharge hospital readmissions between each of these four groups using χ 2 tests for categorical variables and the analysis of variance test for continuous variables.
For purposes of more systematically examining the association between the number of cardiac and noncardiac conditions previously diagnosed with the risk of dying in hospital, developing clinically important in-hospital complications, or being rehospitalized within 7 or 30 days after the patient’s index hospitalization for AMI, we used logistic regression modeling, adjusting for several potentially confounding demographic and clinical factors of prognostic importance in these models. 29,30 These factors were chosen based on findings from prior studies and on their clinical significance. The variables we controlled for included patient’s age, sex, type of AMI (STEMI vs. NSTEMI), hospital length of stay, receipt of evidence-based cardiac medications during the index hospitalization (ACE-I/ARBs, aspirin, beta-blockers, and lipid-lowering medications), and the receipt of any of the three coronary diagnostic and interventional procedures examined (cardiac catheterization, PCI, and CABG) during the patient’s index hospitalization for AMI. We performed post hoc pairwise comparisons with Bonferroni corrections to examine differences between the four groups included in this study.
Results
A total of 3863 residents of Central Massachusetts 65 years and older were hospitalized with an independently validated AMI at the three largest medical centers in Worcester, Massachusetts, during the six study years between 2001 and 2011. The median age of this patient population was 79 years and 48.9% were men. The four comparison groups in our study included 1084 (28%) patients in group 1, 806 (21%) patients in group 2, 784 (20%) patients in group 3, and 1189 (31%) patients in group 4, respectively.
Baseline patient characteristics according to the presence of cardiac and noncardiac conditions
Patients in group 2 were the oldest (median age 81 years) and were more likely to be female as compared with those in group 1 (Table 1). Patients in group 3 had the lowest proportion of individuals older than 75 years and had the second highest prevalence of patients who developed an NSTEMI as compared with those in group 1 (Table 1). Patients in group 4 were slightly older and were more likely to be female as compared with patients in group 1 (Table 1). Patients in group 4 had the highest prevalence of NSTEMI as compared to the other three groups and together with those in group 2 had the longest length of stay as compared to groups 1 and 3.
Patient characteristics according to categories of cardiac- and noncardiac-related conditions.a

NSTEMI: non-ST segment elevation myocardial infarction; AMI: acute myocardial infarction; CKD: chronic kidney disease.
aGroup 1: two or less cardiac diseases and no noncardiac disease; group 2: two or less cardiac diseases and one or more noncardiac disease; group 3: three or more cardiac diseases and no noncardiac disease; and group 4: three or more cardiac diseases and one or more noncardiac disease.
b p < 0.01.
c p < 0.001.
Frequency of previously diagnosed chronic conditions
The most prevalent chronic conditions among patients in group 1 were hypertension (64%), hyperlipidemia (41%), previous myocardial infarction (25%), and diabetes mellitus (11%) (Table 1). Among patients in group 2, the most prevalent conditions were hypertension (68%), chronic pulmonary disease (42%), depression (36%), and CKD (35%) (Table 1). For those in group 3, the most prevalent conditions were hypertension (96%), hyperlipidemia (80%), diabetes mellitus (63%), and previous myocardial infarction (45%) (Table 1). Among patients in group 4, the most prevalent conditions were hypertension (94%), hyperlipidemia (76%), diabetes mellitus (62%), and heart failure (59%) (Table 1).
In-hospital clinical complications
In the overall study population, heart failure and atrial fibrillation were the most common hospital clinical complications, with the highest incidence in group 4. Approximately one in every two patients, and one in every four patients in group 2, developed heart failure and atrial fibrillation, respectively (Table 1). Similarly, approximately one in every two patients, and one in every three patients in group 3, developed heart failure and atrial fibrillation, respectively, during their index hospitalization (Table 1). Patients in group 4 were at the greatest risk for developing heart failure (68%) and atrial fibrillation (31%) during their index hospitalization for AMI. Groups 2 and 4 had the highest death rate as compared with the other two groups.
Hospital management practices
Patients in group 2 had the lowest proportion of individuals who were treated with ACE-I/ARBs as compared with patients in the other three groups. Patients in group 3 were more likely to have been treated with ACE-I/ARBs and lipid-lowering medications as compared with patients in group 1. Patients in group 4, together with those in group 2, were slightly less likely to have been treated with aspirin and beta-blockers during their acute hospitalization as compared with patients in the other two groups (Table 2).
Clinical management during hospitalization for AMI according to categories of cardiac- and noncardiac-related conditions.a

AMI: acute myocardial infarction; PCI: percutaneous coronary intervention; ACE-I: angiotensin converting enzyme inhibitors; ARBs: angiotensin receptor blockers.
aGroup 1: two or less cardiac diseases and no noncardiac disease; group 2: two or less cardiac diseases and one or more noncardiac disease; group 3: three or more cardiac diseases and no noncardiac disease; and group 4: three or more cardiac diseases and one or more noncardiac disease.
b p < 0.001.
c p < 0.01.
The proportion of patients in groups 2 and 4 who received any diagnostic/interventional procedure was significantly lower as compared with the other two patient groups (Table 2).
Risk of adverse hospital and post-discharge outcomes
After controlling for several potentially confounding demographic and clinical factors of prognostic importance, patients in groups 2, 3, and 4 had an increased risk of dying during hospitalization as compared with those in group 1; the greatest risk for dying was observed among patients in group 4 (Table 3). After performing pairwise comparisons with Bonferroni corrections, these important differences were statistically significant between group 2 and group 1 and between group 4 and group 1 (p < 0.05).
Crude and multivariable adjusted risk of adverse events according to categories of cardiac- and noncardiac-related conditions.a

CI: confidence interval; NSTEMI: non-ST segment elevation myocardial infarction; AMI: acute myocardial infarction; STEMI: ST segment elevation myocardial infarction; PCI: percutaneous coronary intervention; ACE-I: angiotensin converting enzyme inhibitors; ARBs: angiotensin receptor blockers; CABG: coronary artery bypass graft surgery.
aFully adjusted models controlled for age, sex, type of AMI (STEMI/NSTEMI), length of stay, receipt of any of the four medications examined (ACE-I/ARBs, aspirin, beta-blockers, and lipid-lowering medications), and the receipt of any of the three coronary diagnostic and interventional procedures (cardiac catheterization, PCI, and CABG) during the index hospitalization for AMI. Group 1: two or less cardiac diseases and no noncardiac disease; group 2: two or less cardiac diseases and one or more noncardiac disease; group 3: three or more cardiac diseases and no noncardiac disease; and group 4: three or more cardiac diseases and one or more noncardiac disease.
The risk of developing any clinically significant in-hospital complication was increased across all comparison groups, with an increasing trend from group 2 through group 4 (Table 3). After running pairwise comparisons with Bonferroni corrections, our findings suggest that these comparisons were statistically significant between group 2 and group 1, group 3 and group 1, group 4 and group 1, group 4 and group 2, and for patients in group 4 and group 3 (p < 0.05).
The risk for being readmitted to the hospital within 7 days after the patient’s index hospitalization for AMI, according to the presence of cardiac and noncardiac conditions, was slightly higher during this period among patients in groups 2 and 4 as compared with those in group 1, with the highest risk of being readmitted during the subsequent 7 days noted for patients in group 4. Similar trends were found with regard to the risk of readmission within 30 days, with the highest risk noted among patients in group 4 (Table 3). After running pairwise comparisons with Bonferroni corrections, there were no differences between groups in the risk of having a 7-day readmission. On the other hand, when examining 30-day readmissions, the comparisons were statistically significant between group 3 and group 1 and group 4 and group 1 (p < 0.05).
Discussion
In this investigation of more than 3800 patients 65 years and older hospitalized with a confirmed AMI at the three largest tertiary care and community medical centers in Central Massachusetts between 2001 and 2011, patients presented to these hospitals with a considerable burden of cardiac- and noncardiac-related conditions. Moreover, after multivariable adjustment, patients in group 4 (those with the greatest burden of MCCs) had a greater risk for developing each of the adverse outcomes examined compared with patients in the other three groups. Of note, our findings suggest that individuals who presented with a higher burden of cardiac- and noncardiac-related conditions were at greater risk for dying or developing clinically significant complications during their index admission for AMI whereas individuals who presented with any noncardiac-related conditions were at a slightly higher risk of being readmitted to the hospital within 7 days of their index AMI event.
Frequency of individual chronic conditions
Among patients in group 4 (31% of the study cohort), hypertension, hyperlipidemia, diabetes, heart failure, and CKD were highly prevalent; a relatively similar profile of these conditions was observed among patients in group 2 though these individuals also presented with a high prevalence of chronic pulmonary disease and depression.
Our findings share similar patterns to the results of a previous analysis from the Worcester Heart Attack Study which showed a high prevalence of hypertension and diabetes among patients with two or more cardiac comorbidities while the most prevalent noncardiac-related condition was CKD. 31 The present results are also consistent with findings from other contemporary investigations that have studied patients hospitalized with AMI, including a community-based study from Kaiser Permanente Northern California that demonstrated a high burden of hypertension and diabetes in this large HMO population. 32
Differences in hospital management practices according to the presence of previously diagnosed cardiac and noncardiac conditions
We observed relatively small differences across the four groups with regard to the prescribing of in-hospital cardiac medications. Clinical trials of treatments for CVD have usually excluded older adults with a high burden of multimorbidity, which has led to evidence gaps in how to best treat this medically complex, vulnerable population.10 We also found that patients in groups 2 and 4, who were slightly older and sicker than the other comparison groups, were less likely to have undergone coronary revascularization procedures. Thus, there is a clear need for developing evidence-based data to help clinicians care for this group of patients given their MCCs and high risk for adverse clinical outcomes.
Risk of adverse hospital outcomes according to the presence of previously diagnosed cardiac and noncardiac conditions
The individual effects of cardiac- and noncardiac-related conditions on in-hospital complications and 7- and 30-day rehospitalizations in individuals hospitalized with AMI have been studied in a number of prior investigations. 5,9,31,33 In a large study in two major hospitals in Spain of more than 5000 patients hospitalized with AMI between 2003 and 2009, those who presented with heart failure and/or various cardiac arrhythmias were at higher risk for dying during their index hospital admission as compared to those without these chronic conditions. 33 In a prior publication from the Worcester Heart Attack Study, patients with an increasing number of cardiac-related conditions were at greater risk for dying at 30 days and 1 year than those with none or one previously diagnosed cardiac condition. 9
Patients with noncardiac-related conditions have also been shown to be at increased risk for developing adverse outcomes in persons hospitalized with AMI, including patients previously studied in the Worcester Heart Attack Study. 31 Similarly, in a prior publication from the Worcester Heart Attack Study, patients presenting with noncardiac-related conditions were at increased risk for developing adverse outcomes during the index hospitalization for AMI. In a study of more than 3900 patients admitted with AMI to 19 US medical centers between 2003 and 2004, the presence of any noncardiac condition was associated with a five times greater risk of dying during hospitalization as compared to those without any noncardiac condition. 5
The combined effects of cardiac- and noncardiac-related conditions on short-term hospital and post-discharge outcomes in individuals hospitalized with AMI are less well known. In our study of Central Massachusetts residents hospitalized with AMI, individuals who presented with three or more cardiac- and one or more noncardiac-related condition were at the greatest risk for dying during their acute hospitalization, developing clinically significant complications, and for being rehospitalized during the next 30 days. The Swiss AMIS Plus registry of more than 29,600 patients with an acute coronary syndrome examined the burden of multimorbidity, as assessed by the Charlson Comorbidity Index, in relation to the risk of dying during the patient’s index hospitalization. The study investigators reported a two times greater risk of dying during the index hospitalization in individuals with three or more chronic conditions as compared to those without any of the examined chronic conditions. 34 A study of more than 3000 patients who were hospitalized in Olmsted County, Minnesota, with a first-ever AMI between 1987 and 2010 and who presented with diabetes, chronic obstructive pulmonary disease, or anemia were at higher risk for being readmitted to the hospital within 30 days as compared to those without these chronic conditions. In a study of more than 3000 patients admitted to the hospital with an incident AMI in Olmsted County, Minnesota, between 1987 and 2010, researchers reported that the presence of diabetes, chronic pulmonary disease or anemia was associated with higher risk for being readmitted to the hospital within 30 days as compared to those without these chronic conditions. 35
We found that individuals with one or more noncardiac-related condition (groups 2 and 4), in addition to any cardiac condition, experienced a slightly higher risk of being rehospitalized over the subsequent 7 days as compared with patients in group 1. These findings provide further supportive evidence that the presence of noncardiac-related conditions including CKD, chronic pulmonary disease, anemia, and depression should be carefully considered and monitored when managing patients recently admitted to the hospital with an AMI.
Clinical implications
The present study expands upon previous work by studying not only the individual but also the combined effects of several previously diagnosed cardiac and noncardiac conditions in patients hospitalized with an AMI. Our results indicate that cardiac and noncardiac conditions are common in individuals hospitalized with AMI and have important prognostic implications. The presence of these cardiac- and noncardiac-related conditions increases the challenges for health-care providers due to the complexity of the interaction between diseases, diseases and medical treatments, and between various cardiac and noncardiac medications.25 Since clinical guidelines and disease management programs typically focus on patients with single conditions, and clinical research often excludes persons with MCCs, our observation that patients with several cardiac or noncardiac conditions were significantly more likely to have experienced adverse hospital and post-discharge outcomes suggests that current clinical guidelines need to take into consideration these high-risk patients.
Study strengths and limitations
The strengths of the present study include its community-based design, its large sample of patients hospitalized with AMI, and its relatively contemporary perspective in examining clinically relevant outcomes and hospital treatment practices according to the frequency of a number of important cardiac and noncardiac conditions. There was comprehensive ascertainment of cardiac- and noncardiac-related conditions, death, in-hospital complications, and post-discharge hospitalizations. Several limitations need to be acknowledged, however, in the interpretation of the present findings. First, since our study population included only patients who had been hospitalized in the Worcester metropolitan area, one needs to be careful to extrapolate our findings to those who reside in other geographic areas. Second, since the majority of the study patients were White, the generalizability of our findings to other race/ethnic groups may be limited. There is the potential for unmeasured confounding since we did not have information available on several patient-associated characteristics, such as income, education, psychosocial factors, body mass index, or smoking status, that may have affected several of the endpoints examined. Finally, detailed information about the duration or severity of the chronic conditions studied was unavailable.
Conclusions
The findings of our investigation suggest that cardiac- and noncardiac-related conditions are highly prevalent in patients 65 years of age and older hospitalized with AMI and individuals presenting with both types of chronic conditions are at greatest risk for developing adverse in-hospital and short-term outcomes. We observed that individuals who presented with one or more noncardiac-related condition were less likely to have been prescribed evidence-based medications and/or undergone coronary revascularization procedures than patients without any noncardiac condition. Due to the extremely limited published evidence that exists to guide the treatment of this vulnerable population, there is a clear need for developing guidelines that might help health-care providers caring for these patients. Future research should also examine the impact of cardiac- and noncardiac-related conditions on important long-term clinical and patient-centered outcomes in patients hospitalized with AMI that will help clinicians, caregivers, and patients in discussions about the management and prognosis of patients with these chronic conditions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant support for this project was provided by the National Heart, Lung, and Blood Institute (RO1 HL35434). Drs Gore, Goldberg, and Yarzebski’s effort was supported in part by funding from the National Heart, Lung and Blood Institute (U01HL105268). Drs Tisminetzky and Gurwitz were supported by grants from the National Institute on Aging (R24AG045050 and R33AG057806).
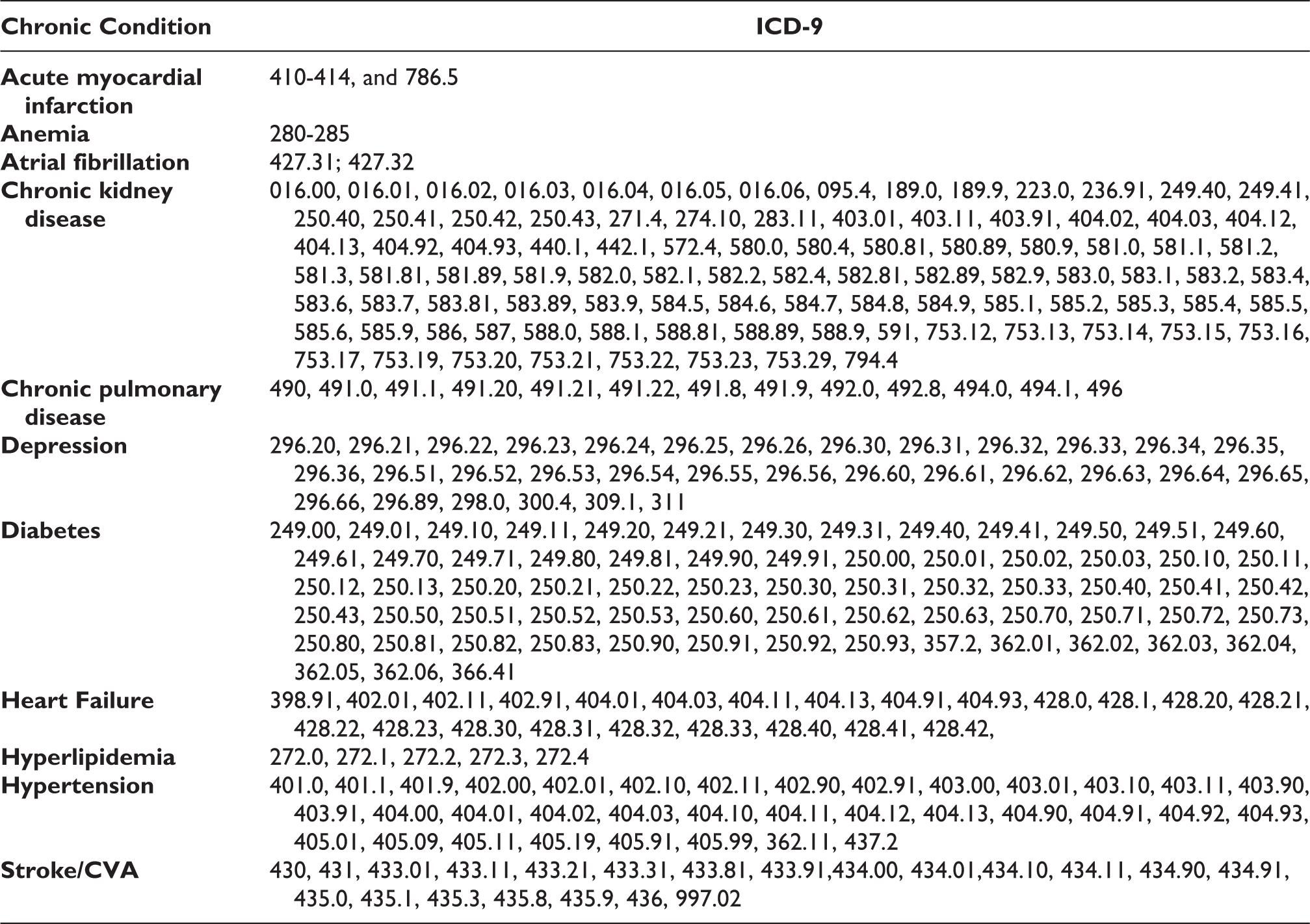
Appendix: ICD-9 Chronic Conditions Codes
|
|
|
|---|---|
|
|
410-414, and 786.5 |
|
|
280-285 |
|
|
427.31; 427.32 |
|
|
016.00, 016.01, 016.02, 016.03, 016.04, 016.05, 016.06, 095.4, 189.0, 189.9, 223.0, 236.91, 249.40, 249.41, 250.40, 250.41, 250.42, 250.43, 271.4, 274.10, 283.11, 403.01, 403.11, 403.91, 404.02, 404.03, 404.12, 404.13, 404.92, 404.93, 440.1, 442.1, 572.4, 580.0, 580.4, 580.81, 580.89, 580.9, 581.0, 581.1, 581.2, 581.3, 581.81, 581.89, 581.9, 582.0, 582.1, 582.2, 582.4, 582.81, 582.89, 582.9, 583.0, 583.1, 583.2, 583.4, 583.6, 583.7, 583.81, 583.89, 583.9, 584.5, 584.6, 584.7, 584.8, 584.9, 585.1, 585.2, 585.3, 585.4, 585.5, 585.6, 585.9, 586, 587, 588.0, 588.1, 588.81, 588.89, 588.9, 591, 753.12, 753.13, 753.14, 753.15, 753.16, 753.17, 753.19, 753.20, 753.21, 753.22, 753.23, 753.29, 794.4 |
|
|
490, 491.0, 491.1, 491.20, 491.21, 491.22, 491.8, 491.9, 492.0, 492.8, 494.0, 494.1, 496 |
|
|
296.20, 296.21, 296.22, 296.23, 296.24, 296.25, 296.26, 296.30, 296.31, 296.32, 296.33, 296.34, 296.35, 296.36, 296.51, 296.52, 296.53, 296.54, 296.55, 296.56, 296.60, 296.61, 296.62, 296.63, 296.64, 296.65, 296.66, 296.89, 298.0, 300.4, 309.1, 311 |
|
|
249.00, 249.01, 249.10, 249.11, 249.20, 249.21, 249.30, 249.31, 249.40, 249.41, 249.50, 249.51, 249.60, 249.61, 249.70, 249.71, 249.80, 249.81, 249.90, 249.91, 250.00, 250.01, 250.02, 250.03, 250.10, 250.11, 250.12, 250.13, 250.20, 250.21, 250.22, 250.23, 250.30, 250.31, 250.32, 250.33, 250.40, 250.41, 250.42, 250.43, 250.50, 250.51, 250.52, 250.53, 250.60, 250.61, 250.62, 250.63, 250.70, 250.71, 250.72, 250.73, 250.80, 250.81, 250.82, 250.83, 250.90, 250.91, 250.92, 250.93, 357.2, 362.01, 362.02, 362.03, 362.04, 362.05, 362.06, 366.41 |
|
|
398.91, 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, 428.0, 428.1, 428.20, 428.21, 428.22, 428.23, 428.30, 428.31, 428.32, 428.33, 428.40, 428.41, 428.42, |
|
|
272.0, 272.1, 272.2, 272.3, 272.4 |
|
|
401.0, 401.1, 401.9, 402.00, 402.01, 402.10, 402.11, 402.90, 402.91, 403.00, 403.01, 403.10, 403.11, 403.90, 403.91, 404.00, 404.01, 404.02, 404.03, 404.10, 404.11, 404.12, 404.13, 404.90, 404.91, 404.92, 404.93, 405.01, 405.09, 405.11, 405.19, 405.91, 405.99, 362.11, 437.2 |
|
|
430, 431, 433.01, 433.11, 433.21, 433.31, 433.81, 433.91,434.00, 434.01,434.10, 434.11, 434.90, 434.91, 435.0, 435.1, 435.3, 435.8, 435.9, 436, 997.02 |